

Volume 6, Issue 2 (6-2021)
CJHR 2021, 6(2): 47-56 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mohammadian S, Asgari P, Makvandi B, Naderi F. Effects of Schema Therapy on Anxiety, Cognitive Avoidance, and Resilience in Couples With Conflicts. CJHR 2021; 6 (2) :47-56
URL: http://cjhr.gums.ac.ir/article-1-188-en.html
URL: http://cjhr.gums.ac.ir/article-1-188-en.html



1- Department of Psychology, Ahvaz Branch, Islamic Azad University, Ahvaz, Iran.
2- Department of Psychology, Ahvaz Branch, Islamic Azad University, Ahvaz, Iran. , paskarii45@gmail.com
2- Department of Psychology, Ahvaz Branch, Islamic Azad University, Ahvaz, Iran. , paskarii45@gmail.com
Full-Text [PDF 621 kb]
(593 Downloads)
| Abstract (HTML) (1142 Views)
Full-Text: (1052 Views)
1. Introduction
As an essential institution of society, the family can shape individuals’ personalities. The prosperity, growth, and development of family members can be greatly influenced by desirability, satisfaction, gratification, quality, and optimal functioning of the family; the interaction of which seems to play a crucial role in marriage success and stability [1]. Low Quality of Life (QoL) is a painful condition of biopsychological and emotional exhaustion; it can affect those who expect dream love and marriage to give meaning to their lives; it occurs when individuals realize that their relationship failed to provide any meaning to the life despite their best efforts [2]. In its worst situation, low marital quality equals relationship breakdown [3, 4].
Anxiety is a common problem among couples and can affect their marital QoL [5, 6]. Anxiety is a normal response to threatening situations. Anxiety is a warning sign that informs of imminent danger, preparing the subject for confrontation. In general, anxiety is a generalized unpleasant and often vague feeling, i.e., accompanied by one or more physical feelings, such as heart drop, chest tightness, palpitation, sweating, headache, and so on. Almost all individuals have experienced some symptoms of anxiety in their life [7, 8]. These groups permanently feel fear and concern for no specific reason. Besides, there is no logical correlation between the severity of fear and threat to them. Fear and concern can lead to displeasure in these individuals and disable them to continue their life, keep the job, and build long-term relationships with friends and family [9, 10]. Sbarra et al. [11] argued that anxiety is a predictor of increased divorce or separation.
An important part of research concerning marital conflicts and marital dissatisfaction has focused on emotional and cognitive characteristics, such as problems related to recognition, management, evaluation, and the monitoring of emotions in a mutual relationship of spouses [12]. Cognitive avoidance seems to affect couples’ relationships. Cognitive avoidance refers to various strategies for modifying individuals’ attitudes in social situations [13]. It entails actions aimed at denying or downplaying the crisis and its consequences, or accepting the situation, as it cannot be changed. Rumination, catastrophizing, re-evaluation, and re-focus on plans are all examples of cognitive avoidance [14]. Holaway et al. [15] revealed that cognitive avoidance plays an essential role in reducing the QoL and developing mental health disorders. Other studies indicated a significant relationship between cognitive avoidance and mental health [16, 17].
As a variable affecting couples’ relationships and conflicts, resilience in marital relationships has gained much attention in family psychology and family therapy; it is addressed to relieve tension and conflicts and their adverse effects. Resilience refers to the ability of an individual to adapt to and overcome disasters or severe pressures and even to be strengthened by these experiences [18]. This is a positive trait, i.e., supported, developed, and appeared by individuals’ inner ability and social skills, as well as their interaction with the environment. Low levels of resilience in the family environment and couples’ relationships may result in conflicts [19]. Numerous studies highlighted the relationship between resilience in couples’ lives and their happiness. This is because resilience is among the main structures of personality conceptualized for understanding motivation, excitement, and behaviors. Tensions and traumatic events cannot be resolved in marital life if resilience is impaired [20, 21]. The lack of resilience can lead to negative experiences as well as incompatibility, low tolerance, and maladaptation with stressful environmental conditions; ultimately, it may disrupt mental health [22].
Schema therapy is currently used for treating various marital problems. A large body of literature suggested the effectiveness of schema therapy, especially in the forms of couple therapy and group therapy. Recent studies reported that schema therapy is more effective than other approaches [23, 24]. This approach can address problems overlooked by other cognitive approaches, such as inefficient patterns in intimate relationships and altering trouble-making childhood memories [25, 26]. Mainly, schema therapy aims at identifying early maladaptive schemas; validate inappropriate emotional needs; change dysfunctional beliefs and maladaptive schemas to improve performance; change lifestyle patterns and maladaptive coping styles, and facilitate learning adaptive skills [27]. Dattilio [28] stated that schema therapy can affect marital intimacy and its components. Mohammadi et al. [29] reported that schema therapy plays an improving effect on early maladaptive schemas and conflict resolution patterns. Accordingly, the present study aimed to investigate the effects of schema therapy on anxiety, cognitive avoidance, and resilience among couples with low marital adjustment.
2. Materials and Methods
This was a quasi-experimental study with a pre-test, post-test, follow-up and a control group design. The study population consisted of all married individuals with low marital adjustment who were referred to the counseling and psychological centers of Ahvaz City, Iran in 2020. Using a convenience sampling method, 30 couples were selected and randomly divided into the experimental and control groups (n=15 couples/group). Randomization was performed by the author and the study participants were assigned to the groups by tossing coins. The inclusion criteria were as follow: obtaining a score lower than the cut-off point in the marital adjustment test, the age of 25-45 years, experiencing more than two years of marital life, and not receiving medications and any interventions during the research. The exclusion criteria were the occurrence of stressful events, such as divorce and the death of relatives, and absence from >2 treatment sessions. The following tools were used to collect the required data:
The Connor-Davidson Resilience Scale (CD-RISC; 2003): Connor and Davidson developed this scale in 2003 to assess resilience. This 25-item questionnaire is scored based on a 5-point Likert-type scale, ranging from zero (strongly disagree) to 4 (strongly agree). The CD-RISC aims to assess resilience in individuals. The total score of the scale is obtained by summing the scores of all items and ranges from zero to 100. The greater score indicated better resilience. The cut-off point of this scale equals 50. In other words, scores higher than 50 indicate resilience in the individual, and the higher than 50 the score is, the greater the individual’s resilience level [30]. In this study, the Persian version of the scale was used. The psychometric properties of the Persian version of this scale were confirmed by Keyhani and associates [31]. Badie et al. [32] reported a Cronbach alpha coefficient of 0.85 for the scale. In the present study, Cronbach’s alpha coefficient was obtained as 0.82 for the scale.
