

Volume 6, Issue 3 (9-2021)
CJHR 2021, 6(3): 101-108 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mobayen M, Zarei R, Masoumi S, Shahrousvand M, Mazloum S M H, Ghaed Z et al . Epidemiology of Childhood Burn: A 5-Year Retrospective Study in the Referral Burn Center of Northern Iran. CJHR 2021; 6 (3) :101-108
URL: http://cjhr.gums.ac.ir/article-1-204-en.html
URL: http://cjhr.gums.ac.ir/article-1-204-en.html
Mohammadreza Mobayen1 

 , Reza Zarei2 , Sanaz Masoumi1 , Mohsen Shahrousvand3 , Seyyed Mohammad Hossein Mazloum1 , Zeinab Ghaed4 , Negin Rahimzadeh * 5
, Reza Zarei2 , Sanaz Masoumi1 , Mohsen Shahrousvand3 , Seyyed Mohammad Hossein Mazloum1 , Zeinab Ghaed4 , Negin Rahimzadeh * 5
, Reza Zarei2 , Sanaz Masoumi1 , Mohsen Shahrousvand3 , Seyyed Mohammad Hossein Mazloum1 , Zeinab Ghaed4 , Negin Rahimzadeh * 5
1- Burns and Regenerative Medicine Research Center, Guilan University of Medical Sciences, Rasht, Iran.
2- Department of Statistics, Faculty of Mathematical Sciences, University of Guilan, Rasht, Iran.
3- Department of Polymer Engineering and Color Technology, School of Engineering, Amirkabir University of Technology, Tehran, Iran.
4- Health Services Management, Guilan University of Medical Science, Rasht, Iran.
5- Burns and Regenerative Medicine Research Center, Guilan University of Medical Sciences, Rasht, Iran. , n.rahimzadeh97@gmail.com
2- Department of Statistics, Faculty of Mathematical Sciences, University of Guilan, Rasht, Iran.
3- Department of Polymer Engineering and Color Technology, School of Engineering, Amirkabir University of Technology, Tehran, Iran.
4- Health Services Management, Guilan University of Medical Science, Rasht, Iran.
5- Burns and Regenerative Medicine Research Center, Guilan University of Medical Sciences, Rasht, Iran. , n.rahimzadeh97@gmail.com
Full-Text [PDF 1472 kb]
(387 Downloads)
| Abstract (HTML) (1091 Views)
Full-Text: (547 Views)
1. Introduction
Despite all the advances, there are still significant injuries threatening human life. One of these injuries is burn, which takes many people’s lives and causes many disabilities every year, even in developed countries [1]. Burn injury is one of the important reasons for morbidity and mortality in developing countries that can affect the psychological and functional behaviors of patients [2].
Burns account for an estimated 180000 deaths annually. Nowadays, the rate of child deaths from burns is over seven times higher in low- and middle-income countries than in high-income countries [3]. Burn can affect anybody, regardless of age or socioeconomic status [4]. Moreover, it is globally the most common type of pediatric injury and is the leading cause of household injuries [5]. Besides its health care and socioeconomic costs, the burn can cause irreparable psychological damages to children and their families.
Children under 5 years are the most susceptible group to burns considering their innate curiosity and high motility. A recent study showed that the pathophysiology and etiology of burns in children younger than 5 years are different from children older than 5 years [5].
Understanding the burns epidemiology is essential for planning, implementing, and evaluating the prevention programs [6]. Scalds and contact burns were the most common reported burn injuries in children [7], especially children less than 16 years of age [8]. A 2016 Chinese study estimated the incidence of burns in rural children at 12.7%. It also claimed that increasing the child’s knowledge about burn prevention and first-aid treatments can decrease the incidence of pediatric burns [9]. Also, a 2008 study in Guilan Province showed that the most burned cases were among children under 2 years old; the most scalds occurred during cooking and eating hours. Moreover, increasing in burn severity and Burned Body Surface Area (BBSA) were related to the outcomes [10].
Considering the differences in epidemiological burn indicators and their related outcomes in different populations, we investigated the epidemiology of childhood burn in children under 16 in northern Iran and its relationship between different factors.
2. Materials and Methods
Study setting and study population
This study was a retrospective cross-sectional analytical study that aimed to investigate the epidemiology of childhood burn in children under 16 years old. The study population included burnt patients aged under 16 years who had been referred to Velayat Educational Burn Center, Rasht City, Guilan, Iran, 2013-2018. The inclusion criteria included: 1) children aged under 16 years old; 2) absence of any other chronic and comorbid diseases; 3) satisfaction of children and their parents.
