

Volume 7, Issue 3 (7-2022)
CJHR 2022, 7(3): 107-118 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Movahedi M, Moshirpanahi S, Mokhayeri Y, Almasian M, Bastami F. Stigma, Anxiety, Depression, and Quality of Life Among Patients With Hepatitis C in Iran. CJHR 2022; 7 (3) :107-118
URL: http://cjhr.gums.ac.ir/article-1-231-en.html
URL: http://cjhr.gums.ac.ir/article-1-231-en.html
Masoumeh Movahedi1 

 , Shiva Moshirpanahi2 , Yaser Mokhayeri3 , Mohammad Almasian4 , Fatemeh Bastami * 5
, Shiva Moshirpanahi2 , Yaser Mokhayeri3 , Mohammad Almasian4 , Fatemeh Bastami * 5
, Shiva Moshirpanahi2 , Yaser Mokhayeri3 , Mohammad Almasian4 , Fatemeh Bastami * 5
1- Social Determinants of Health Research Center, Lorestan University of Medical Sciences, Khorramabad, Iran
2- Department of Clinical psychology, School of Psychology and Educational Sciences, Kharazmi University, Tehran, Iran.
3- Cardiovascular Research Center, Shahid Rahimi Hospital, Lorestan University of Medical Sciences, Khorramabad, Iran
4- School of Medicine, Lorestan University of Medical Sciences, Khorramabad, Iran
5- Social Determinants of Health Research Center, School of Health and Nutrition, Lorestan University of Medical Sciences, Khorramabad, Iran. , Fatemeh2011bastami@gmail.com
2- Department of Clinical psychology, School of Psychology and Educational Sciences, Kharazmi University, Tehran, Iran.
3- Cardiovascular Research Center, Shahid Rahimi Hospital, Lorestan University of Medical Sciences, Khorramabad, Iran
4- School of Medicine, Lorestan University of Medical Sciences, Khorramabad, Iran
5- Social Determinants of Health Research Center, School of Health and Nutrition, Lorestan University of Medical Sciences, Khorramabad, Iran. , Fatemeh2011bastami@gmail.com
Full-Text [PDF 691 kb]
(245 Downloads)
| Abstract (HTML) (824 Views)
Full-Text: (303 Views)
1. Introduction
Hepatitis C virus (HCV) infection is one of the most important virus-caused diseases globally. In 2015, an estimated 71 million individuals were living with hepatitis C worldwide. On average, the HCV is currently affecting three percent of the world population [1]. Developing countries have the highest rates of HCV infection. The prevalence of the disease has been reported at about one percent among the Iranian population [2]. The majority of infected people are asymptomatic and can carry the virus for decades. Liver cirrhosis and Hepatocellular Carcinoma (HCC) are the most severe consequences of this chronic infection, which occurs in 20-40% of patients. HCV patients mostly develop liver failure and eventually die [3].
There are unpleasant consequences for a patient diagnosed with a serious disease such as HCV. This is especially the :::case when::: a particular disease is considered to be stigmatic. Health-related stigma is a personal experience that is characterized by feelings of deprivation, rejection, and blame [4]. Goffman has identified three types of stigma: physical stigma, such as physical illnesses and malformations, character stigma like mental illnesses or crimes, and tribal stigma such as racial or national stigma. Goffman believes that all types of stigma vary in different and specific social, cultural, and historical contexts [5, 6].
Goffman states that stigma damages a person’s reputation and value in the community. He believes the community gives negative labels to infected individuals, which poses challenges to them in their relationships with others [6, 7]. Bad labeling plays an important part in one’s experience of living with chronic illnesses, especially when there are risks of disease transmission in vulnerable populations [8]. People usually give HCV patients negative labels and blame them, regardless of their source of exposure. In many countries, HCV is viewed and symbolized as a dirty and immoral disease. Consequently, many patients have negative beliefs about the disease, as well [9].
Labels for patients with chronic diseases is a major source of one’s identity as shared by others. Stigmatized patients are at risk of being identified at any moment if their virtual identity, which is the way they should be, does not correspond with their true social identity, which is the way they are. This can create a lasting source of stress for them and may therefore encourage them to hide their true identity. Therefore, the management of stigmatic conditions is a major part of disease management that health professionals should consider in the treatments they provide [10].
Anxiety and depression are among the symptoms of hepatitis C. The prevalence of depression and anxiety in people with hepatitis C is not clear. These symptoms are thought to be due to the disease itself or the nature of the stigma associated with it [11]. The symptoms have devastating effects on the disease process and may include physical symptoms, functional impairment, reduced treatment compliance, and lower quality of life [12, 13]. Cultural attitudes affect the management of the disease among Iranian patients [14]. This is because the disease is often discovered accidentally and sometimes so late that complications have already started. Successful treatment of HCV requires management of both anxiety and depression prior to and during treatment [15]. HCV-related stigma may contribute to decreased quality of life among infected individuals because it acts as a barrier to receiving healthcare services [16].
The idea of shameful communication and deviation from what is called the norm has a long history concerning infectious diseases. The negative effects of labeling on the health of people with chronic infectious diseases such as HIV have been well documented in previous studies [17, 18, 19]. HCV-related stigma has not been explored in Iran. Studies show that stigma can have devastating effects over the course of the disease, such as augmented physical symptoms, functional impairment, reduced compliance, and decreased adherence to treatment. As a result, the quality of life may be affected, as well. Given the above information, it is important to consider the role of stigma in predicting quality of life among patients with hepatitis C. Given the high prevalence of psychiatric symptoms, especially mood and anxiety disorders among HCV patients [20], the aim of this study was to evaluate perceived stigma and its role in predicting anxiety, depression, and quality of life in patients with hepatitis C.
2. Materials and Methods
Study design and participants
The current analytic cross-sectional study was conducted in the behavioral counseling centers of three major cities in the Lorestan Province, located in the Western part of Iran, including Khorramabad, Boroujerd, and Noorabad, from May to August 2019.
In Iran, there are centers called Behavioral Disease Counseling (BDC) centers that give advice to people who engage in high-risk sexual behaviors or drug abuse. People with diseases such as AIDS, hepatitis B, and C refer to these centers to receive mental health counseling as well as other types of healthcare services such as treatment.
Sampling was performed using the multistage cluster random method. Each city was considered as a cluster and the participants were randomly selected from Behavioral Disorder Counselling (BDC) centers of the cities. The percentage of people with hepatitis C in the three cities was as follows: 60% of the patients lived in Khorramabad, 30% resided in Boroujerd, and the remaining 10% were inhabitants of Noorabad. Next, based on the population of the patients in each cluster, the required number of participants (144 individuals) were selected from the list of people infected with HCV by simple random sampling using random number tables. The inclusion criteria were being older than 18 years, having been diagnosed with HCV infection since at least one year ago, willingness to participate in the study, being aware of the illness, and having medical records at the behavioral counselling center.
Data collection
The study questionnaires were filled out by two psychologists during clinical interviews with patients diagnosed with HCV. Questionnaires for female patients were completed by a female counselor, while those for male patients were filled out by a male counselor. The Stigma Impact Scale (SIS), WHOQOL-BREF (Short Quality of Life Assessment Scale) , Beck Depression Inventory Second Edition (BDI-II), and the Beck Anxiety Inventory (BAI) were used for data collection.
The SIS scale includes 24 items designed to determine the level of stigma perception [21]. This scale has been translated into Persian through the standard two-step translation process. The framework for this scale was designated based on the modified theory of labeling [22], which states that many people have stigmatic views about groups of people with certain features. The SIS scale measures the four dimensions of perceived stigma, including social rejection (7 items), financial insecurity (3 items), internalized shame (7 items), and social isolation (7 items). Social rejection is defined as being socially discriminated against, through such acts as showing less respect. Social isolation is feelings of loneliness, inadequacy, or inferiority to others. Financial insecurity might be the result of or affected by discriminatory acts in interpersonal relationships. The experience of occupational insecurity, social insecurity, or hiding one’s illness from others may cause an inner feeling of shame. Internalized shame is defined as the acceptance and internalization of social rejection and financial insecurity can involve feelings of separation from others, self-blame, and secretiveness about the disease [21]. The items were graded on a four-point Likert scale. A score of 4 was given to the answer “Completely agree”, while “Completely disagree” was scored 1. Cronbach’s alpha for SIS subscales was in the range of 80% to 90% [21]. A high SIS score indicates a high level of perceived stigma. Item impact scores were used to quantitatively evaluate face validity. The importance of each item was multiplied by its frequency to obtain its impact score. An impact score greater than 1.5 was considered as satisfactory [23]. To verify content validity, an expert panel consisting of 10 healthcare specialists, including biostatisticians, epidemiologists, psychologists, health education experts, and infectious disease specialists examined the content validity. The participating experts work in the Lorestan University of Medical Sciences in the capital of the province, where the research project was approved and given an ethics code. The comments of the expert panel members on the necessity and relevance of the items were used to calculate the Content Validity Ratio (CVR) and the Content Validity Index (CVI), respectively. Based on the Lawshe table, statements with CVR index values higher than 0.62 were retained [24]. After calculating the CVI index values, items with scores lower than 0.79 were discarded. Cronbach’s alpha on a sample of 30 participants was 85% for the dimensions of the scale.