Cognitive Avoidance Questionnaire (CAQ): The CAQ is a self-report scale developed by Sexton and Dugas [33]. It consists of 25 items that aim to measure cognitive avoidance from various aspects (the appeasement of anxious thoughts, the substitution of anxious thoughts with positive ones, using distraction to interrupt the process of worrying, avoiding situations and activities that activate anxious thoughts, and turning mental images into verbal thoughts). It is scored on a 5-point Likert-type scale, ranging from very untrue=1 to very true=5. The total score is obtained by adding the scores of each item, ranging between 25 and 125. Lower scores indicate low cognitive avoidance and higher scores represent greater cognitive avoidance. Besharat and Mirjalili [34] confirmed the psychometric properties of the Persian version of this questionnaire. Aghajani et al. [35] reported a Cronbach alpha coefficient of 0.86 for the questionnaire. In the present study, Cronbach’s alpha coefficient was calculated as 0.79 for the questionnaire.
The Symptom CheckList-90- Revised (SCL-90-R): The SCL-90-R, developed by Derogatis, is a self-report tool that includes 90 items. The SCL-90-R is designed to measure 9 current psychiatric symptoms, as well as psychological distress. The subscales of SCL-90-R assess the following psychiatric symptoms: obsessive-compulsive disorder, somatization, depression, interpersonal sensitivity, hostility, anxiety, paranoid ideation, phobic anxiety, and psychoticism. The items are scored based on a 5-point Likert-type scale, ranging from 0 to 4. Each item has 5 following response categories: 0=not at all, 1=low, 2=moderate, 3=high, 4=severe [36]. In the present study, the Persian version of the questionnaire was used. The psychometric properties of the Persian version of SCL-90-R were confirmed by Akhavan Abiri and Shairi [37]. In the present study, Cronbach’s alpha coefficient was computed as 0.87 for the scale.
The study participants were selected from referrals to counseling and psychology clinics in Ahvaz City, Iran, with low marital adjustment and high intrapersonal problems. Following the necessary examinations, 30 eligible couples were selected to participate in the study. After selecting the research participants, the experimental group received 10 group-based schema therapy sessions (90-minute weekly sessions). The control group received no treatment. In the last session of the schema therapy program, a post-test was performed in the experimental and control groups. The follow-up phase was performed after 45 days. In the present study, the mean scores of the research variables per couple were calculated. Then, the mean score was obtained from the relevant values. For ethical considerations, the researchers received written informed consent forms from the study participants. The study was approved by the Ethics Committee of Islamic Azad University, Ahvaz Branch (Code: IR.IAU.AHVAZ.REC.1399.019).
The schema therapy sessions were performed once a week based on the schema therapy package of Young and associates [38]. A summary of the provided schema therapy sessions is presented in Table 1.