Study variables
The study variables were collected from electronic hospital records of patients. Individual social variables were included age, sex, place of residence, work status of their parents, and presence or absence of the mother or babysitter during the event. The clinical and therapeutic variables were included place, date, and time of injury, burn etiology, BBSA, burn severity, and the anatomical area. In this study, the prognostic outcome was defined as hospitalization. BBSA was measured according to the rule of nine [11].
Statistical analysis
Continuous data were described as mean ± standard deviation, and categorical variables were reported as frequency and percentages. The Chi-squared test and Fisher exact test were used to compare categorical variables. Continuous variables were compared using the Mann-Whitney U test. All statistical analyses were two-tailed, and a P<0.05 was considered statistically significant. All analyses were performed with the statistical package using SPSS v. 24.
3. Results
The demographic data of this study are shown in Figure 1.
.png)
Based on the results, 52.9% of patients were urban (23.4% girls and 29.4% boys), and 47.1% were rural (21.1% girls and 26.1% boys). The Mean±SD age of the patients was 4.54±3.87, with an age range of 1 month to 16 years. The Mean±SD age of the girls and boys were 4.22±3.64 and 4.80±4.03 years, respectively. The highest frequency of burns (56.1%) was reported in the 1-5 years age group.
The lower extremities (255 patients, 35.6%) were the most affected area. The Mean±SD BBSA percentage was 11.67±11.61%, and the Mean±SD duration of hospitalization was 3.07±4.15 days.
Based on the recorded information about the mother’s employment status, 60 mothers were manual workers (8.4%), 218 were employees (30.4%), 187 were self-employed, 185 were homemakers (25.8%), 41 were farmers (5.7%), and 26 mothers had other employment statuses. Additionally, 257 fathers were manual workers (35.8%), 192 were employees (26.8%), 127 were self-employed (17.7%), 108 were farmers (15.1%), 27 were unemployed (3.8%), and 6 had other jobs (0.8%).
Examination of the person supervising the child during the burn showed that 324 children (45.2%) were observed by their mothers, 41 children by their fathers (5.7%), 34 children with their both parents (4.7%), 192 children with their grandmothers (26.8%), 119 children with babysitters (16.6%) and 7 patients with their aunts (1%). Based on the results, there was no significant relationship between BBSA and the supervisor of the child (P=0.863).
The highest burn frequency was related to winter (215 cases, 29.9%), with the highest frequency of burns in March (79 patients, 36.7% of winter cases, and 11% of the total cases). On the other hand, the lowest proportion of burn injuries was related to summer (147 cases, 20.5%), with the highest frequency in July (53 patients, 36% of the summer, and 7% of the total). Table 1 presents the number of burns according to the season and month of the year.
.png)
Daily investigation showed that the highest frequency was related to Saturdays (22.7%), followed by Mondays (15.9%) and Thursdays (13.4%). The other days of the weeks were between 11.3% to 12.3%.
For hourly investigation, the day was divided into four 6-hour sections. The highest frequency of burns was between 6 and 12 o’clock (42.8%). Likewise, the burn frequencies of 12-18 o’clock, 18-24 o’clock, and 24-6 o’clock was 38.1%, 16.9%, and 2.2%, respectively. Additionally, there was no significant relationship between age groups and incidence per hour (P=0.399).
Table 2 presents the association of burn-related characteristics with hospitalization duration.
.png)
To explore the predictors of hospitalization, we divided them into two categories of less than ten days (682 patients, 95.1%) and more than ten days (35 patients, 4.9%).
There were significant relationships between duration of hospitalization and etiology (P=0.003), burn severity (P=0.002), and BBSA (P=0.001). The most common type of burns in both periods of less and more than ten days of hospitalization was related to scalds. Patients with more than 10 days of hospitalization were more likely to suffer from fire (25.7%) followed by electrical burns (7.7%) compared to patients with less than 10 days of hospitalization (13.4% and 1.3%, respectively).
As expected, the frequency of more severe degrees of burn (the second- and third-degree) in patients with more than 10 days of hospitalization (57.1%) was higher than patients with less than 10 days of hospitalization (32.1%). Additionally, patients hospitalized for less than 10 days were more likely to had <10% BBSA (66.4%), while those who hospitalized for more than 10 days were more suffered from 30%-40% BBSA (25.7%).