WHOQOL-BREF includes 26 items and four subscales. The physical health subscale contains 7 questions with a score range of 7 to 35. The psychological health subscale includes 6 questions ranging from 6 to 30. The social relationship subscale consists of 3 questions, with a score range of 3 to 15. The environmental health subscale is comprised of 8 items with a score ranging from 8 to 40. There is also the combined subscales of quality of life and general health, which are determined by questions 1 and 2. The score range for this subscale is from 2 to 10 [25].
The validity of this instrument was evaluated and reported using discriminant validity and structural validity. Nejat, et al. translated and standardized this instrument in 2006 [25]. Cronbach’s alpha was applied to assess the internal consistency of this questionnaire on a sample consisting of 30 individuals. Cronbach’s alpha was 0.82, 0.81, 0.80, and 0.68 for physical health, mental health, environmental health, and social relationships, respectively.
BDI-II consists of 21 standardized questions. Each item has 4 choices where a score of 0 to 3 indicates a normal state to severe depression, respectively. A score of 0-9 is regarded as normal, whereas a score of 10-16 indicates mild depression, a score of 17-29 indicates moderate depression and a score of 30-63 shows severe depression. Scores range from 0 to 63. This questionnaire correlates with the Hamilton rating scale of 0.71 and its one-week reassessment reliability is as high as 0.91 [26]. The psychometric properties of the split-half correlation coefficient and the test-retest coefficient with an interval of one week were 0.89 and 0.94, respectively, as measured in Iran [27]. Internal consistency (Cronbach’s alpha) was used to assess the reliability of this questionnaire. Cronbach’s alpha was 0.91 on a 30-participant sample.
BAI is a 21-item self-report instrument aiming to evaluate the severity of anxiety [28]. This test assesses the severity of anxiety during the previous week, ranging from “not at all” to “severe”. The score for each question is from 0 to 3, and the total score varies from 0 to 63, higher scores indicating greater anxiety. Each statement reflects one anxiety symptom, which is usually experienced by people who are clinically anxious or in anxiety-provoking situations. If the score is in the range of 0 to 7, the person under study has no anxiety. Low anxiety is indicated by scores from 8 to 15. A score of 16 to 25 indicates moderate anxiety. Scores between 25 and 63 suggest the presence of severe anxiety. The Cronbach’s alpha of this scale was reported to be 0.92 on a 30 person sample.
Statistical analysis
Depending on the type of variables, qualitative or quantitative characteristics, measures of central tendency, dispersion, and frequencies were calculated. Univariate and multivariate linear regression models were used to estimate the association of covariates with stigma and quality of life. In the multivariate model, stigma score covariates including age, sex, marital status, education, occupation, depression, and anxiety were entered into the model. In the multivariate regression model all the above-mentioned variables plus stigma score were entered into the model to predict the quality of life. Stata 16 was used to analyze the data at the significance level of 0.05.
3. Results
Baseline characteristics of HCV patients
The present study was conducted on 144 patients previously diagnosed with HCV. The mean age of patients was 41.1±10.1 (with an age range of 21 to 65 years) and 46.5 percent were between 36-50 years old. The majority of the patients were female (64.6%). About 71% of the patients were married, one fifth (20.1 percent) had a high school diploma, and over half of them were unemployed (55.6%). Table 1 shows baseline characteristics of the study participants.

Scores of stigma, depression, anxiety, and qulity of life
The perceived stigma Mean±SD was 66.8±1.29. The social rejection dimension achieved the highest score with Mean±SD of 23.4±0.5. The Mean±SD scores for job insecurity, internal shame, and social isolation were 8.388±0.21, 14.798±0.27, and 20.21±0.44, respectively. The Mean±SD scores for anxiety, depression, and quality of life were 21.923±1.034, 22.666±1.041, and 72.187±1.309, respectively. In terms of the frequency distribution of anxiety level, severe anxiety had the highest frequency (40.28%) (Table 2).
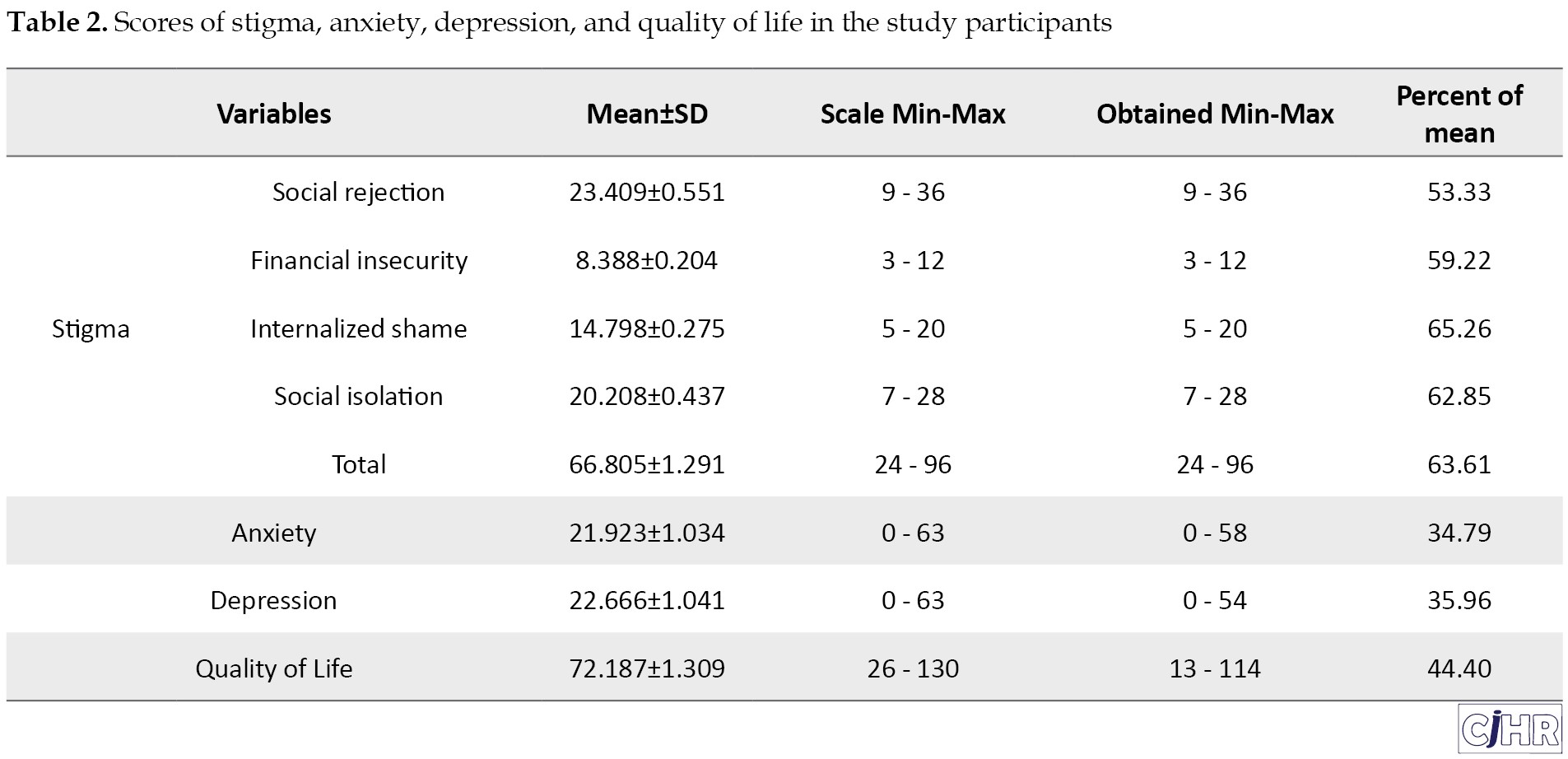
In terms of the frequency distribution of depression level, moderate depression was the most frequent (33.33%).
Results of univariate and multivariate linear regression models
Depression and anxiety were significantly associated with stigma in both the crude and multivariate regression models predicting stigma. The stigma score increased by 0.701 (95% confidence interval (CI):0.50 to 0.89) per unit increase in the depression score when adjusted for anxiety and demographic variables of the participants. Anxiety was also significantly associated with stigma. The stigma score increased by 0.211 (95% CI: 0.017 to 0.40) for each additional increase in anxiety score (Table 3).