.png)
The obtained data were analyzed by descriptive (mean, standard deviation) and inferential statistics, including repeated-measures Analysis of Variance (ANOVA). The Bonferroni posthoc test was employed to investigate differences in the mean scores of anxiety, cognitive avoidance, and resilience between the pre-test, post-test, and follow-up steps. SPSS was used for analyzing the collected data. The significance level was set at P<0.05.
3. Results
The study participants included 60 subjects (30 couples) visiting Ahvaz counseling centers, aged 25-45 years. The demographic characteristics of the explored couples are listed in Table 2.
.png)
Table 3 presents the group-wise pre-test, post-test, and follow-up Mean±SD scores of anxiety, cognitive avoidance, and resilience among the examined couples.
.png)
The baseline values of anxiety, cognitive avoidance, and resilience were considered as covariates. The calculated correlation coefficients ranged between 0.09 (P>0.05) and 0.10 (P>0.05). According to the obtained correlations, the multicollinearity assumption was established between auxiliary variables (covariates). In this study, Levene’s test of equality of variances was used to examine the homogeneity of variances. The F-value calculated in Levene’s test was not significant respecting anxiety, cognitive avoidance, and resilience in the pre-test, post-test, and follow-up phases; therefore, there was no significant difference in error variances between the experimental and control groups.
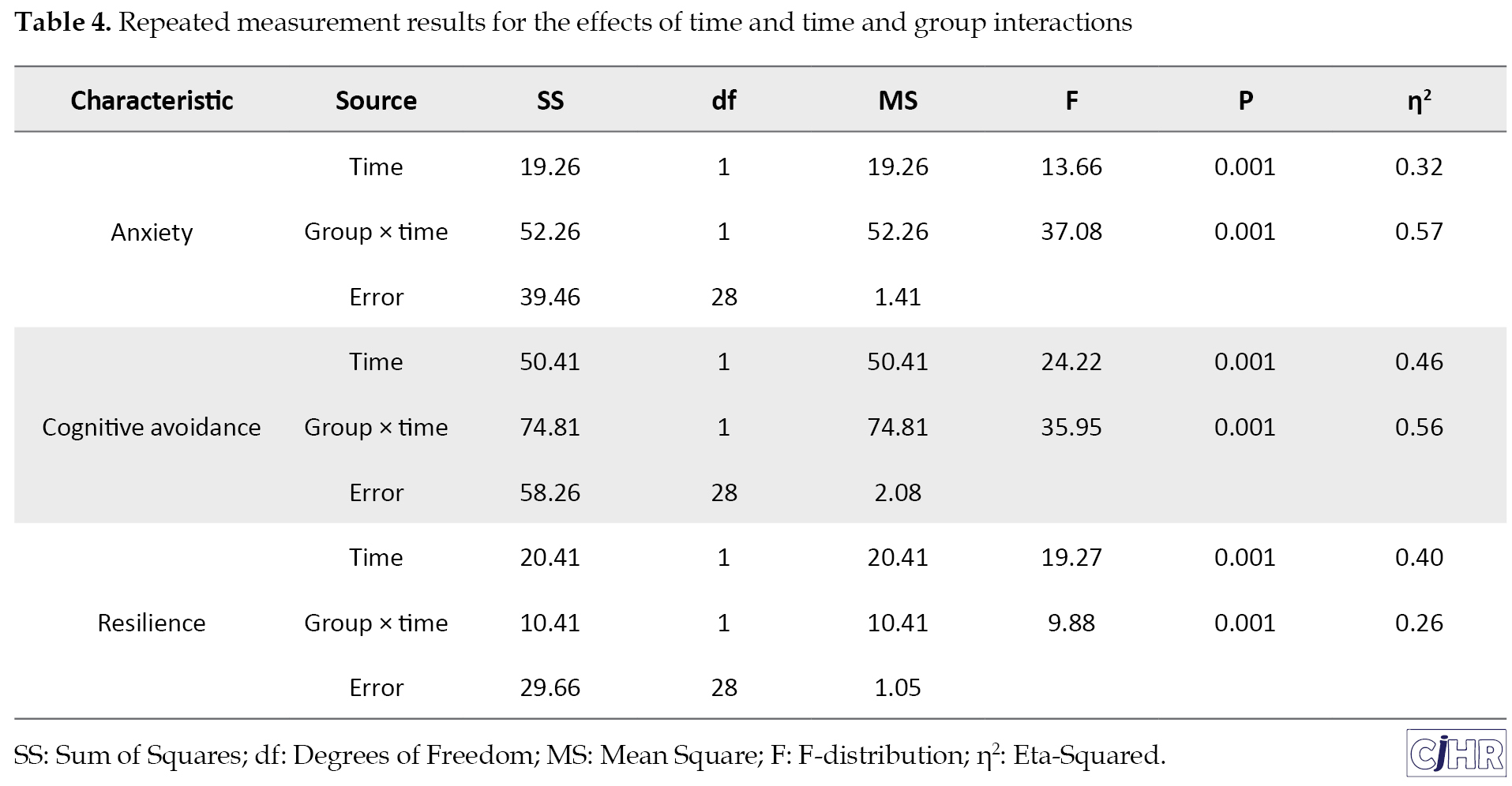
Based on the results of within groups analysis, there was a significant difference in the mean scores of anxiety, cognitive avoidance, and resilience between the pre-test, post-test, and follow-up phases in the intervention group (P<0.001). Furthermore, 32% of the differences in anxiety, 46% in cognitive avoidance, and 40% in resilience were due to the interaction of the effect of the pre-test, post-test, and follow-up steps. Based on the results of the between-groups analysis, the mean scores of anxiety, cognitive avoidance, and resilience significantly differed in the experimental group (schema therapy) and the control group (P<0.001). Additionally, 57% of the differences in anxiety, 56% in cognitive avoidance, and 26% in resilience were due to group × time interaction effects (Table 4).
The results of the Bonferroni posthoc test for comparing the research groups are presented in Table 5.
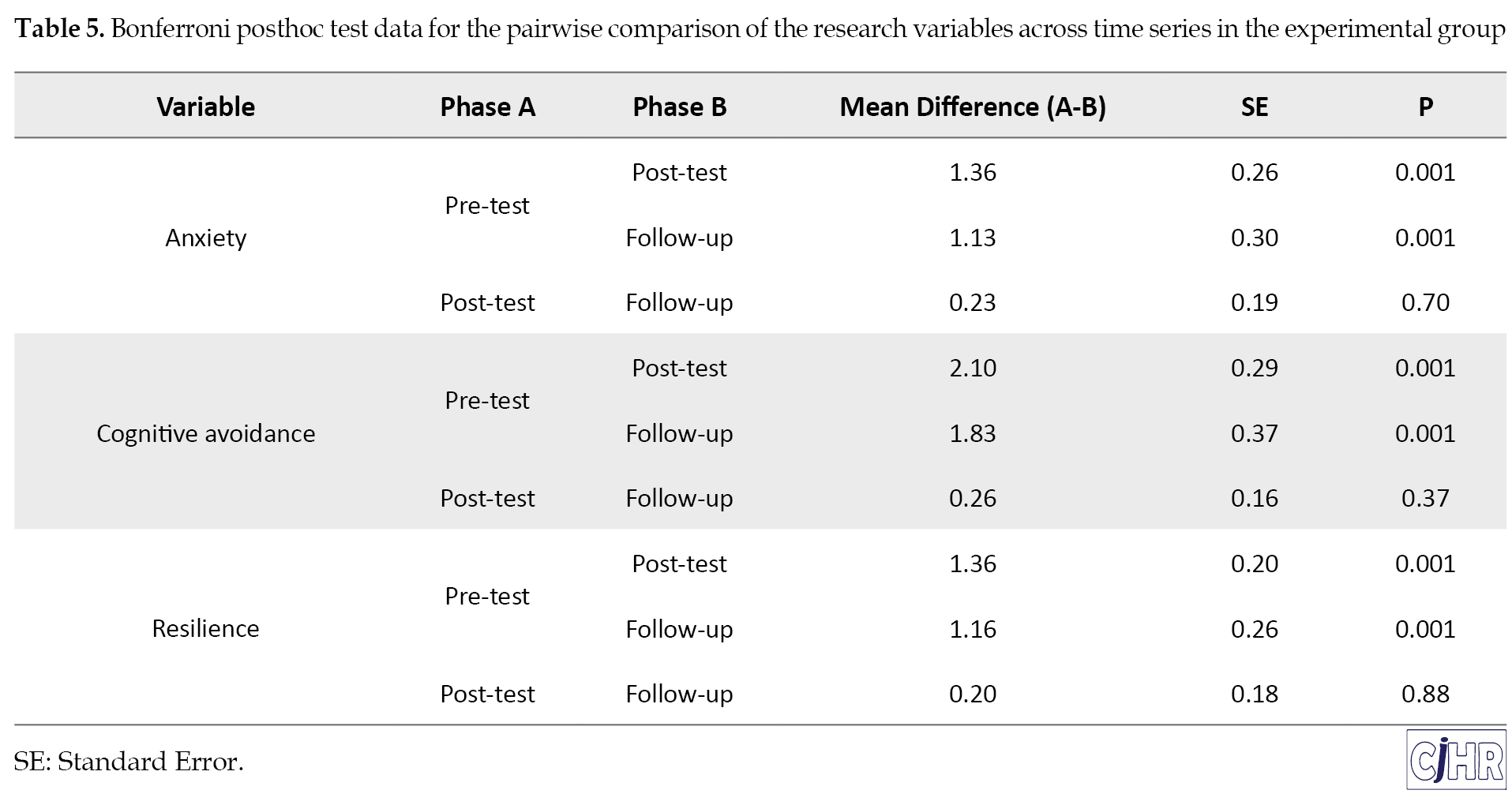
According to the relevant results, there was a significant difference between the pre-test and post-test scores in anxiety, cognitive avoidance, and resilience (P<0.001). There was also a significant difference between pre-test and follow-up values in research variables (P<0.001). In other words, the stability of the intervention was confirmed for all variables. Moreover, comparing post-test and follow-up scores of the study variables revealed no significant difference (P>0.05).
