

Volume 7, Issue 3 (7-2022)
CJHR 2022, 7(3): 127-136 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sadati C, Namvar H, Nasrolahi B. Metacognitive Beliefs, Emerging Adulthood Identity, and Mediating Role of Mental Health: A Structural Equation Modeling Approach. CJHR 2022; 7 (3) :127-136
URL: http://cjhr.gums.ac.ir/article-1-251-en.html
URL: http://cjhr.gums.ac.ir/article-1-251-en.html



1- Department of Psychology, Science and Research Branch, Islamic Azad University, Tehran, Iran., Department of Psychology, Science and Research Branch, Islamic Azad University, Tehran, Iran.
2- Department of Psychology, Saveh Branch, Islamic Azad University, Saveh, Iran. ,hnamvar@iau-saveh.ac.ir
2- Department of Psychology, Saveh Branch, Islamic Azad University, Saveh, Iran. ,
Full-Text [PDF 652 kb]
(919 Downloads)
| Abstract (HTML) (1844 Views)
Full-Text: (1048 Views)
1. Introduction
Identity refers to a set of attitudes, characteristics, and spirits that distinguish one from others. Identity represents a comprehensive and coherent concept of self that is composed of goals, values, and beliefs to which a person strongly adheres [1]. According to evolutionary psychology, the end of adolescence i.e., around the age of 18 is defined as the beginning of adulthood. This definition does not consider the perception-related psychological concepts and the current cultural and economic developments in modern societies [2]. Arnett [3] presented the theory of emerging adulthood (EA) in the context of developmental-cultural psychology, which focuses on the age range of 18 to 25 years, i.e., from late adolescence to early adulthood. He argues that the signs and emotions of adulthood have completely changed for the youth, as they are dependent on individual and unknown aspects rather than social roles. Socioeconomic changes, increased length of study, increased marriage age, and prolonged waiting time for a stable job not only have caused human evolution and transition to adulthood to become a long and complex process but also have given special characteristics to this developmental period of life [4].
The theory of EA was presented within the identity characteristics as an intermediate developmental stage in five distinct identity dimensions [5]; 1- identity exploration that occurs in late adolescence, early twenties, and mid-twenties. Adolescents are looking for an answer to the fundamental question “Who am I?”, explore the options related to occupation and romantic affairs based on their personality background, surrounding environment, and facilities. 2- Possibilities/optimism: one may face many opportunities based on their potential abilities and try to positively seek information and make decisions about their future life. 3- Instability/negativity: the search for identity, social roles, and values of life may be accompanied by numerous and unstable choices, decisions, and plans for education, occupation, and romantic affairs. 4- Self-focus: Compared to the process of socialization in adolescence, this period is the beginning of individualism; individuals focus more on their thoughts so that they can achieve relative stability about social roles as well as their academic, occupational, and romantic choices and make important decisions in line with their life goals to be known an independent and self-sufficient person. 5- Feeling in-between: Identity discovery, instability, and negativity in this transitional period differentiate adolescence from adulthood. This stage of development is characterized by identity exploration, during which one feels he/she is no longer an adolescent but not yet a complete adult [6, 7].
Identity exploration is a complex process involving metacognitive components [8]. Cognitive awareness, or metacognition, refers to high-level and effective processes in the dynamic interpretation, control, guidance, and evaluation of cognitive processes and products that improve human abilities to regulate cognitive activities through the interaction between knowledge, experiences, and cognitive strategies [9]. This process controls, regulates, and interprets thoughts and information processes and consciously, purposefully, and predictably revise cognitive goals and strategies that enable one to make choices and solve problems [10].
Through its judgmental function, metacognition can reduce psychological disturbances and improve mental health of individuals. Studies have shown that successful identity development in youth is directly related to psychological health, and identity variables can significantly predict mental health [11, 12]. On the other hand, the mental health of young people is highly influenced by the identity exploration processes, social origin of identity, and information processing styles. As a result, the coherence of identity dimensions and the development of a unified whole during EA can lead to the highest level of mental health [13].
In the theoretical model based on metacognitive theory, it is assumed that with the activation of dysfunctional and damaged metacognitive components, worries and experiences full of negative emotions and feelings of uncontrollability take on a pathological aspect, and people develop mental health problems [14]. People in this state are involved in thoughts, physical states, moods and external threats that prevent them from paying attention to new information that may not confirm negative beliefs; As a result, subsequent behaviors are disturbed and cause confusion in the person. Thus, people’s specific strategies are always biased and focus the individual’s attention on negative information. Because mental health is how people view themselves, others, and life, and what strategies they use to evaluate, make decisions, and choices in the face of significant developmental challenges and crises, this situation can lead to a style of negativity and a distorted perception of oneself and the environment [15]. Accordingly, the person uses avoidant identity styles in various ways, such as feeling frustrated and unable to control situations, failing to seize opportunities, and lacking self-esteem, and they lose the chance to achieve a successful identity and become an effective adult in the future [16].