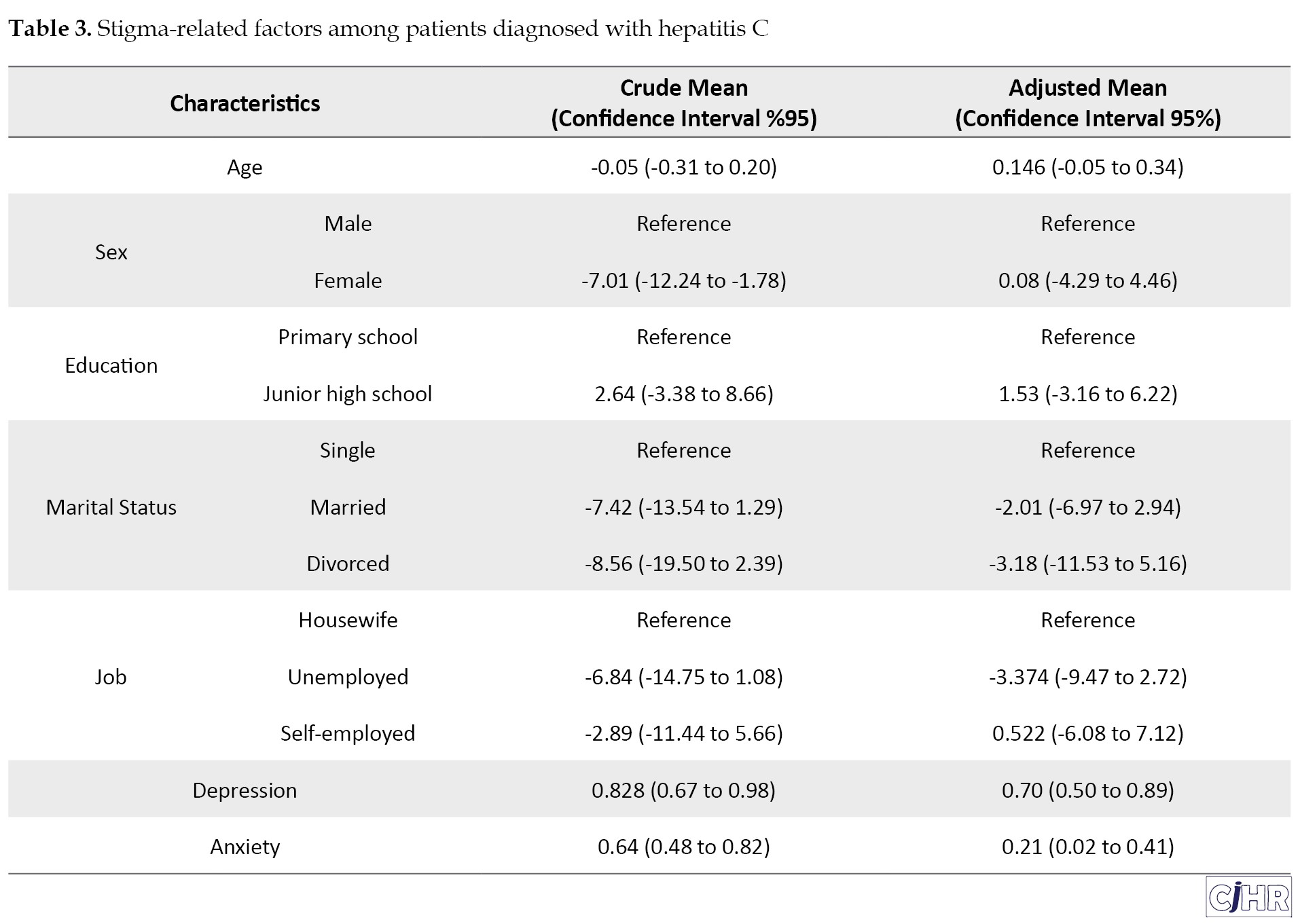
Age, sex, marital status, education, and occupation were not significant predictors of stigma.
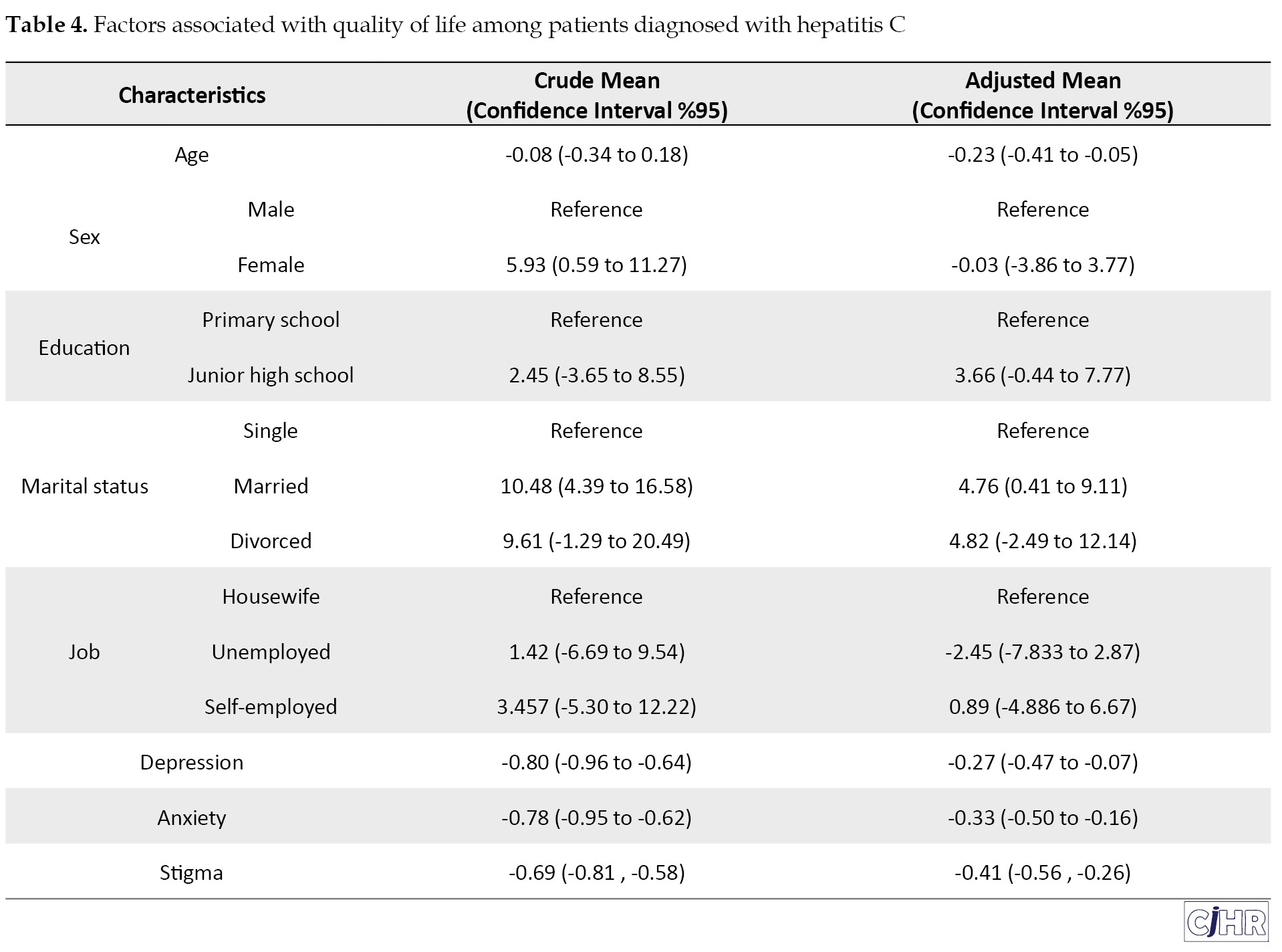
In the model predicting quality of life, marital status, depression, anxiety, and stigma were significant independent predictors of quality of life. The mean score of quality of life decreased with each additional increase in depression (-0.27, 95% CI: -0.47 to -0.07), anxiety (-0.33, 95% CI: -0.5, -0.16), and stigma scores (-0.41, 95% CI:-0.56, -0.26) when adjusted for age, sex, marital status, and occupation (Table 4).