4. Discussion
The present study investigated the effects of schema therapy on anxiety, cognitive avoidance, and resilience in couples visiting Ahvaz counseling centers in 2020. The obtained results indicated that schema therapy effectively decreased anxiety and cognitive avoidance and increased resilience in the experimental group. This finding was consistent with those of Dattilio [28] and Mohammadi et al. [29]. By taking advantage of experimental techniques, which reconstruct childhood cognition and memories, schema therapy can greatly help the expression of suppressed emotions; finally, it may result in emotional self-censorship, difficulty in the expression of emotions, and emotional coldness. Schema therapy establishes a good relationship between the past and the present. According to Young et al. [38], schema therapy can effectively treat psychological problems. This is because it combines cognitive, behavioral, interpersonal, and experimental techniques for evaluating schemas; thus, schema therapy can improve anxiety by emphasizing the roots of problems and transformational processes involved in creating and maintaining schemas. Anxiety can reduce couples’ self-esteem; consequently, it might impair a family’s mental health status. Anxiety is a generalized, unpleasant, and often vague feeling of concern that signals a sudden and imminent danger, preparing individuals to face the threat [23]. Modifying and adjusting them through psychological training, like schema therapy, can play an effective role in the destructive actions of individuals. This is because emotions act as solutions to cope with challenges, stress, and problems of life. In other words, emotions play an essential role in life. Accordingly, teaching these techniques to individuals with marital conflicts, to regulate emotions as a healing method for modifying emotions, is associated with acceptance and positive social interaction. Eventually, this process results in effective coping with the challenging and stressful situations of marital life and increases participation in responding to social situations [25]. Therefore, by informing individuals of their positive and negative emotions to accept and express them promptly, schema therapy can significantly reduce destructive behaviors and increase positive behaviors.
Cognitive avoidance is a manner that couples choose for facing social events and interpersonal relationships to respond to stressful situations. Based on this strategy, individuals change their minds during social relations. Various strategies are employed in cognitive avoidance, including intentional attempts to suppress thought, thought substitution, the avoidance of frightening stimuli, distraction, and turning imagination into thought [26]. These strategies are used to divert the mind from worrying topics to other ones. Schema therapy facilitates change through working on the individual’s multifaceted dimensions, including cognitive, experimental, emotional, and behavioral aspects. In the cognitive dimension, schema therapy focuses on the internalized voice of parents and the deepest emotional level, i.e., schemas; thus, it helps couples who are unhappy with their marital life find the roots of their emotions to question the schema and its resulting emotions. It also helps them to foster a new perspective on marital relationships by examining the schema’s correctness and finding a new definition for the schema approving or disproving evidence. Individuals emphasize information, i.e., consistent with the schema, and ignore the inconsistent data. They continue this process in their marital relationships and can observe the direct effect of the schema on marital relationships [27]. Schema therapy, as a summary of the individual’s healthy responses and the identification of the schema roots and inefficient thoughts, is the most beneficial tool for an individual to identify the schema motivating situations, to diagnose negative behaviors, and to replace healthy behaviors in marital relationships; accordingly, this method informs the individual about schemas and facilitates change in them, and consequently in the couple’s relationship.
Spouses require a high level of resilience in their marital life. This is because of the perception of their psychological challenges, conflicts, and stressful living conditions. They have an analytical-critical mentality about their abilities and circumstances; they reflect on abilities and circumstances. They are resilient in different situations and have a wonderful imagination (thinking power) about the solutions. Resilience refers to return to the original balance or reaching a higher level of balance. Therefore, it provides a successful adaptation in life. Positive adaptation with life not only can be a consequence of resilience but also can lead to a higher level of resilience. Schema-based approaches are useful in modifying the beliefs and thoughts of individuals with a desire for divorce; they can reduce the desire for divorce, as they work on psychological themes or early maladaptive schemas [39]. In the emotional dimension, schema therapy uses experimental strategies to challenge the cognitive belief, i.e., tied to emotional belief to make the couples fight their schemas in the treatment session at the cognitive and emotional levels [24]. This technique helps the couples to express their emotions in marital relationships; accordingly, they can recognize their unknown emotional needs that have led to the formation of maladaptive schemas. An interesting technique of experimental strategy, namely writing a letter to the spouse, helps the individual to use it as an opportunity to realize the rights, feelings, unexpressed anger, and the expression of beliefs that seem to cause a problem in the couple’s communication pattern.
A limitation of the present study was that this approach was applied to both married men and women and the researcher was unable to establish separate gender-wise groups. It is suggested that researchers examine the effectiveness of this approach on other aspects of marital life.
5. Conclusion
Schema therapy decreased anxiety, cognitive avoidance, and increased resilience in the explored couples with marital conflicts. Schema therapy can be used to improve resilience in couples involved in marital conflicts. Given the results obtained in this study, therapists and counselors are recommended to use schema therapy to improve marital variables.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the Islamic Azad University, Ahvaz Branch (Code: IR.IAU.AHVAZ.REC.1399.019).
Funding
This article was extracted from the PhD. dissertation of the first author at the Department of Psychology, Ahvaz Branch, Islamic Azad University, Ahvaz.
Authors' contributions
Conceptualization and supervision: Shabnam Mohammadian, Parviz Asgari; Methodology: Shabnam Mohammadian, Behnam Makvandi; Investigation, writing–review & editing: Parviz Asgari, Farah Naderi; Writing – original draft and funding acquisition, resources: Shabnam Mohammadian, Parviz Asgari.
Conflict of interest
The authors declared no conflicts of interest.
References
As an essential institution of society, the family can shape individuals’ personalities. The prosperity, growth, and development of family members can be greatly influenced by desirability, satisfaction, gratification, quality, and optimal functioning of the family; the interaction of which seems to play a crucial role in marriage success and stability [1]. Low Quality of Life (QoL) is a painful condition of biopsychological and emotional exhaustion; it can affect those who expect dream love and marriage to give meaning to their lives; it occurs when individuals realize that their relationship failed to provide any meaning to the life despite their best efforts [2]. In its worst situation, low marital quality equals relationship breakdown [3, 4].
Anxiety is a common problem among couples and can affect their marital QoL [5, 6]. Anxiety is a normal response to threatening situations. Anxiety is a warning sign that informs of imminent danger, preparing the subject for confrontation. In general, anxiety is a generalized unpleasant and often vague feeling, i.e., accompanied by one or more physical feelings, such as heart drop, chest tightness, palpitation, sweating, headache, and so on. Almost all individuals have experienced some symptoms of anxiety in their life [7, 8]. These groups permanently feel fear and concern for no specific reason. Besides, there is no logical correlation between the severity of fear and threat to them. Fear and concern can lead to displeasure in these individuals and disable them to continue their life, keep the job, and build long-term relationships with friends and family [9, 10]. Sbarra et al. [11] argued that anxiety is a predictor of increased divorce or separation.