The mean BBSA percentage was significantly associated with the cause of burn (F=7.34, P=0.001). The mean BBSA percentage in fire (16.17±16.98) was significantly higher than other causes of burn.
Figure 2 shows the association of burn severity and cause of the burn.
.png)
There was significant association between burn etiology and burn degree (P=0.002). Fire and electrical burns predominantly caused mixed second- and third-degree burns, while scald and chemical burns predominantly caused the second-degree burn. chemical and contact burn had the highest frequency of first degree burn (12%) compared to other cause of burn.
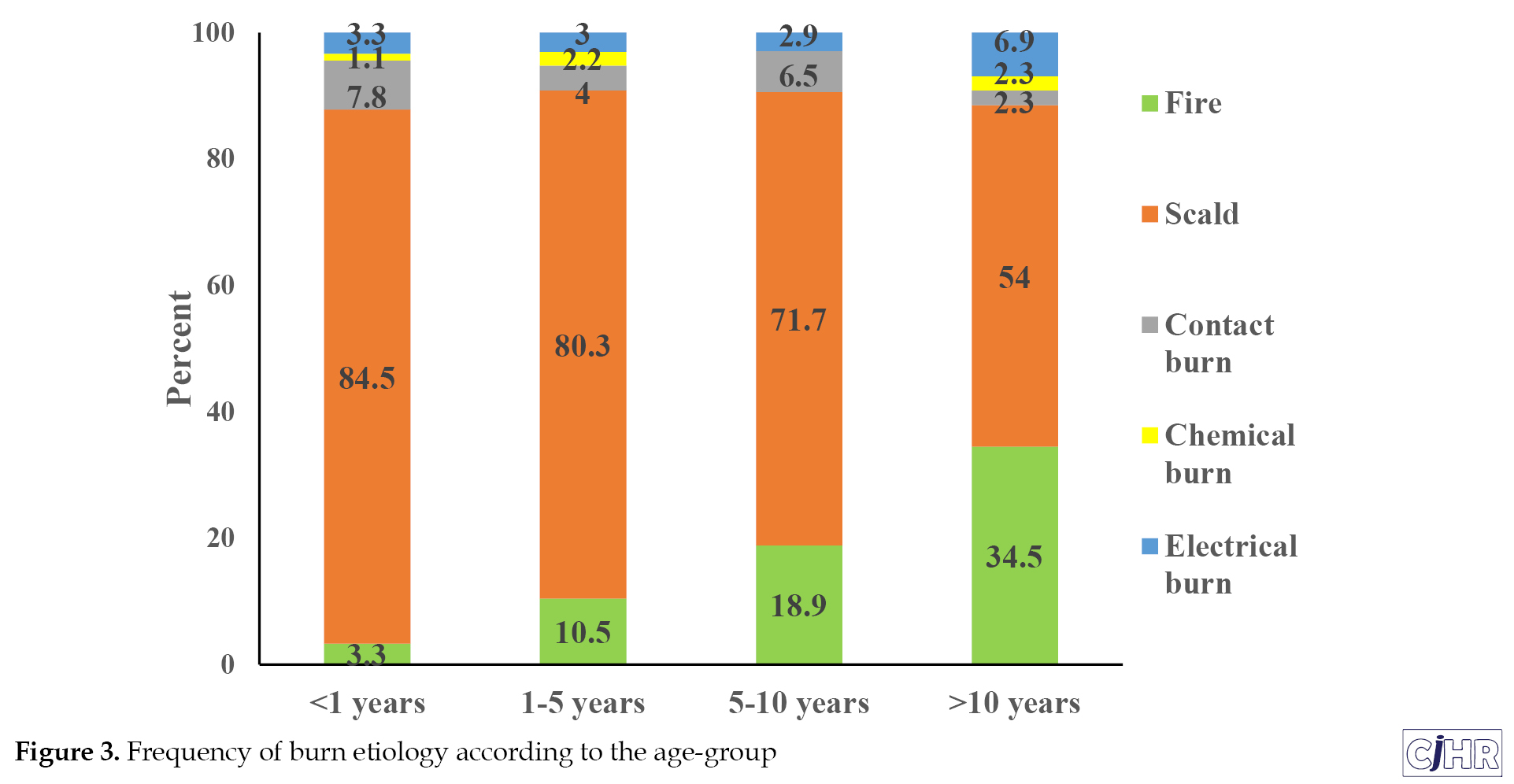
Moreover, there was a significant relationship between age groups and burn etiology (P=0.001). Children older than 10 years were more likely to burn from fire (34.5%) than other age groups. Similarly, the percentage of electrical burn in children older than 10 years (6.9%) was higher than in other age groups. Scald was reported as the most common type of burns etiology in all age groups (Figure 3).