4. Discussion
This study showed that patients with hepatitis C had high stigma scores. The mean perceived stigma was 66.805±1.291, with social rejection having the highest score among the dimensions of stigma. A higher score for perceived stigma indicates that the person has worse experiences. The stigma score of the study population in the current study was much higher than previous studies conducted on patients with mental disorders in Iran that was 51.2±55. Perceived stigma was inversely correlated with hope, self-esteem, self-efficacy, and adherence to treatment. In other words, perceived stigma reduced the value of these variables among individuals [29]. According to a qualitative study conducted on HIV patients in Iran, patients experienced three types of stigma, including isolation, shame, and feelings of unhappiness [30]. Likewise, a qualitative study on HIV patients in Tehran, the capital city of Iran, showed that patients experienced four types of stigma including refusal to offer care, subpar care, disproportionate precautions, and physical distancing by healthcare providers, as well as feelings of humiliation and self-blame [31]. Since these findings are similar to the results of the present study, it can be said that cultural factors seem to influence the findings. Another previous study in Tehran, Iran, mentioned that high stigma levels might reflect the religious, cultural, and social views and conditions regarding HIV patients [32].
In the present study, social rejection and social isolation obtained the highest scores as dimensions of perceived stigma, indicating the worst condtions. In line with previous studies, perceived stigma in HCV patients can result in excessive anxiety of being infected experienced by people in touch with the patients, and this can greatly contribute to higher social isolation and decreased closeness and intimacy in relationships [33, 34].
In the present study, gender was not independently associated with stigma. In previous studies in the United States and Australia, women experienced significantly more stigma than men in the community [34, 35]. Consistent with the current study, previous studies in Egypt and Pakistan have not found such an association among people with perceived hepatitis C-related stigma [33, 36]. In line with previous studies in Egypt and the United States, there was no significant relationship between HCV stigma and demographic variables such as education, age, and marital status [33, 34].
Similar to AIDS another blood-borne disease, hepatitis C carries the risk of stigmatization [35, 36]. Although HCV infection is not easily transmitted, people normally avoid infected individuals. Fear and ignorance of people in the community may entail adversities, including job loss, negative impact on social relationships, reduced quality of life, and the development of mental illnesses, such as anxiety and depression [37].
According to previous studies, HIV-positive patients experience stigma in the form of social rejection, avoidance, shame, and the fear of disclosure of the disease. However, hiding such diseases can lead to reduced social support, development of mental disorders, inability to work, financial problems, and inadequate medical treatment. High stigma is associated with noncompliance with antiviral treatment, increased psychological distress (e.g. depression, anxiety, hopelessness), and problems in receiving proper medical treatment [38, 39]. In our study, depression and anxiety were independently associated with stigma, when the model was adjusted for age, sex, marital status, and job. Based on previous studies, aspects of perceived stigma include social rejection, isolation, occupational insecurity, and internalized shame, which are predictors of low self-worth, which can increase anxiety and depression, and reduce adaptation to the disease [40, 41, 42]. The results of previous studies showed that people with chronic diseases, such as AIDS and lung cancer, experience a relatively high level of stigma which is significantly associated with psychological disorders, such as anxiety and depression [33, 43, 44, 45]. Depression will lead to a gloomy attitude towards the world and future, and this will eventually create negative cognitive schemas in these people. The attitudes of other people in society make patients evaluate themselves positively or negatively [46]. The more infected people think about hepatitis C, the more likely it is that they will endanger their social and individual status, and this will lead them to isolation and thus feelings of loneliness and anxiety [35]. According to Beck’s cognitive theory, hepatitis C patients make negative interpretations of life events because they use negative speculative beliefs as interpretive filters to understand these events [46]. In fact, the negative view of the community about patients with hepatitis C causes them to make cognitive errors in specific situations. On the other hand, the more these people are accepted by society and family and away from disgraceful and destructive thoughts about the disease, the more positive their views and attitudes toward life will be and this will help them accept the disease. As a result, they perform self-care behaviors, show high resilience, are hopeful for the future, and are thus happier and less depressed [47].
In the current study, depression, anxiety, and stigma were inversely associated with patients’ quality of life. The effects of disease on quality of life can mainly be explained by perceived stigma. An increase in the perceived severity of the disease is associated with a decrease in the functional dimensions of quality of life, including bodily health, mental well-being, social relationships, and living environments, which in turn results in increased perceived stigma. This is because when perceived severity of illness increases, it will be difficult to cover it up and individual differences become more apparent to others. Likewise, if the disease is believed to be more severe, patients will be less able to participate in social activities of normal life which makes them more isolated and makes them feel excluded from society [48, 49, 50]. The diagnosis of hepatitis C has multi-dimensional effects on social functioning. HCV patients are usually identified and subsequently considered as abnormal and deviant [16]. In addition, the infection itself may cause the community to experience exaggerated fears of contact with patients, so that people will start avoiding infected individuals who have already been identified. As such, the resulting stigma may work as a major cause of social isolation and reduced intimacy among the infected individuals [40].
Using structured clinical interviews, a study conducted in Ireland on HCV-infected individuals under treatment showed that 28% of the patients suffered from depression and 24% suffered from an anxiety disorder. In these individuals, failure to accept the disease, perceived stigma regarding the disease, poor concentration and thinking, and higher levels of physical and mental symptoms were present [51]. The results of this study showed that depression and anxiety were highly prevalent among patients with hepatitis C, and were not recognized and treated. A systematic review that was conducted on published quantitative and qualitative studies about the quality of life of patients suffering from hepatitis using the mixed methods approach in 26 countries showed that the unfulfilled needs of patients due to perceived stigma dramatically affected the quality of their lives [52].
The Iranian Ministry of Health has declared that prejudice and the general negative attitudes of the public to individuals infected with HIV leads to stigma and feelings of discrimination, which increase high-risk behaviors among these individuals. Additionally, depression and anxiety, which are among the consequences of stigma, considerably affect the quality of life of the affected individuals. This, in turn, can adversely affect the functioning of the immune system and intensify chronic pains. It can also interfere with compliance with anti-retroviral therapy. In some cases, the resultant depression accompanies high-risk behaviors, such as alcohol and substance abuse, resulting in increased transmission of the disease to other individuals [34, 53].
There are a number of strong points in the present study. This is the first time that perceived stigma associated with hepatitis C disease has been investigated in Iran. Nonetheless, there were limitations as well. The cross-sectional nature of the study did not allow the longitudinal assessment of study variables. Moreover, due to the limited number of studies on this topic in Iran, we had to compare our findings with studies conducted elsewhere. Furthermore, no data was collected on the infection mode or treatment methods offered to the patients. Therefore, it is suggested that the source of infection be considered in examining the perceived stigma of incurable blood-borne diseases.
5. Conclusion
In this study, perceived stigma high scores were observed among HCV patients. Depression and anxiety were significantly associated with stigma. The quality of life of HCV patients was inversely associated with depression, anxiety, and stigma scores. It is suggested that psychologists working in mental health centers inform family, friends, and colleagues of patients with hepatitis C about the role of stigmatization and its effects on the quality of life of patients.
Ethical Considerations
Compliance with ethical guidelines
This study was conducted after obtaining the approval of the Ethics Committee of the Lorestan University of Medical Sciences, Lorestan, Iran (approval code: IR.LUMS.REC.1395.1130). The duties and obligations of the project implementer and their expectations from the participants were explained to the participants. Ethical standards such as free participation in research, confidentiality of information, and psychological and physical security of patients during the interview were explained to the participants and observed.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design: Masoumeh Movahedi, Shiva Moshirpanahi; Data collection: Masoumeh Movahedi; Manuscript: Yaser Mokhayeri, Fatemeh Bastami; Revision of the manuscript: Fatemeh Bastami, Mohammad Almasian, Yaser Mokhayeri.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The researchers would like to express their gratitude to the study participants and the staff of the health centers in Lorestan, Iran.
References
Hepatitis C virus (HCV) infection is one of the most important virus-caused diseases globally. In 2015, an estimated 71 million individuals were living with hepatitis C worldwide. On average, the HCV is currently affecting three percent of the world population [1]. Developing countries have the highest rates of HCV infection. The prevalence of the disease has been reported at about one percent among the Iranian population [2]. The majority of infected people are asymptomatic and can carry the virus for decades. Liver cirrhosis and Hepatocellular Carcinoma (HCC) are the most severe consequences of this chronic infection, which occurs in 20-40% of patients. HCV patients mostly develop liver failure and eventually die [3].
There are unpleasant consequences for a patient diagnosed with a serious disease such as HCV. This is especially the :::case when::: a particular disease is considered to be stigmatic. Health-related stigma is a personal experience that is characterized by feelings of deprivation, rejection, and blame [4]. Goffman has identified three types of stigma: physical stigma, such as physical illnesses and malformations, character stigma like mental illnesses or crimes, and tribal stigma such as racial or national stigma. Goffman believes that all types of stigma vary in different and specific social, cultural, and historical contexts [5, 6].