An important part of research concerning marital conflicts and marital dissatisfaction has focused on emotional and cognitive characteristics, such as problems related to recognition, management, evaluation, and the monitoring of emotions in a mutual relationship of spouses [12]. Cognitive avoidance seems to affect couples’ relationships. Cognitive avoidance refers to various strategies for modifying individuals’ attitudes in social situations [13]. It entails actions aimed at denying or downplaying the crisis and its consequences, or accepting the situation, as it cannot be changed. Rumination, catastrophizing, re-evaluation, and re-focus on plans are all examples of cognitive avoidance [14]. Holaway et al. [15] revealed that cognitive avoidance plays an essential role in reducing the QoL and developing mental health disorders. Other studies indicated a significant relationship between cognitive avoidance and mental health [16, 17].
As a variable affecting couples’ relationships and conflicts, resilience in marital relationships has gained much attention in family psychology and family therapy; it is addressed to relieve tension and conflicts and their adverse effects. Resilience refers to the ability of an individual to adapt to and overcome disasters or severe pressures and even to be strengthened by these experiences [18]. This is a positive trait, i.e., supported, developed, and appeared by individuals’ inner ability and social skills, as well as their interaction with the environment. Low levels of resilience in the family environment and couples’ relationships may result in conflicts [19]. Numerous studies highlighted the relationship between resilience in couples’ lives and their happiness. This is because resilience is among the main structures of personality conceptualized for understanding motivation, excitement, and behaviors. Tensions and traumatic events cannot be resolved in marital life if resilience is impaired [20, 21]. The lack of resilience can lead to negative experiences as well as incompatibility, low tolerance, and maladaptation with stressful environmental conditions; ultimately, it may disrupt mental health [22].
Schema therapy is currently used for treating various marital problems. A large body of literature suggested the effectiveness of schema therapy, especially in the forms of couple therapy and group therapy. Recent studies reported that schema therapy is more effective than other approaches [23, 24]. This approach can address problems overlooked by other cognitive approaches, such as inefficient patterns in intimate relationships and altering trouble-making childhood memories [25, 26]. Mainly, schema therapy aims at identifying early maladaptive schemas; validate inappropriate emotional needs; change dysfunctional beliefs and maladaptive schemas to improve performance; change lifestyle patterns and maladaptive coping styles, and facilitate learning adaptive skills [27]. Dattilio [28] stated that schema therapy can affect marital intimacy and its components. Mohammadi et al. [29] reported that schema therapy plays an improving effect on early maladaptive schemas and conflict resolution patterns. Accordingly, the present study aimed to investigate the effects of schema therapy on anxiety, cognitive avoidance, and resilience among couples with low marital adjustment.
2. Materials and Methods
This was a quasi-experimental study with a pre-test, post-test, follow-up and a control group design. The study population consisted of all married individuals with low marital adjustment who were referred to the counseling and psychological centers of Ahvaz City, Iran in 2020. Using a convenience sampling method, 30 couples were selected and randomly divided into the experimental and control groups (n=15 couples/group). Randomization was performed by the author and the study participants were assigned to the groups by tossing coins. The inclusion criteria were as follow: obtaining a score lower than the cut-off point in the marital adjustment test, the age of 25-45 years, experiencing more than two years of marital life, and not receiving medications and any interventions during the research. The exclusion criteria were the occurrence of stressful events, such as divorce and the death of relatives, and absence from >2 treatment sessions. The following tools were used to collect the required data:
The Connor-Davidson Resilience Scale (CD-RISC; 2003): Connor and Davidson developed this scale in 2003 to assess resilience. This 25-item questionnaire is scored based on a 5-point Likert-type scale, ranging from zero (strongly disagree) to 4 (strongly agree). The CD-RISC aims to assess resilience in individuals. The total score of the scale is obtained by summing the scores of all items and ranges from zero to 100. The greater score indicated better resilience. The cut-off point of this scale equals 50. In other words, scores higher than 50 indicate resilience in the individual, and the higher than 50 the score is, the greater the individual’s resilience level [30]. In this study, the Persian version of the scale was used. The psychometric properties of the Persian version of this scale were confirmed by Keyhani and associates [31]. Badie et al. [32] reported a Cronbach alpha coefficient of 0.85 for the scale. In the present study, Cronbach’s alpha coefficient was obtained as 0.82 for the scale.
Cognitive Avoidance Questionnaire (CAQ): The CAQ is a self-report scale developed by Sexton and Dugas [33]. It consists of 25 items that aim to measure cognitive avoidance from various aspects (the appeasement of anxious thoughts, the substitution of anxious thoughts with positive ones, using distraction to interrupt the process of worrying, avoiding situations and activities that activate anxious thoughts, and turning mental images into verbal thoughts). It is scored on a 5-point Likert-type scale, ranging from very untrue=1 to very true=5. The total score is obtained by adding the scores of each item, ranging between 25 and 125. Lower scores indicate low cognitive avoidance and higher scores represent greater cognitive avoidance. Besharat and Mirjalili [34] confirmed the psychometric properties of the Persian version of this questionnaire. Aghajani et al. [35] reported a Cronbach alpha coefficient of 0.86 for the questionnaire. In the present study, Cronbach’s alpha coefficient was calculated as 0.79 for the questionnaire.
The Symptom CheckList-90- Revised (SCL-90-R): The SCL-90-R, developed by Derogatis, is a self-report tool that includes 90 items. The SCL-90-R is designed to measure 9 current psychiatric symptoms, as well as psychological distress. The subscales of SCL-90-R assess the following psychiatric symptoms: obsessive-compulsive disorder, somatization, depression, interpersonal sensitivity, hostility, anxiety, paranoid ideation, phobic anxiety, and psychoticism. The items are scored based on a 5-point Likert-type scale, ranging from 0 to 4. Each item has 5 following response categories: 0=not at all, 1=low, 2=moderate, 3=high, 4=severe [36]. In the present study, the Persian version of the questionnaire was used. The psychometric properties of the Persian version of SCL-90-R were confirmed by Akhavan Abiri and Shairi [37]. In the present study, Cronbach’s alpha coefficient was computed as 0.87 for the scale.