4. Discussion
The epidemiology of burns is vital for better understanding and management of patients, taking measures for successful prevention and treatment, and evaluating the quality of burn cares in each region. This study showed that the sex ratio in children with burns was 1.2, and children in 1-5 years old constituted up to 68.7% of the patients. These findings were in accordance with previous studies [5, 10, 12]. In agreement with previous studies [12, 13, 14], the overall incidence was slightly higher in boys than girls, likely because the families considered less limitation for boys [15].
This study revealed that the leading cause of pediatric burns was scalds due to hot liquids or scalds, which was compatible with previous studies [9, 16, 17]. The lower extremities were the most injured body parts, which somehow conflicted with past studies [8, 9, 10]. Battle et al. reported that the most commonly injured site in both age groups was a hand or digit [8].
The mean BBSA percentage was 11.7%, which is lower than the similar Australian population with more than 20% [18]. Second-degree burns were the most common burn severity pattern in this study (47.1%). It was compatible with Almarghoub et al. result, except with a slightly lower percentage (57.7%) [19]. The hospital stay was directly related to BBSA. In another Iranian study, the length of stay was 10 days [12], while the mean length of hospitalization in this study was three days.
The highest proportion of burn was related to winter (30%), compatible with other studies [20, 21, 22]. A probable explanation of higher incidence proportion during March and April could be the holding of traditional festivals, like the Scarlet Wednesday, during this month. In this study, the lowest proportion was in summer (20%), contrasting previous studies [12, 22]. Karimi et al. found that summer is the season with the highest proportion (32.4%) of burn injury [12].
Most burns in the present study occurred between 6 and 12 o’clock, covering most working hours. Considering the distribution of most cases on working days, a logical explanation for this result could be the occupation of the parents and the reduction of necessary care of the child at the time of the accident. Further studies are needed to investigate this matter more closely.
In this study, most patients hospitalized for less than 10 days were similar to a study by Alipour et al. (mean hospital stay=7 days) [21] and Karimi et al., which have claimed that the mean hospitalization period for scalds was less than 10 days [12].
According to the results, patients with >10 days of hospitalization were more likely to burn with fire than those with <10 days. This finding confirms the results of another study which showed that most patients with >14 days of hospital stay were affected by fire and injury [23].
This study reconfirms the necessity of preventive programs for burns among children, especially for health providers in Iran. Policymakers should be aware of the annual increase in the number of children hospitalized for burn injury. Increasing efficient household safety measures, training families and parents on risk prevention, and designing educational programs and regulations are some possible recommendations. Further studies to evaluate the efficacy of these recommendations should be carried out.
5. Conclusion
This study showed that children of 1-5 years old were the most susceptible age groups for burn injuries and scalds were the most common cause of the burn. The male to female ratio was 1.2, and the majority of burns occurred in the winter. This study prompts the necessity of preventive programs for burns among children. Increased public awareness and education are necessary to decrease the incidence of these potentially catastrophic injuries, especially in preschool-age groups and male patients who are more susceptible to burn.
Ethical Considerations
Compliance with ethical guidelines
The protocol of this study was approved by the Institutional Review Board of Guilan University of Medical Sciences (IR.GUMS.REC.1397.165).
Funding
This paper was extracted from the research project (No. 2708), funded by the Guilan University of Medical Sciences, Rasht, Iran.
Authors' contributions
Conceptualization and Supervision : Mohammad Reza Mobayen; Methodology: Reza Zarei; Investigation, writing - original draft and writing – review and editing : all authors; Data collection: Sanaz Masoumi, Zeinab Ghaedchukamei, Seyyed Mohammad Hossein Mazloum and Negin Rahimzadeh; Funding acquisition and resources: Mohsen Shahrousvand.
Conflict of interest
The authors declared no competing interests.
Refrences
Despite all the advances, there are still significant injuries threatening human life. One of these injuries is burn, which takes many people’s lives and causes many disabilities every year, even in developed countries [1]. Burn injury is one of the important reasons for morbidity and mortality in developing countries that can affect the psychological and functional behaviors of patients [2].