Goffman states that stigma damages a person’s reputation and value in the community. He believes the community gives negative labels to infected individuals, which poses challenges to them in their relationships with others [6, 7]. Bad labeling plays an important part in one’s experience of living with chronic illnesses, especially when there are risks of disease transmission in vulnerable populations [8]. People usually give HCV patients negative labels and blame them, regardless of their source of exposure. In many countries, HCV is viewed and symbolized as a dirty and immoral disease. Consequently, many patients have negative beliefs about the disease, as well [9].
Labels for patients with chronic diseases is a major source of one’s identity as shared by others. Stigmatized patients are at risk of being identified at any moment if their virtual identity, which is the way they should be, does not correspond with their true social identity, which is the way they are. This can create a lasting source of stress for them and may therefore encourage them to hide their true identity. Therefore, the management of stigmatic conditions is a major part of disease management that health professionals should consider in the treatments they provide [10].
Anxiety and depression are among the symptoms of hepatitis C. The prevalence of depression and anxiety in people with hepatitis C is not clear. These symptoms are thought to be due to the disease itself or the nature of the stigma associated with it [11]. The symptoms have devastating effects on the disease process and may include physical symptoms, functional impairment, reduced treatment compliance, and lower quality of life [12, 13]. Cultural attitudes affect the management of the disease among Iranian patients [14]. This is because the disease is often discovered accidentally and sometimes so late that complications have already started. Successful treatment of HCV requires management of both anxiety and depression prior to and during treatment [15]. HCV-related stigma may contribute to decreased quality of life among infected individuals because it acts as a barrier to receiving healthcare services [16].
The idea of shameful communication and deviation from what is called the norm has a long history concerning infectious diseases. The negative effects of labeling on the health of people with chronic infectious diseases such as HIV have been well documented in previous studies [17, 18, 19]. HCV-related stigma has not been explored in Iran. Studies show that stigma can have devastating effects over the course of the disease, such as augmented physical symptoms, functional impairment, reduced compliance, and decreased adherence to treatment. As a result, the quality of life may be affected, as well. Given the above information, it is important to consider the role of stigma in predicting quality of life among patients with hepatitis C. Given the high prevalence of psychiatric symptoms, especially mood and anxiety disorders among HCV patients [20], the aim of this study was to evaluate perceived stigma and its role in predicting anxiety, depression, and quality of life in patients with hepatitis C.
2. Materials and Methods
Study design and participants
The current analytic cross-sectional study was conducted in the behavioral counseling centers of three major cities in the Lorestan Province, located in the Western part of Iran, including Khorramabad, Boroujerd, and Noorabad, from May to August 2019.
In Iran, there are centers called Behavioral Disease Counseling (BDC) centers that give advice to people who engage in high-risk sexual behaviors or drug abuse. People with diseases such as AIDS, hepatitis B, and C refer to these centers to receive mental health counseling as well as other types of healthcare services such as treatment.
Sampling was performed using the multistage cluster random method. Each city was considered as a cluster and the participants were randomly selected from Behavioral Disorder Counselling (BDC) centers of the cities. The percentage of people with hepatitis C in the three cities was as follows: 60% of the patients lived in Khorramabad, 30% resided in Boroujerd, and the remaining 10% were inhabitants of Noorabad. Next, based on the population of the patients in each cluster, the required number of participants (144 individuals) were selected from the list of people infected with HCV by simple random sampling using random number tables. The inclusion criteria were being older than 18 years, having been diagnosed with HCV infection since at least one year ago, willingness to participate in the study, being aware of the illness, and having medical records at the behavioral counselling center.
Data collection
The study questionnaires were filled out by two psychologists during clinical interviews with patients diagnosed with HCV. Questionnaires for female patients were completed by a female counselor, while those for male patients were filled out by a male counselor. The Stigma Impact Scale (SIS), WHOQOL-BREF (Short Quality of Life Assessment Scale) , Beck Depression Inventory Second Edition (BDI-II), and the Beck Anxiety Inventory (BAI) were used for data collection.
The SIS scale includes 24 items designed to determine the level of stigma perception [21]. This scale has been translated into Persian through the standard two-step translation process. The framework for this scale was designated based on the modified theory of labeling [22], which states that many people have stigmatic views about groups of people with certain features. The SIS scale measures the four dimensions of perceived stigma, including social rejection (7 items), financial insecurity (3 items), internalized shame (7 items), and social isolation (7 items). Social rejection is defined as being socially discriminated against, through such acts as showing less respect. Social isolation is feelings of loneliness, inadequacy, or inferiority to others. Financial insecurity might be the result of or affected by discriminatory acts in interpersonal relationships. The experience of occupational insecurity, social insecurity, or hiding one’s illness from others may cause an inner feeling of shame. Internalized shame is defined as the acceptance and internalization of social rejection and financial insecurity can involve feelings of separation from others, self-blame, and secretiveness about the disease [21]. The items were graded on a four-point Likert scale. A score of 4 was given to the answer “Completely agree”, while “Completely disagree” was scored 1. Cronbach’s alpha for SIS subscales was in the range of 80% to 90% [21]. A high SIS score indicates a high level of perceived stigma. Item impact scores were used to quantitatively evaluate face validity. The importance of each item was multiplied by its frequency to obtain its impact score. An impact score greater than 1.5 was considered as satisfactory [23]. To verify content validity, an expert panel consisting of 10 healthcare specialists, including biostatisticians, epidemiologists, psychologists, health education experts, and infectious disease specialists examined the content validity. The participating experts work in the Lorestan University of Medical Sciences in the capital of the province, where the research project was approved and given an ethics code. The comments of the expert panel members on the necessity and relevance of the items were used to calculate the Content Validity Ratio (CVR) and the Content Validity Index (CVI), respectively. Based on the Lawshe table, statements with CVR index values higher than 0.62 were retained [24]. After calculating the CVI index values, items with scores lower than 0.79 were discarded. Cronbach’s alpha on a sample of 30 participants was 85% for the dimensions of the scale.
WHOQOL-BREF includes 26 items and four subscales. The physical health subscale contains 7 questions with a score range of 7 to 35. The psychological health subscale includes 6 questions ranging from 6 to 30. The social relationship subscale consists of 3 questions, with a score range of 3 to 15. The environmental health subscale is comprised of 8 items with a score ranging from 8 to 40. There is also the combined subscales of quality of life and general health, which are determined by questions 1 and 2. The score range for this subscale is from 2 to 10 [25].
The validity of this instrument was evaluated and reported using discriminant validity and structural validity. Nejat, et al. translated and standardized this instrument in 2006 [25]. Cronbach’s alpha was applied to assess the internal consistency of this questionnaire on a sample consisting of 30 individuals. Cronbach’s alpha was 0.82, 0.81, 0.80, and 0.68 for physical health, mental health, environmental health, and social relationships, respectively.
BDI-II consists of 21 standardized questions. Each item has 4 choices where a score of 0 to 3 indicates a normal state to severe depression, respectively. A score of 0-9 is regarded as normal, whereas a score of 10-16 indicates mild depression, a score of 17-29 indicates moderate depression and a score of 30-63 shows severe depression. Scores range from 0 to 63. This questionnaire correlates with the Hamilton rating scale of 0.71 and its one-week reassessment reliability is as high as 0.91 [26]. The psychometric properties of the split-half correlation coefficient and the test-retest coefficient with an interval of one week were 0.89 and 0.94, respectively, as measured in Iran [27]. Internal consistency (Cronbach’s alpha) was used to assess the reliability of this questionnaire. Cronbach’s alpha was 0.91 on a 30-participant sample.
BAI is a 21-item self-report instrument aiming to evaluate the severity of anxiety [28]. This test assesses the severity of anxiety during the previous week, ranging from “not at all” to “severe”. The score for each question is from 0 to 3, and the total score varies from 0 to 63, higher scores indicating greater anxiety. Each statement reflects one anxiety symptom, which is usually experienced by people who are clinically anxious or in anxiety-provoking situations. If the score is in the range of 0 to 7, the person under study has no anxiety. Low anxiety is indicated by scores from 8 to 15. A score of 16 to 25 indicates moderate anxiety. Scores between 25 and 63 suggest the presence of severe anxiety. The Cronbach’s alpha of this scale was reported to be 0.92 on a 30 person sample.
Statistical analysis
Depending on the type of variables, qualitative or quantitative characteristics, measures of central tendency, dispersion, and frequencies were calculated. Univariate and multivariate linear regression models were used to estimate the association of covariates with stigma and quality of life. In the multivariate model, stigma score covariates including age, sex, marital status, education, occupation, depression, and anxiety were entered into the model. In the multivariate regression model all the above-mentioned variables plus stigma score were entered into the model to predict the quality of life. Stata 16 was used to analyze the data at the significance level of 0.05.