The study participants were selected from referrals to counseling and psychology clinics in Ahvaz City, Iran, with low marital adjustment and high intrapersonal problems. Following the necessary examinations, 30 eligible couples were selected to participate in the study. After selecting the research participants, the experimental group received 10 group-based schema therapy sessions (90-minute weekly sessions). The control group received no treatment. In the last session of the schema therapy program, a post-test was performed in the experimental and control groups. The follow-up phase was performed after 45 days. In the present study, the mean scores of the research variables per couple were calculated. Then, the mean score was obtained from the relevant values. For ethical considerations, the researchers received written informed consent forms from the study participants. The study was approved by the Ethics Committee of Islamic Azad University, Ahvaz Branch (Code: IR.IAU.AHVAZ.REC.1399.019).
The schema therapy sessions were performed once a week based on the schema therapy package of Young and associates [38]. A summary of the provided schema therapy sessions is presented in Table 1.
The obtained data were analyzed by descriptive (mean, standard deviation) and inferential statistics, including repeated-measures Analysis of Variance (ANOVA). The Bonferroni posthoc test was employed to investigate differences in the mean scores of anxiety, cognitive avoidance, and resilience between the pre-test, post-test, and follow-up steps. SPSS was used for analyzing the collected data. The significance level was set at P<0.05.
3. Results
The study participants included 60 subjects (30 couples) visiting Ahvaz counseling centers, aged 25-45 years. The demographic characteristics of the explored couples are listed in Table 2.
Table 3 presents the group-wise pre-test, post-test, and follow-up Mean±SD scores of anxiety, cognitive avoidance, and resilience among the examined couples.
The baseline values of anxiety, cognitive avoidance, and resilience were considered as covariates. The calculated correlation coefficients ranged between 0.09 (P>0.05) and 0.10 (P>0.05). According to the obtained correlations, the multicollinearity assumption was established between auxiliary variables (covariates). In this study, Levene’s test of equality of variances was used to examine the homogeneity of variances. The F-value calculated in Levene’s test was not significant respecting anxiety, cognitive avoidance, and resilience in the pre-test, post-test, and follow-up phases; therefore, there was no significant difference in error variances between the experimental and control groups.
Based on the results of within groups analysis, there was a significant difference in the mean scores of anxiety, cognitive avoidance, and resilience between the pre-test, post-test, and follow-up phases in the intervention group (P<0.001). Furthermore, 32% of the differences in anxiety, 46% in cognitive avoidance, and 40% in resilience were due to the interaction of the effect of the pre-test, post-test, and follow-up steps. Based on the results of the between-groups analysis, the mean scores of anxiety, cognitive avoidance, and resilience significantly differed in the experimental group (schema therapy) and the control group (P<0.001). Additionally, 57% of the differences in anxiety, 56% in cognitive avoidance, and 26% in resilience were due to group × time interaction effects (Table 4).
The results of the Bonferroni posthoc test for comparing the research groups are presented in Table 5.
According to the relevant results, there was a significant difference between the pre-test and post-test scores in anxiety, cognitive avoidance, and resilience (P<0.001). There was also a significant difference between pre-test and follow-up values in research variables (P<0.001). In other words, the stability of the intervention was confirmed for all variables. Moreover, comparing post-test and follow-up scores of the study variables revealed no significant difference (P>0.05).
4. Discussion
The present study investigated the effects of schema therapy on anxiety, cognitive avoidance, and resilience in couples visiting Ahvaz counseling centers in 2020. The obtained results indicated that schema therapy effectively decreased anxiety and cognitive avoidance and increased resilience in the experimental group. This finding was consistent with those of Dattilio [28] and Mohammadi et al. [29]. By taking advantage of experimental techniques, which reconstruct childhood cognition and memories, schema therapy can greatly help the expression of suppressed emotions; finally, it may result in emotional self-censorship, difficulty in the expression of emotions, and emotional coldness. Schema therapy establishes a good relationship between the past and the present. According to Young et al. [38], schema therapy can effectively treat psychological problems. This is because it combines cognitive, behavioral, interpersonal, and experimental techniques for evaluating schemas; thus, schema therapy can improve anxiety by emphasizing the roots of problems and transformational processes involved in creating and maintaining schemas. Anxiety can reduce couples’ self-esteem; consequently, it might impair a family’s mental health status. Anxiety is a generalized, unpleasant, and often vague feeling of concern that signals a sudden and imminent danger, preparing individuals to face the threat [23]. Modifying and adjusting them through psychological training, like schema therapy, can play an effective role in the destructive actions of individuals. This is because emotions act as solutions to cope with challenges, stress, and problems of life. In other words, emotions play an essential role in life. Accordingly, teaching these techniques to individuals with marital conflicts, to regulate emotions as a healing method for modifying emotions, is associated with acceptance and positive social interaction. Eventually, this process results in effective coping with the challenging and stressful situations of marital life and increases participation in responding to social situations [25]. Therefore, by informing individuals of their positive and negative emotions to accept and express them promptly, schema therapy can significantly reduce destructive behaviors and increase positive behaviors.
Cognitive avoidance is a manner that couples choose for facing social events and interpersonal relationships to respond to stressful situations. Based on this strategy, individuals change their minds during social relations. Various strategies are employed in cognitive avoidance, including intentional attempts to suppress thought, thought substitution, the avoidance of frightening stimuli, distraction, and turning imagination into thought [26]. These strategies are used to divert the mind from worrying topics to other ones. Schema therapy facilitates change through working on the individual’s multifaceted dimensions, including cognitive, experimental, emotional, and behavioral aspects. In the cognitive dimension, schema therapy focuses on the internalized voice of parents and the deepest emotional level, i.e., schemas; thus, it helps couples who are unhappy with their marital life find the roots of their emotions to question the schema and its resulting emotions. It also helps them to foster a new perspective on marital relationships by examining the schema’s correctness and finding a new definition for the schema approving or disproving evidence. Individuals emphasize information, i.e., consistent with the schema, and ignore the inconsistent data. They continue this process in their marital relationships and can observe the direct effect of the schema on marital relationships [27]. Schema therapy, as a summary of the individual’s healthy responses and the identification of the schema roots and inefficient thoughts, is the most beneficial tool for an individual to identify the schema motivating situations, to diagnose negative behaviors, and to replace healthy behaviors in marital relationships; accordingly, this method informs the individual about schemas and facilitates change in them, and consequently in the couple’s relationship.