Burns account for an estimated 180000 deaths annually. Nowadays, the rate of child deaths from burns is over seven times higher in low- and middle-income countries than in high-income countries [3]. Burn can affect anybody, regardless of age or socioeconomic status [4]. Moreover, it is globally the most common type of pediatric injury and is the leading cause of household injuries [5]. Besides its health care and socioeconomic costs, the burn can cause irreparable psychological damages to children and their families.
Children under 5 years are the most susceptible group to burns considering their innate curiosity and high motility. A recent study showed that the pathophysiology and etiology of burns in children younger than 5 years are different from children older than 5 years [5].
Understanding the burns epidemiology is essential for planning, implementing, and evaluating the prevention programs [6]. Scalds and contact burns were the most common reported burn injuries in children [7], especially children less than 16 years of age [8]. A 2016 Chinese study estimated the incidence of burns in rural children at 12.7%. It also claimed that increasing the child’s knowledge about burn prevention and first-aid treatments can decrease the incidence of pediatric burns [9]. Also, a 2008 study in Guilan Province showed that the most burned cases were among children under 2 years old; the most scalds occurred during cooking and eating hours. Moreover, increasing in burn severity and Burned Body Surface Area (BBSA) were related to the outcomes [10].
Considering the differences in epidemiological burn indicators and their related outcomes in different populations, we investigated the epidemiology of childhood burn in children under 16 in northern Iran and its relationship between different factors.
2. Materials and Methods
Study setting and study population
This study was a retrospective cross-sectional analytical study that aimed to investigate the epidemiology of childhood burn in children under 16 years old. The study population included burnt patients aged under 16 years who had been referred to Velayat Educational Burn Center, Rasht City, Guilan, Iran, 2013-2018. The inclusion criteria included: 1) children aged under 16 years old; 2) absence of any other chronic and comorbid diseases; 3) satisfaction of children and their parents.
Study variables
The study variables were collected from electronic hospital records of patients. Individual social variables were included age, sex, place of residence, work status of their parents, and presence or absence of the mother or babysitter during the event. The clinical and therapeutic variables were included place, date, and time of injury, burn etiology, BBSA, burn severity, and the anatomical area. In this study, the prognostic outcome was defined as hospitalization. BBSA was measured according to the rule of nine [11].
Statistical analysis
Continuous data were described as mean ± standard deviation, and categorical variables were reported as frequency and percentages. The Chi-squared test and Fisher exact test were used to compare categorical variables. Continuous variables were compared using the Mann-Whitney U test. All statistical analyses were two-tailed, and a P<0.05 was considered statistically significant. All analyses were performed with the statistical package using SPSS v. 24.
3. Results
The demographic data of this study are shown in Figure 1.
Based on the results, 52.9% of patients were urban (23.4% girls and 29.4% boys), and 47.1% were rural (21.1% girls and 26.1% boys). The Mean±SD age of the patients was 4.54±3.87, with an age range of 1 month to 16 years. The Mean±SD age of the girls and boys were 4.22±3.64 and 4.80±4.03 years, respectively. The highest frequency of burns (56.1%) was reported in the 1-5 years age group.
The lower extremities (255 patients, 35.6%) were the most affected area. The Mean±SD BBSA percentage was 11.67±11.61%, and the Mean±SD duration of hospitalization was 3.07±4.15 days.
Based on the recorded information about the mother’s employment status, 60 mothers were manual workers (8.4%), 218 were employees (30.4%), 187 were self-employed, 185 were homemakers (25.8%), 41 were farmers (5.7%), and 26 mothers had other employment statuses. Additionally, 257 fathers were manual workers (35.8%), 192 were employees (26.8%), 127 were self-employed (17.7%), 108 were farmers (15.1%), 27 were unemployed (3.8%), and 6 had other jobs (0.8%).
Examination of the person supervising the child during the burn showed that 324 children (45.2%) were observed by their mothers, 41 children by their fathers (5.7%), 34 children with their both parents (4.7%), 192 children with their grandmothers (26.8%), 119 children with babysitters (16.6%) and 7 patients with their aunts (1%). Based on the results, there was no significant relationship between BBSA and the supervisor of the child (P=0.863).
The highest burn frequency was related to winter (215 cases, 29.9%), with the highest frequency of burns in March (79 patients, 36.7% of winter cases, and 11% of the total cases). On the other hand, the lowest proportion of burn injuries was related to summer (147 cases, 20.5%), with the highest frequency in July (53 patients, 36% of the summer, and 7% of the total). Table 1 presents the number of burns according to the season and month of the year.