3. Results
Baseline characteristics of HCV patients
The present study was conducted on 144 patients previously diagnosed with HCV. The mean age of patients was 41.1±10.1 (with an age range of 21 to 65 years) and 46.5 percent were between 36-50 years old. The majority of the patients were female (64.6%). About 71% of the patients were married, one fifth (20.1 percent) had a high school diploma, and over half of them were unemployed (55.6%). Table 1 shows baseline characteristics of the study participants.
Scores of stigma, depression, anxiety, and qulity of life
The perceived stigma Mean±SD was 66.8±1.29. The social rejection dimension achieved the highest score with Mean±SD of 23.4±0.5. The Mean±SD scores for job insecurity, internal shame, and social isolation were 8.388±0.21, 14.798±0.27, and 20.21±0.44, respectively. The Mean±SD scores for anxiety, depression, and quality of life were 21.923±1.034, 22.666±1.041, and 72.187±1.309, respectively. In terms of the frequency distribution of anxiety level, severe anxiety had the highest frequency (40.28%) (Table 2).
In terms of the frequency distribution of depression level, moderate depression was the most frequent (33.33%).
Results of univariate and multivariate linear regression models
Depression and anxiety were significantly associated with stigma in both the crude and multivariate regression models predicting stigma. The stigma score increased by 0.701 (95% confidence interval (CI):0.50 to 0.89) per unit increase in the depression score when adjusted for anxiety and demographic variables of the participants. Anxiety was also significantly associated with stigma. The stigma score increased by 0.211 (95% CI: 0.017 to 0.40) for each additional increase in anxiety score (Table 3).
Age, sex, marital status, education, and occupation were not significant predictors of stigma.
In the model predicting quality of life, marital status, depression, anxiety, and stigma were significant independent predictors of quality of life. The mean score of quality of life decreased with each additional increase in depression (-0.27, 95% CI: -0.47 to -0.07), anxiety (-0.33, 95% CI: -0.5, -0.16), and stigma scores (-0.41, 95% CI:-0.56, -0.26) when adjusted for age, sex, marital status, and occupation (Table 4).
4. Discussion
This study showed that patients with hepatitis C had high stigma scores. The mean perceived stigma was 66.805±1.291, with social rejection having the highest score among the dimensions of stigma. A higher score for perceived stigma indicates that the person has worse experiences. The stigma score of the study population in the current study was much higher than previous studies conducted on patients with mental disorders in Iran that was 51.2±55. Perceived stigma was inversely correlated with hope, self-esteem, self-efficacy, and adherence to treatment. In other words, perceived stigma reduced the value of these variables among individuals [29]. According to a qualitative study conducted on HIV patients in Iran, patients experienced three types of stigma, including isolation, shame, and feelings of unhappiness [30]. Likewise, a qualitative study on HIV patients in Tehran, the capital city of Iran, showed that patients experienced four types of stigma including refusal to offer care, subpar care, disproportionate precautions, and physical distancing by healthcare providers, as well as feelings of humiliation and self-blame [31]. Since these findings are similar to the results of the present study, it can be said that cultural factors seem to influence the findings. Another previous study in Tehran, Iran, mentioned that high stigma levels might reflect the religious, cultural, and social views and conditions regarding HIV patients [32].
In the present study, social rejection and social isolation obtained the highest scores as dimensions of perceived stigma, indicating the worst condtions. In line with previous studies, perceived stigma in HCV patients can result in excessive anxiety of being infected experienced by people in touch with the patients, and this can greatly contribute to higher social isolation and decreased closeness and intimacy in relationships [33, 34].
In the present study, gender was not independently associated with stigma. In previous studies in the United States and Australia, women experienced significantly more stigma than men in the community [34, 35]. Consistent with the current study, previous studies in Egypt and Pakistan have not found such an association among people with perceived hepatitis C-related stigma [33, 36]. In line with previous studies in Egypt and the United States, there was no significant relationship between HCV stigma and demographic variables such as education, age, and marital status [33, 34].
Similar to AIDS another blood-borne disease, hepatitis C carries the risk of stigmatization [35, 36]. Although HCV infection is not easily transmitted, people normally avoid infected individuals. Fear and ignorance of people in the community may entail adversities, including job loss, negative impact on social relationships, reduced quality of life, and the development of mental illnesses, such as anxiety and depression [37].
According to previous studies, HIV-positive patients experience stigma in the form of social rejection, avoidance, shame, and the fear of disclosure of the disease. However, hiding such diseases can lead to reduced social support, development of mental disorders, inability to work, financial problems, and inadequate medical treatment. High stigma is associated with noncompliance with antiviral treatment, increased psychological distress (e.g. depression, anxiety, hopelessness), and problems in receiving proper medical treatment [38, 39]. In our study, depression and anxiety were independently associated with stigma, when the model was adjusted for age, sex, marital status, and job. Based on previous studies, aspects of perceived stigma include social rejection, isolation, occupational insecurity, and internalized shame, which are predictors of low self-worth, which can increase anxiety and depression, and reduce adaptation to the disease [40, 41, 42]. The results of previous studies showed that people with chronic diseases, such as AIDS and lung cancer, experience a relatively high level of stigma which is significantly associated with psychological disorders, such as anxiety and depression [33, 43, 44, 45]. Depression will lead to a gloomy attitude towards the world and future, and this will eventually create negative cognitive schemas in these people. The attitudes of other people in society make patients evaluate themselves positively or negatively [46]. The more infected people think about hepatitis C, the more likely it is that they will endanger their social and individual status, and this will lead them to isolation and thus feelings of loneliness and anxiety [35]. According to Beck’s cognitive theory, hepatitis C patients make negative interpretations of life events because they use negative speculative beliefs as interpretive filters to understand these events [46]. In fact, the negative view of the community about patients with hepatitis C causes them to make cognitive errors in specific situations. On the other hand, the more these people are accepted by society and family and away from disgraceful and destructive thoughts about the disease, the more positive their views and attitudes toward life will be and this will help them accept the disease. As a result, they perform self-care behaviors, show high resilience, are hopeful for the future, and are thus happier and less depressed [47].
In the current study, depression, anxiety, and stigma were inversely associated with patients’ quality of life. The effects of disease on quality of life can mainly be explained by perceived stigma. An increase in the perceived severity of the disease is associated with a decrease in the functional dimensions of quality of life, including bodily health, mental well-being, social relationships, and living environments, which in turn results in increased perceived stigma. This is because when perceived severity of illness increases, it will be difficult to cover it up and individual differences become more apparent to others. Likewise, if the disease is believed to be more severe, patients will be less able to participate in social activities of normal life which makes them more isolated and makes them feel excluded from society [48, 49, 50]. The diagnosis of hepatitis C has multi-dimensional effects on social functioning. HCV patients are usually identified and subsequently considered as abnormal and deviant [16]. In addition, the infection itself may cause the community to experience exaggerated fears of contact with patients, so that people will start avoiding infected individuals who have already been identified. As such, the resulting stigma may work as a major cause of social isolation and reduced intimacy among the infected individuals [40].
Using structured clinical interviews, a study conducted in Ireland on HCV-infected individuals under treatment showed that 28% of the patients suffered from depression and 24% suffered from an anxiety disorder. In these individuals, failure to accept the disease, perceived stigma regarding the disease, poor concentration and thinking, and higher levels of physical and mental symptoms were present [51]. The results of this study showed that depression and anxiety were highly prevalent among patients with hepatitis C, and were not recognized and treated. A systematic review that was conducted on published quantitative and qualitative studies about the quality of life of patients suffering from hepatitis using the mixed methods approach in 26 countries showed that the unfulfilled needs of patients due to perceived stigma dramatically affected the quality of their lives [52].
The Iranian Ministry of Health has declared that prejudice and the general negative attitudes of the public to individuals infected with HIV leads to stigma and feelings of discrimination, which increase high-risk behaviors among these individuals. Additionally, depression and anxiety, which are among the consequences of stigma, considerably affect the quality of life of the affected individuals. This, in turn, can adversely affect the functioning of the immune system and intensify chronic pains. It can also interfere with compliance with anti-retroviral therapy. In some cases, the resultant depression accompanies high-risk behaviors, such as alcohol and substance abuse, resulting in increased transmission of the disease to other individuals [34, 53].
There are a number of strong points in the present study. This is the first time that perceived stigma associated with hepatitis C disease has been investigated in Iran. Nonetheless, there were limitations as well. The cross-sectional nature of the study did not allow the longitudinal assessment of study variables. Moreover, due to the limited number of studies on this topic in Iran, we had to compare our findings with studies conducted elsewhere. Furthermore, no data was collected on the infection mode or treatment methods offered to the patients. Therefore, it is suggested that the source of infection be considered in examining the perceived stigma of incurable blood-borne diseases.