Spouses require a high level of resilience in their marital life. This is because of the perception of their psychological challenges, conflicts, and stressful living conditions. They have an analytical-critical mentality about their abilities and circumstances; they reflect on abilities and circumstances. They are resilient in different situations and have a wonderful imagination (thinking power) about the solutions. Resilience refers to return to the original balance or reaching a higher level of balance. Therefore, it provides a successful adaptation in life. Positive adaptation with life not only can be a consequence of resilience but also can lead to a higher level of resilience. Schema-based approaches are useful in modifying the beliefs and thoughts of individuals with a desire for divorce; they can reduce the desire for divorce, as they work on psychological themes or early maladaptive schemas [39]. In the emotional dimension, schema therapy uses experimental strategies to challenge the cognitive belief, i.e., tied to emotional belief to make the couples fight their schemas in the treatment session at the cognitive and emotional levels [24]. This technique helps the couples to express their emotions in marital relationships; accordingly, they can recognize their unknown emotional needs that have led to the formation of maladaptive schemas. An interesting technique of experimental strategy, namely writing a letter to the spouse, helps the individual to use it as an opportunity to realize the rights, feelings, unexpressed anger, and the expression of beliefs that seem to cause a problem in the couple’s communication pattern.
A limitation of the present study was that this approach was applied to both married men and women and the researcher was unable to establish separate gender-wise groups. It is suggested that researchers examine the effectiveness of this approach on other aspects of marital life.
5. Conclusion
Schema therapy decreased anxiety, cognitive avoidance, and increased resilience in the explored couples with marital conflicts. Schema therapy can be used to improve resilience in couples involved in marital conflicts. Given the results obtained in this study, therapists and counselors are recommended to use schema therapy to improve marital variables.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the Islamic Azad University, Ahvaz Branch (Code: IR.IAU.AHVAZ.REC.1399.019).
Funding
This article was extracted from the PhD. dissertation of the first author at the Department of Psychology, Ahvaz Branch, Islamic Azad University, Ahvaz.
Authors' contributions
Conceptualization and supervision: Shabnam Mohammadian, Parviz Asgari; Methodology: Shabnam Mohammadian, Behnam Makvandi; Investigation, writing–review & editing: Parviz Asgari, Farah Naderi; Writing – original draft and funding acquisition, resources: Shabnam Mohammadian, Parviz Asgari.
Conflict of interest
The authors declared no conflicts of interest.
References
- Thomas PA, Liu H, Umberson D. Family relationships and well-being. Innov Aging. 2017; 1(3):igx025. [DOI:10.1093/geroni/igx025] [PMID] [PMCID]
- Noruzi S, Maarefvand M, Khanke HR, Eghlima M. A qualitative research on couples’ sexual satisfaction with emphasis on individual socio-cultural factors. Caspian J Health Res. 2019; 4(4):105-9. [DOI:10.29252/cjhr.4.4.105]
- Guerrero-Barona E, Guerrero-Molina M, García-Gómez A, Moreno-Manso JM, García-Baamonde ME. Quality of working life, psychosocial factors, burnout syndrome and emotional intelligence. Int J Environ Res Public Health. 2020; 17(24):9550. [DOI:10.3390/ijerph17249550] [PMID] [PMCID]
- Robles TF, Slatcher RB, Trombello JM, McGinn MM. Marital quality and health: A meta-analytic review. Psychol Bull. 2014; 140(1):140-87. [DOI:10.1037/a0031859] [PMID] [PMCID]
- Shahraki Z, Ghajarzadeh M, Ganjali M. Depression, anxiety, quality of life and sexual dysfunction in Zabol women with infertility. Maedica. 2019; 14(2):131-4. [PMID] [PMCID]
- Yusuf L. Depression, anxiety and stress among female patients of infertility; A case control study. Pak J Med Sci. 2016; 32(6):1340-3. [DOI:10.12669/pjms.326.10828] [PMID] [PMCID]
- Jahanbin-Amirhandeh E, Hakim-Javadi M, Hosein-Khanzadeh AA, Hatamian HR. Comparison of anxiety, depression and lifestyle in obese and normal weight children. Caspian J Health Res. 2018; 3(2):35-40. [DOI:10.29252/cjhr.3.2.35]
- MacNamara A, Kotov R, Hajcak G. Diagnostic and symptom-based predictors of emotional processing in generalized anxiety disorder and major depressive disorder: An event-related potential study. Cognit Ther Res. 2016; 40(3):275-89. [DOI:10.1007/s10608-015-9717-1] [PMID] [PMCID]
- Cisler JM, Olatunji BO, Feldner MT, Forsyth JP. Emotion regulation and the anxiety disorders: An integrative review. J Psychopathol Behav Assess. 2010; 32(1):68-82. [DOI:10.1007/s10862-009-9161-1] [PMID] [PMCID]
- Cisler JM, Olatunji BO. Emotion regulation and anxiety disorders. Curr Psychiatry Rep. 2012; 14(3):182-7. [DOI:10.1007/s11920-012-0262-2] [PMID] [PMCID]
- Sbarra DA, Hasselmo K, Bourassa KJ. Divorce and health: Beyond individual differences. Curr Dir Psychol Sci. 2015; 24(2):109-13. [DOI:10.1177/0963721414559125] [PMID] [PMCID]
- McCoy KP, George MRW, Cummings EM, Davies PT. Constructive and destructive marital conflict, parenting, and children’s school and social adjustment. Soc Dev. 2013; 22(4):641-62. [DOI:10.1111/sode.12015] [PMID] [PMCID]
- Hofmann SG. Cognitive factors that maintain social anxiety disorder: A comprehensive model and its treatment implications. Cogn Behav Ther. 2007; 36(4):193-209. [DOI:10.1080/16506070701421313] [PMID] [PMCID]
- Martin RC, Dahlen ER. Cognitive emotion regulation in the prediction of depression, anxiety, stress, and anger. Pers Individ Dif. 2005; 39(7):1249-60. [DOI:10.1016/j.paid.2005.06.004]
- Holaway RM, Heimberg RG, Coles ME. A comparison of intolerance of uncertainty in analogue obsessive-compulsive disorder and generalized anxiety disorder. J Anxiety Disord. 2006; 20(2):158-74. [DOI:10.1016/j.janxdis.2005.01.002] [PMID]