Daily investigation showed that the highest frequency was related to Saturdays (22.7%), followed by Mondays (15.9%) and Thursdays (13.4%). The other days of the weeks were between 11.3% to 12.3%.
For hourly investigation, the day was divided into four 6-hour sections. The highest frequency of burns was between 6 and 12 o’clock (42.8%). Likewise, the burn frequencies of 12-18 o’clock, 18-24 o’clock, and 24-6 o’clock was 38.1%, 16.9%, and 2.2%, respectively. Additionally, there was no significant relationship between age groups and incidence per hour (P=0.399).
Table 2 presents the association of burn-related characteristics with hospitalization duration.
To explore the predictors of hospitalization, we divided them into two categories of less than ten days (682 patients, 95.1%) and more than ten days (35 patients, 4.9%).
There were significant relationships between duration of hospitalization and etiology (P=0.003), burn severity (P=0.002), and BBSA (P=0.001). The most common type of burns in both periods of less and more than ten days of hospitalization was related to scalds. Patients with more than 10 days of hospitalization were more likely to suffer from fire (25.7%) followed by electrical burns (7.7%) compared to patients with less than 10 days of hospitalization (13.4% and 1.3%, respectively).
As expected, the frequency of more severe degrees of burn (the second- and third-degree) in patients with more than 10 days of hospitalization (57.1%) was higher than patients with less than 10 days of hospitalization (32.1%). Additionally, patients hospitalized for less than 10 days were more likely to had <10% BBSA (66.4%), while those who hospitalized for more than 10 days were more suffered from 30%-40% BBSA (25.7%).
The mean BBSA percentage was significantly associated with the cause of burn (F=7.34, P=0.001). The mean BBSA percentage in fire (16.17±16.98) was significantly higher than other causes of burn.
Figure 2 shows the association of burn severity and cause of the burn.
There was significant association between burn etiology and burn degree (P=0.002). Fire and electrical burns predominantly caused mixed second- and third-degree burns, while scald and chemical burns predominantly caused the second-degree burn. chemical and contact burn had the highest frequency of first degree burn (12%) compared to other cause of burn.
Moreover, there was a significant relationship between age groups and burn etiology (P=0.001). Children older than 10 years were more likely to burn from fire (34.5%) than other age groups. Similarly, the percentage of electrical burn in children older than 10 years (6.9%) was higher than in other age groups. Scald was reported as the most common type of burns etiology in all age groups (Figure 3).
4. Discussion
The epidemiology of burns is vital for better understanding and management of patients, taking measures for successful prevention and treatment, and evaluating the quality of burn cares in each region. This study showed that the sex ratio in children with burns was 1.2, and children in 1-5 years old constituted up to 68.7% of the patients. These findings were in accordance with previous studies [5, 10, 12]. In agreement with previous studies [12, 13, 14], the overall incidence was slightly higher in boys than girls, likely because the families considered less limitation for boys [15].
This study revealed that the leading cause of pediatric burns was scalds due to hot liquids or scalds, which was compatible with previous studies [9, 16, 17]. The lower extremities were the most injured body parts, which somehow conflicted with past studies [8, 9, 10]. Battle et al. reported that the most commonly injured site in both age groups was a hand or digit [8].
The mean BBSA percentage was 11.7%, which is lower than the similar Australian population with more than 20% [18]. Second-degree burns were the most common burn severity pattern in this study (47.1%). It was compatible with Almarghoub et al. result, except with a slightly lower percentage (57.7%) [19]. The hospital stay was directly related to BBSA. In another Iranian study, the length of stay was 10 days [12], while the mean length of hospitalization in this study was three days.
The highest proportion of burn was related to winter (30%), compatible with other studies [20, 21, 22]. A probable explanation of higher incidence proportion during March and April could be the holding of traditional festivals, like the Scarlet Wednesday, during this month. In this study, the lowest proportion was in summer (20%), contrasting previous studies [12, 22]. Karimi et al. found that summer is the season with the highest proportion (32.4%) of burn injury [12].
Most burns in the present study occurred between 6 and 12 o’clock, covering most working hours. Considering the distribution of most cases on working days, a logical explanation for this result could be the occupation of the parents and the reduction of necessary care of the child at the time of the accident. Further studies are needed to investigate this matter more closely.