5. Conclusion
In this study, perceived stigma high scores were observed among HCV patients. Depression and anxiety were significantly associated with stigma. The quality of life of HCV patients was inversely associated with depression, anxiety, and stigma scores. It is suggested that psychologists working in mental health centers inform family, friends, and colleagues of patients with hepatitis C about the role of stigmatization and its effects on the quality of life of patients.
Ethical Considerations
Compliance with ethical guidelines
This study was conducted after obtaining the approval of the Ethics Committee of the Lorestan University of Medical Sciences, Lorestan, Iran (approval code: IR.LUMS.REC.1395.1130). The duties and obligations of the project implementer and their expectations from the participants were explained to the participants. Ethical standards such as free participation in research, confidentiality of information, and psychological and physical security of patients during the interview were explained to the participants and observed.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design: Masoumeh Movahedi, Shiva Moshirpanahi; Data collection: Masoumeh Movahedi; Manuscript: Yaser Mokhayeri, Fatemeh Bastami; Revision of the manuscript: Fatemeh Bastami, Mohammad Almasian, Yaser Mokhayeri.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The researchers would like to express their gratitude to the study participants and the staff of the health centers in Lorestan, Iran.
References
- World Hepatitis Day- July 28, 2019. MMWR Morb Mortal Wkly Rep. 2019; 68(29):637. [DOI:10.15585/mmwr.mm6829a1] [PMID] [PMCID]
- Mahmud S, Akbarzadeh V, Abu-Raddad LJ. The epidemiology of hepatitis C virus in Iran: Systematic review and meta-analyses. Sci Rep. 2018; 8(1):150. [DOI:10.1038/s41598-017-18296-9] [PMID] [PMCID]
- Lions C, Laroche H, Zaegel-Faucher O, Ressiot E, Bregigeon S, Geneau de Lamarliere P, et al. Hepatitis C virus-microelimination program and patient trajectories after hepatitis C virus cure in an outpatient HIV clinical unit. Eur J Gastroenterol Hepatol. 2020; 32(9):1212-21. [DOI:10.2139/ssrn.3378701]
- Sheehan L, Nieweglowski K, Corrigan P. The stigma of personality disorders. Curr Psychiatry Rep. 2016; 18(1):11. [DOI:10.1007/s11920-015-0654-1] [PMID]
- Bates L, Stickley T. Confronting Goffman: how can mental health nurses effectively challenge stigma? A critical review of the literature. J Psychiatr Ment Health Nurs. 2013; 20(7):569-75. [DOI:10.1111/j.1365-2850.2012.01957.x] [PMID]
- Goffman E. Stigma: Notes on the management of spoiled identity. New York: Simon and Schuster; 2009. https://books.google.com/books/about/Stigma.html?id=zuMFXuTMAqAC
- Cruz ML, Bastos FI, Darmont M, Dickstein P, Monteiro S. The “moral career” of perinatally HIV-infected children: revisiting Goffman’s concept. AIDS care. 2015; 27(1):6-9. [DOI:10.1080/09540121.2014.940270] [PMID]
- Judgeo N, Moalusi KP. My secret: the social meaning of HIV/AIDS stigma. SAHARA J. 2014; 11(1):76-83. [DOI:10.1080/17290376.2014.932302] [PMID] [PMCID]
- Butt G, Paterson BL, McGuinness LK. Living with the stigma of hepatitis C. West J Nurs Res. 2008; 30(2):204-21. [DOI:10.1177/0193945907302771] [PMID]
- Pachankis JE, Hatzenbuehler ML, Wang K, Burton CL, Crawford FW, Phelan JC, et al. The Burden of stigma on health and well-being: A taxonomy of concealment, course, disruptiveness, aesthetics, origin, and peril across 93 stigmas. Pers Soc Psychol Bullv. 2018; 44(4):451-74. [DOI:10.1177/0146167217741313] [PMID] [PMCID]
- Deterding K, Gruner N, Buggisch P, Galle PR, Spengler U, Hinrichsen H, et al. Symptoms of anxiety and depression are frequent in patients with acute hepatitis C and are not associated with disease severity. Eur J Gastroenterol Hepatol. 2016; 28(2):187-92. [DOI:10.1097/MEG.0000000000000517] [PMID]
- Gallach M, Vergara M, da Costa JP, Miquel M, Casas M, Sanchez-Delgado J, et al. Impact of treatment with direct-acting antivirals on anxiety and depression in chronic hepatitis C. PloS one. 2018; 13(12):e0208112. [DOI:10.1371/journal.pone.0208112] [PMID] [PMCID]
- Didehvar M, Zareban I, Jalili Z, Bakhshani N-M, Shahrakipoor M, Balouchi A. The effect of stress management training through PRECEDE-PROCEED model on occupational stress among nurses and midwives at Iran hospital, Iranshahr. J Clin Diagn Res. 2016; 10(10):LC01-5. [DOI:10.7860/JCDR/2016/22569.8674] [PMID] [PMCID]
- Davoodi L, Masoum B, Moosazadeh M, Jafarpour H, Haghshenas MR, Mousavi T. Psychiatric side effects of pegylated interferon-alpha and ribavirin therapy in Iranian patients with chronic hepatitis C: A meta-analysis. Exp Ther Med. 2018; 16(2):971-8. [DOI:10.3892/etm.2018.6255] [PMID] [PMCID]
- Ashrafi M, Modabbernia A, Dalir M, Taslimi S, Karami M, Ostovaneh MR, et al. Predictors of mental and physical health in non-cirrhotic patients with viral hepatitis: a case control study. J Psychosom Res. 2012; 73(3):218-24. [DOI:10.1016/j.jpsychores.2012.06.006] [PMID]
- Northrop JM. A dirty little secret: stigma, shame and hepatitis C in the health setting. Med Humanit. 2017; 43(4):218-24. [DOI:10.1136/medhum-2016-011099] [PMID]
- Alexandra Marshall S, Brewington KM, Kathryn Allison M, Haynes TF, Zaller ND. Measuring HIV-related stigma among healthcare providers: A systematic review. AIDS care. 2017; 29(11):1337-45. [DOI:10.1080/09540121.2017.1338654] [PMID]
- Rueda S, Mitra S, Chen S, Gogolishvili D, Globerman J, Chambers L, et al. Examining the associations between HIV-related stigma and health outcomes in people living with HIV/AIDS: a series of meta-analyses. BMJ Open. 2016; 6(7):e011453. [DOI:10.1136/bmjopen-2016-011453] [PMID] [PMCID]
- Rutledge SE, Abell N, Padmore J, McCann TJ. AIDS stigma in health services in the Eastern Caribbean. Sociol Health Illn. 2009; 31(1):17-34. [DOI:10.1111/j.1467-9566.2008.01133.x] [PMID]
- Fortier E, Alavi M, Bruneau J, Micallef M, Perram J, Sockalingam S, et al. Depression, anxiety, and stress among people with chronic hepatitis C virus infection and a history of injecting drug use in New South Wales, Australia. J Addict Med. 2017; 11(1):10-8. [DOI:10.1097/ADM.0000000000000261] [PMID]
- Fife BL, Wright ER. The dimensionality of stigma: A comparison of its impact on the self of persons with HIV/AIDS and cancer. J Health Soc Behav. 2000; 41(1):50-67. [DOI:10.2307/2676360] [PMID]
- Link BG, Phelan JC. Labeling and stigma. In: Aneshensel CS, Phelan JC, Bierman A, editors. Handbook of the sociology of mental health. Netherlands: Springer; 2013. [DOI:10.1007/978-94-007-4276-5_25]
- Sartori R. Face validity in personality tests: psychometric instruments and projective techniques in comparison. Qual Quant. 2010; 44(4):749-59. [DOI:10.1007/s11135-009-9224-0]
- Skevington SM, Lotfy M, O’Connell KA. The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. 2004; 13(2):299-310. [DOI:10.1023/B:QURE.0000018486.91360.00] [PMID]
- Nejat S, Montazeri A, Holakouie Naieni K, Mohammad K, Majdzadeh S. [The World Health Organization quality of Life (WHOQOL-BREF) questionnaire: Translation and validation study of the Iranian version (Persian)]. J Sch Public Health Inst Public Health Res. 2006; 4(4):1-12. https://sjsph.tums.ac.ir/browse.php?a_code=A-10-25-187&slc_lang=en&sid=1