- Lillis J, Wing RR. The role of avoidance-based coping in the psychosocial functioning of weight loss treatment-seeking adults. Obes Sci Pract. 2015; 1(1):59-64. [DOI:10.1002/osp4.1] [PMID] [PMCID]
- Stapinski LA, Abbott MJ, Rapee RM. Evaluating the cognitive avoidance model of generalised anxiety disorder: Impact of worry on threat appraisal, perceived control and anxious arousal. Behav Res Ther. 2010; 48(10):1032-40. [DOI:10.1016/j.brat.2010.07.005] [PMID]
- Bradley JM, Hojjat M. A model of resilience and marital satisfaction. J Soc Psychol. 2017; 157(5):588-601. [DOI:10.1080/00224545.2016.1254592] [PMID]
- Clark P. Resiliency in the practicing marriage and family therapist. J Marital Fam Ther. 2009; 35(2):231-47. [DOI:10.1111/j.1752-0606.2009.00108.x] [PMID]
- Masarik AS, Martin MJ, Ferrer E, Lorenz FO, Conger KJ, Conger RD. Couple resilience to economic pressure over time and across generations. J Marriage Fam. 2016; 78(2):326-45. [DOI:10.1111/jomf.12284] [PMID] [PMCID]
- Wade JB, Hart RP, Wade JH, Bajaj JS, Price DD. The relationship between marital status and psychological resilience in chronic pain. Pain Res Treat. 2013; 2013:928473. [DOI:10.1155/2013/928473] [PMID] [PMCID]
- Ha JY, Ban SH. Effect of resilience on infertile couples’ quality of life: An actor-partner interdependence model approach. Health Qual Life Outcomes. 2020; 18(1):295. [DOI:10.1186/s12955-020-01550-6] [PMID] [PMCID]
- Taylor CDJ, Bee P, Haddock G. Does schema therapy change schemas and symptoms? A systematic review across mental health disorders. Psychol Psychother. 2017; 90(3):456-79. [DOI:10.1111/papt.12112] [PMID] [PMCID]
- Kopf-Beck J, Zimmermann P, Egli S, Rein M, Kappelmann N, Fietz J, et al. Schema therapy versus cognitive behavioral therapy versus individual supportive therapy for depression in an inpatient and day clinic setting: Study protocol of the OPTIMA-RCT. BMC Psychiatry. 2020; 20(1):506. [DOI:10.1186/s12888-020-02880-x] [PMID] [PMCID]
- Baljé A, Greeven A, van Giezen A, Korrelboom K, Arntz A, Spinhoven Ph. Group schema therapy versus group cognitive behavioral therapy for social anxiety disorder with comorbid avoidant personality disorder: Study protocol for a randomized controlled trial. Trials. 2016; 17(1):487. [DOI:10.1186/s13063-016-1605-9] [PMID] [PMCID]
- Mohammadi S, Hafezi F, Ehteshamzadeh P, Eftekhar Saadi Z, Bakhtiarpour S. Effectiveness of schema therapy and emotional self-regulation therapy in the components of women’s marital conflicts. J Client Cent Nurs Care. 2020; 6(4):277-88. [DOI:10.32598/JCCNC.6.4.341.1]
- Erfan A, Noorbala AA, Karbasi Amel S, Mohammadi A, Adibi P. The effectiveness of emotional schema therapy on the emotional schemas and emotional regulation in irritable bowel syndrome: Single subject design. Adv Biomed Res. 2018; 7:72. [DOI:10.4103/abr.abr_113_16] [PMID] [PMCID]
- Dattilio FM. The restructuring of family schemas: A cognitive-behavior perspective. J Marital Fam Ther. 2005; 31(1):15-30. [DOI:10.1111/j.1752-0606.2005.tb01540.x] [PMID]
- Mohammadi S, Hafezi F, Ehteshamzadeh P, Eftekhar Saadi Z, Bakhtiarpour S. The effect of schema therapy on sexual self-esteem in the women involved in marital conflicts. Womens Health Bull. 2020; 7(2):49-55. [DOI:10.30476/WHB.2020.86498.1058]
- Connor KM, Davidson JR. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003; 18(2):76-82. [DOI:10.1002/da.10113] [PMID]
- Keyhani M, Taghvaei D, Rajabi A, Amirpour B. [Internal consistency and confirmatory factor analysis of the Connor-Davidson Resilience Scale (CD-RISC) among nursing female (Persian)]. Iran J Med Educ. 2015; 14(10):857-65. http://ijme.mui.ac.ir/article-1-3254-fa.html
- Badie A, Makvandi B, Bakhtiarpour S, Pasha R. Drug cravings and its relationship with family communication patterns and resiliency through the mediatory role of difficulty in cognitive emotion regulation. J Client Cent Nurs Care. 2020; 6(2):125-34. [DOI:10.32598/JCCNC.6.2.329.1]
- Sexton KA, Dugas MJ. The Cognitive Avoidance Questionnaire: Validation of the English translation. J Anxiety Disord. 2008; 22(3):355-70. [DOI:10.1016/j.janxdis.2007.04.005] [PMID]
- Besharat MA, Mirjalili RS. [The simple and multiple relations of cognitive characteristics and worry in patients with generalized anxiety and obsessive-compulsive disorders (Persian)]. J Dev Psychol. 2014; 11(41):3-17. http://jip.azad.ac.ir/article_512176.html
- Aghajani S, Samadifard HR, Narimani M. [The role of cognitive avoidance components and metacognitive belief in the prediction of quality of life in diabetic patients (Persian)]. Q J Health Psychol. 2017; 6(21):142-56. http://hpj.journals.pnu.ac.ir/article_3705.html
- Tomioka M, Shimura M, Hidaka M, Kubo Ch. The reliability and validity of a Japanese version of symptom checklist 90 revised. Biopsychosoc Med. 2008; 2:19. [DOI:10.1186/1751-0759-2-19] [PMID] [PMCID]
- Akhavan Abiri F, Shairi M. [Validity and reliability of Symptom Checklist-90-Revised (SCL-90-R) and Brief Symptom Inventory-53 (BSI-53) (Persian)]. Clin Psychol Personal. 2019; 17(2):169-95. [DOI:10.22070/CPAP.2020.2916]
- Young JE, Klosko JS, Weishaar ME. Schema therapy: A practitioner’s guide. New York, NY: Guilford Press. 2006. https://www.guilford.com/books/Schema-Therapy/Young-Klosko-Weishaar/9781593853723
- Heilemann MV, Pieters HC, Kehoe P, Yang Q. Schema therapy, motivational interviewing, and collaborative-mapping as treatment for depression among low income, second generation Latinas. J Behav Ther Exp Psychiatry. 2011; 42(4):473-80. [DOI:10.1016/j.jbtep.2011.05.001] [PMID] [PMCID]
Article Type: Original Contributions |
Subject:
Health Education and Promotion
Received: 2021/04/27 | Accepted: 2021/06/1 | Published: 2021/06/8
Received: 2021/04/27 | Accepted: 2021/06/1 | Published: 2021/06/8
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Contact Information
cjhr Office, Guilan University of Medical Sciences
P.O.Box 93345-41938, Rasht, Iran
Journal Tel: +9813 33335820
Publisher Tel: +9821 453 55 000
Email: cjhr.gums@gmail.com