In this study, most patients hospitalized for less than 10 days were similar to a study by Alipour et al. (mean hospital stay=7 days) [21] and Karimi et al., which have claimed that the mean hospitalization period for scalds was less than 10 days [12].
According to the results, patients with >10 days of hospitalization were more likely to burn with fire than those with <10 days. This finding confirms the results of another study which showed that most patients with >14 days of hospital stay were affected by fire and injury [23].
This study reconfirms the necessity of preventive programs for burns among children, especially for health providers in Iran. Policymakers should be aware of the annual increase in the number of children hospitalized for burn injury. Increasing efficient household safety measures, training families and parents on risk prevention, and designing educational programs and regulations are some possible recommendations. Further studies to evaluate the efficacy of these recommendations should be carried out.
5. Conclusion
This study showed that children of 1-5 years old were the most susceptible age groups for burn injuries and scalds were the most common cause of the burn. The male to female ratio was 1.2, and the majority of burns occurred in the winter. This study prompts the necessity of preventive programs for burns among children. Increased public awareness and education are necessary to decrease the incidence of these potentially catastrophic injuries, especially in preschool-age groups and male patients who are more susceptible to burn.
Ethical Considerations
Compliance with ethical guidelines
The protocol of this study was approved by the Institutional Review Board of Guilan University of Medical Sciences (IR.GUMS.REC.1397.165).
Funding
This paper was extracted from the research project (No. 2708), funded by the Guilan University of Medical Sciences, Rasht, Iran.
Authors' contributions
Conceptualization and Supervision : Mohammad Reza Mobayen; Methodology: Reza Zarei; Investigation, writing - original draft and writing – review and editing : all authors; Data collection: Sanaz Masoumi, Zeinab Ghaedchukamei, Seyyed Mohammad Hossein Mazloum and Negin Rahimzadeh; Funding acquisition and resources: Mohsen Shahrousvand.
Conflict of interest
The authors declared no competing interests.
Refrences
- Aghakhani K, Mohammadi S, Molanaei A, Memarian A, Ameri M. [Epidemiologic study of scald burns in victims in Tehran burn hospital (Persian)]. Tehran Univ Med J. 2013; 71(7):452-7. http://tumj.tums.ac.ir/article-1-5497-en.html
- Alavi CE, Salehi SH, Tolouei M, Paydary K, Samidoust P, Mobayen M. Epidemiology of burn injuries at a newly established burn care center in Rasht. Trauma Mon. 2012; 17(3):341-6. [DOI:10.5812/traumamon.6991] [PMID] [PMCID]
- World Health Organization (WHO). Burns [Internet]. 2018 [Updated 2018 March 6]. Available from: https://www.who.int/news-room/fact-sheets/detail/burns
- Hinkle JL, CHeer KH. Brunner & suddarth’s text book of medical-surgical nursing. Alphen aan den Rijn: Wolters Kluwer; 2018. https://www.google.com/books/edition/Brunner_Suddarth_s_Textbook_of_Medical_s/rbEbkAEACAAJ?hl=en
- Battle CE, Evans V, James K, Guy K, Whitley J, Evans PA. Epidemiology of burns and scalds in children presenting to the emergency department of a regional burns unit: A 7-year retrospective study. Burns Trauma. 2016; 4:19. [DOI:10.1186/s41038-016-0047-7] [PMID] [PMCID]
- Balseven-Odabasi A, Tümer AR, Keten A, Yorganci K. Burn injuries among children aged up to seven years. Turk J Pediatr. 2009; 51(4):328-35. [PMID]
- Palmieri TL. Pediatric burn resuscitation. Crit Care Clin. 2016; 32(4):547-59. [DOI:10.1016/j.ccc.2016.06.004] [PMID]
- Wang, S., Li, D., Shen, C. et al. Epidemiology of burns in pediatric patients of Beijing City. BMC Pediatr. 2016; 16(1):166. [DOI:10.1186/s12887-016-0686-7] [PMID] [PMCID]