- Wang YP, Gorenstein C. Psychometric properties of the Beck Depression Inventory-II: A comprehensive review. Braz J Psychiatry. 2013; 35(4):416-31. [DOI:10.1590/1516-4446-2012-1048] [PMID]
- Mousavi SA, Aghayan S, Razavianzadeh N, Nourouzi N, Khosravi A. [Depression and general health status in type ii diabetic patients (Persian)]. Knowl Health. 2008; 3(1):44-8. https://www.sid.ir/en/Journal/ViewPaper.aspx?ID=137864
- Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: Psychometric properties. J Consult Clin Psychol. 1988; 56(6):893-7. [DOI:10.1037/0022-006X.56.6.893] [PMID]
- Jahn DR, Leith J, Muralidharan A, Brown CH, Drapalski AL, Hack S, et al. The influence of experiences of stigma on recovery: Mediating roles of internalized stigma, self-esteem, and self-efficacy. Psychiatr Rehabil J. 2020; 43(2):97-105. https://psycnet.apa.org/buy/2019-35069-001
- Karamouzian M, Akbari M, Haghdoost A-A, Setayesh H, Zolala F. “I am dead to them”: HIV-related stigma experienced by people living with HIV in Kerman, Iran. J Assoc Nurses AIDS Care. 2015; 26(1):46-56. [DOI:10.1016/j.jana.2014.04.005] [PMID]
- Rahmati-Najarkolaei F, Niknami S, Aminshokravi F, Bazargan M, Ahmadi F, Hadjizadeh E, et al. Experiences of stigma in healthcare settings among adults living with HIV in the Islamic Republic of Iran. J Int AIDS Soc. 2010; 13:27. [DOI:10.1186/1758-2652-13-27] [PMID] [PMCID]
- Rasoolinajad M, Abedinia N, Noorbala AA, Mohraz M, Badie BM, Hamad A, et al. Relationship among HIV-related stigma, mental health and quality of life for HIV-positive patients in Tehran. AIDS Behav. 2018; 22(12):3773-82. [DOI:10.1007/s10461-017-2023-z] [PMID]
- Grundy G, Beeching N. Understanding social stigma in women with hepatitis C. Nurs Stand. 2004; 19(4):35-9. [DOI:10.7748/ns.19.4.35.s62] [PMID]
- Soltan EM, Salama HM, Aboelmagd MA. Assessment of stigma among patients infected with hepatitis C virus in Suez City, Egypt. J Public Health. 2018; 26(3):279-88. [DOI:10.1007/s10389-017-0872-6]
- Dowsett LE, Coward S, Lorenzetti DL, MacKean G, Clement F. Living with hepatitis C virus: A systematic review and narrative synthesis of qualitative literature. Can J Gastroenterol Hepatol. 2017; 2017:3268650. [DOI:10.1155/2017/3268650] [PMID] [PMCID]
- Turan B, Budhwani H, Fazeli PL, Browning WR, Raper JL, Mugavero MJ, et al. How does stigma affect people living with HIV? The mediating roles of internalized and anticipated HIV stigma in the effects of perceived community stigma on health and psychosocial outcomes. AIDS Behav. 2017; 21(1):283-91. [DOI:10.1007/s10461-016-1451-5] [PMID] [PMCID]
- Enescu A, Mitrut P, Balasoiu M, Turculeanu A, Enescu AS. Psychosocial issues in patients with chronic hepatitis B and C. Curr Health Sci J. 2014; 40(2):93-6. [DOI:10.12865/CHSJ.40.02.02]
- Levi-Minzi MA, Surratt HL. HIV stigma among substance abusing people living with HIV/AIDS: implications for HIV treatment. AIDS Patient Care and STDs. 2014; 28(8):442-51. [DOI:10.1089/apc.2014.0076] [PMID] [PMCID]
- Chan KY, Stoové MA, Sringernyuang L, Reidpath DD. Stigmatization of AIDS patients: disentangling Thai nursing students’ attitudes towards HIV/AIDS, drug use, and commercial sex. AIDS Behav. 2008; 12(1):146-57. [DOI:10.1007/s10461-007-9222-y] [PMID]
- Noor A, Bashir S, Earnshaw VA. Bullying, internalized hepatitis (Hepatitis C virus) stigma, and self-esteem: Does spirituality curtail the relationship in the workplace. J Health Psychol. 2016; 21(9):1860-9. [DOI:10.1177/1359105314567211] [PMID]
- Garvey CM, Jones R. The role of stigma and trauma in hepatitis C virus treatment in veterans: Applying the common-sense model. Public Health Nurs. 2019; 36(6):829-35. [DOI:10.1111/phn.12665] [PMID]
- Krzeczkowska A, Flowers P, Chouliara Z, Hayes P, Dickson A. Experiences of diagnosis, stigma, culpability and disclosure in male patients with hepatitis C virus: An interpretative phenomenological analysis. Health (London). 2021; 25(1):69-85 [DOI:10.1177/1363459319846939] [PMID]
- Brown Johnson CG, Brodsky JL, Cataldo JK. Lung cancer stigma, anxiety, depression, and quality of life. J Psychosoc Oncol. 2014; 32(1):59-73. [DOI:10.1080/07347332.2013.855963] [PMID] [PMCID]
- Chambers SK, Baade P, Youl P, Aitken J, Occhipinti S, Vinod S, et al. Psychological distress and quality of life in lung cancer: the role of health-related stigma, illness appraisals and social constraints. Psychooncology. 2015; 24(11):1569-77. [DOI:10.1002/pon.3829] [PMID] [PMCID]
- Ronel J, Dinkel A, Wolf E, Marten-Mittag B, Mueck B, Mayr C, et al. Anxiety, depression, and health-related quality of life in aging people living with HIV compared to diabetes patients and patients with minor health conditions: A longitudinal study. Psychol Health Med. 2018; 23(7):823-30. [DOI:10.1080/13548506.2018.1437276] [PMID]
- Weeland MM, Nijhof KS, Otten R, Vermaes IPR, Buitelaar JK. Beck’s cognitive theory and the response style theory of depression in adolescents with and without mild to borderline intellectual disability. Res Dev Disabil. 2017; 69:39-48. [DOI:10.1016/j.ridd.2017.07.015] [PMID]
- Henrique-Araujo R, Quarantini LC, Caribe AC, Argolo FC, Jesus-Nunes AP, Morais-de-Jesus M, et al. Quality of life, risk behaviors and depression among carriers of hepatitis C virus and human T-cell lymphotropic virus type 1: A comparative study. Braz J Infect Dis. 2019; 23(4):224-30. [DOI:10.1016/j.bjid.2019.06.013] [PMID]
- Dalky HF, Qandil AM, Natour AS, Janet MC. Quality of life, stigma and burden perception among family caregivers and patients with psychiatric illnesses in Jordan. Community Ment Health J. 2017; 53(3):266-74. [DOI:10.1007/s10597-016-0028-0] [PMID]
- Kim SY, Kim JM, Kim SW, Kang HJ, Lee JY, Bae KY, et al. Perceived stigma and quality of life in patients following recovery from delirium. J Clin Psychiatryy. 2017; 78(7):e744-9. [DOI:10.4088/JCP.16m11076] [PMID]
- Tedrus G, Sterca GS, Pereira RB. Physical activity, stigma, and quality of life in patients with epilepsy. Epilepsy Behav. 2017; 77:96-8. [DOI:10.1016/j.yebeh.2017.07.039] [PMID]
- Golden J, O’Dwyer AM, Conroy RM. Depression and anxiety in patients with hepatitis C: prevalence, detection rates and risk factors. Gen Hosp Psychiatry. 2005; 27(6):431-8. [DOI:10.1016/j.genhosppsych.2005.06.006] [PMID]
- Grønkjær LL, Lauridsen MM. Quality of life and unmet needs in patients with chronic liver disease: A mixed-method systematic review. JHEP Rep. 2021; 3(6):100370. [DOI:10.1016/j.jhepr.2021.100370] [PMID] [PMCID]
- Zickmund S, Ho EY, Masuda M, Ippolito L, LaBrecque DR. “They treated me like a leper”. Stigmatization and the quality of life of patients with hepatitis C. J Gen Intern Med. 2003; 18(10):835-44. [DOI:10.1046/j.1525-1497.2003.20826.x] [PMID] [PMCID]
Article Type: Original Contributions |
Subject:
Public Health
Received: 2021/11/13 | Accepted: 2022/05/20 | Published: 2022/07/1
Received: 2021/11/13 | Accepted: 2022/05/20 | Published: 2022/07/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Contact Information
cjhr Office, Guilan University of Medical Sciences
P.O.Box 93345-41938, Rasht, Iran
Journal Tel: +9813 33335820
Publisher Tel: +9821 453 55 000
Email: cjhr.gums@gmail.com