- Shi S, Yang H, Hui Y, Zhou X, Wang T, Luo Y, et al. Epidemiologic characteristics, knowledge and risk factors of unintentional burns in rural children in Zunyi, Southwest China. Sci Rep. 2016; 6:35445. [DOI:10.1038/srep35445] [PMID] [PMCID]
- Emir Alavi S, Tolouei M, Shodjaei H, Kouchakinejad L. [Epidemiology of childhood burns in children referred to Velayat Burn University Hospital of Rasht during 2008-9 (Persian)]. J Kashan Univ Med Sci (Feyz). 2011; 14(5):512-9. http://feyz.kaums.ac.ir/article-1-1087-en.html
- Knaysi GA, Crikelair GF, Cosman B. The role of nines: Its history and accuracy. Plast Reconstr Surg. 1968; 41(6):560-3. [DOI:10.1097/00006534-196806000-00008] [PMID]
- Karimi H, Montevalian A, Motabar AR, Safari R, Parvas MS, Vasigh M. Epidemiology of paediatric burns in Iran. Ann Burns Fire Disasters. 2012; 25(3):115-20. [PMID] [PMCID]
- Toon MH, Maybauer DM, Arceneaux LL, Fraser JF, Meyer W, Runge A, et al. Children with burn injuries-assessment of neglect, violence and abuse. J Inj Violence Res. 2011; 3(2):98-110. [DOI:10.5249/jivr.v3i2.91] [PMID] [PMCID]
- Kubilius D, Smailytė G, Rimdeikienė I, Malcius D, Kaikaris V, Rimdeika R. Epidemiology of paediatric burns in Lithuania: Focus on a vulnerable population exposed to the risk of scalds at home without hot tap water supply. Burns. 2014; 40(3):506-10. [DOI:10.1016/j.burns.2013.07.012] [PMID]
- Jayachandran S. The roots of gender inequality in developing countries [Internet]. 2014 [Updated 2014 August]. [DOI:10.3386/w20380]
- Jun WH, Jie X, Jun Z, Feng t, Hui HG. Comparable results of epidemiology of children with burns among different decades in a burn unit in JinZhou, China. Burns. 2011; 37(3):513-20. [DOI:10.1016/j.burns.2010.11.001] [PMID]
- Solis FF, Domic CC, Saavedra OR. Epidemiology of burns in children and adolescents from Chile’s Metropolitan Region. Rev Chil Pediatr. 85(6):690-700. [DOI:10.4067/S0370-41062014000600006] [PMID]
- Abeyasundara SL, Rajan V, Lam L, Harvey JG, Holland AJ. The changing pattern of pediatric burns. J Burn Care Res. 2011; 32(2):178-84. [DOI:10.1097/BCR.0b013e31820aada8] [PMID]
- Almarghoub MA, Alotaibi AS, Alyamani A, Alfaqeeh FA, Almehaid FF, Al-Qattan MM, et al. The epidemiology of burn injuries in saudi arabia: A systematic review. J Burn Care Res. 2020; 41(5):1122-7. [DOI:10.1093/jbcr/iraa084] [PMID]
- Liu M, Zhu H, Yan R, Yang J, Zhan R, Yu X, et al. Epidemiology and outcome analysis of 470 patients with hand burns: A five-year retrospective study in a major burn center in Southwest China. Med Sci Monit. 2020; 26:e918881. [DOI:10.12659/MSM.918881] [PMID] [PMCID]
- Alipour J, Mehdipour Y, Karimi A. Epidemiology and outcome analysis of 3030 burn patients with an ICD-10 approach. Ann Burns Fire Disasters. 2020; 33(1):3-13. [PMID] [PMCID]
- Qian W, Wang S, Wang Y, Zhang X, Liu M, Zhan R, Huang Y, He W, Luo G. Epidemiological and clinical characteristics of burns in the older person: A seven-year retrospective analysis of 693 cases at a burn center in south-west China. Burns Trauma. 2020; 8:tkz005. [DOI:10.1093/burnst/tkz005] [PMID] [PMCID]
- AbdelWahab ME, Sadaka MS, Elbana EA, Hendy AA. Evaluation of prognostic factors affecting lenght of stay in hospital and mortality rates in acute burn patients. Ann Burns Fire Disasters. 2018; 31(2):83-8. [PMID] [PMCID]
Article Type: Original Contributions |
Subject:
Epidemiology
Received: 2021/02/21 | Accepted: 2021/08/14 | Published: 2021/09/1
Received: 2021/02/21 | Accepted: 2021/08/14 | Published: 2021/09/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Contact Information
cjhr Office, Guilan University of Medical Sciences
P.O.Box 93345-41938, Rasht, Iran
Journal Tel: +9813 33335820
Publisher Tel: +9821 453 55 000
Email: cjhr.gums@gmail.com