Mental health problems increase during adolescence, even under normal conditions. About 15-20% of adolescents experience a period of depression in this stage of their lives [17]. It has been reported that about 19% of the emerging adolescents have experienced at least one mental disorder [18]. Therefore, it is necessary to identify young people aged 15 to 24 years as a high-risk group to be the target of special interventions [19]. Based on the above-mentioned items, there is a relationship between metacognitive factors and identity mediated by mental health. The literature review indicated that a few studies have dealt with the relationship between these three variables in a structural model. Accordingly, the present study aimed to investigate the relationship of metacognitive beliefs with the dimensions of EA identity mediated by mental health in university students.
2. Materials and Methods
In this descriptive-correlational study, the statistical population comprises all 18-25 years old university students of the public universities of Tehran in 2020-21. The research sample consisted of 178 participants (49 male and 129 female) selected through convenience and quota sampling method. One university was selected from each geographical direction of Tehran for a total of four public universities including; Amirkabir University of Technology, Iran University of Science and Technology; Shahid Beheshti and Sharif University of Technology. For each research variable (A total of 11 research variables), 10 samples and a total of 110 students plus 50 were considered as the sample size (160 students). The research data were collected using four questionnaires as an integrated electronic questionnaire due to the Covid-19 pandemic and the universities closure. The questionnaires were uploaded virtually to the official channel of the target public universities. Students were invited to participate in the research via Telegram and WhatsApp. The students were asked to select and mark an option based on the instructions mentioned in each paragraph of the questionnaire and submit it after completion.
Instruments
Arnett’s Inventory of the Dimensions of Emerging Adulthood (IDEA) designed by Reifman et al. contains 31 items [20]. It consists of six subscales, namely identity exploration, possibilities/optimism, instability/negativity, self-focus, feeling in-between, and other-focus. The responses were rated based on a 4-point Likert scale including; 1 strongly disagree, 2 moderately disagree, 3 moderately agree, and 4 strongly agree. The instruction asked the participants to imagine their five recent years (2 past years, the present year, and 2 coming years) and answer the questions on the basis of their personal characteristics and the level of their agreement. The items are accumulated in a subscale on average for each participant, then, the mean of the groups is calculated. The higher scores for all subscales signify the higher amount of the respective structure. The total score of the inventory was obtained from the accumulation of the scores of all subscales, except for the subscale of other-focus. The subscale of “other-focus” is not a part of the main conceptual framework of EA and it was not added to the total score of the other five subscales. Kiani and Hejazi [21] confirmed the validity and reliability (Cronbach’s alpha=0.80) of the Persian version of IDEA.
Metacognition Questionnaire-30 (MCQ-30) was Developed by Wells and Cartwright-Hatton [22]. The MCQ-30 consists of 30 items in five subscales: cognitive confidence, positive beliefs about worry, cognitive self-consciousness, negative beliefs about the uncontrollability of thoughts and danger, and beliefs about the need to control thoughts. The items are scored based on a 4-point Likert scale from 1: Totally Disagree to 4: Totally Agree. Shirinzadeh Dastgiri [23] reported a Cronbach’s alpha of 0.95 for the questionnaire.
Goldberg’s 12-item General Health Questionnaire (GHQ-12) constituents 12 items, and measure the mental health. Each item is scored from 0 to 3 (0=less than usual, 1=no more than usual, 2=rather more than usual, and 3=much more than usual). GHQ-12 examines a person’s mental state over the past four weeks (one month) include symptoms such as abnormal thoughts and feelings and aspects of observable behavior. The score range of this questionnaire is 0 to 36 [24, 25]. Rahmati Najarkolaei [26] reported a Cronbach’s alpha of 0.85 for the questionnaire.
Statistical analyses
According to the research principles, a model was developed and the model parameters were estimated by the method of partial least squares. Metacognitive beliefs were exogenous variables. Mental health was the mediating variable of the model, which was defined as a latent variable. EA components were introduced as endogenous, dependent, and latent variables. To measure the fit of the research conceptual model, Structural Equation Modeling (SEM) was used, which is a kind of latent variable analysis, which allows sets of multiple regression equations to be tested simultaneously to test the relationships between variables. After specifying the model, an estimation of overall goodness of fit of the model with the observed data was performed. Research data were described through mean and standard deviation. Correlation matrix was reported using Pearson correlation coefficient. Data analysis was conducted in SPSS software, version 22 and SEM was performed using SmartPLS-3 software. The reliability of the variables was evaluated in Composite Reliability (CR), which is a measure of the internal fit of the model, in the SmartPLS-3 software. Convergent validity of latent variables was tested with the Average Variance Extracted (AVE). Convergent validity was defined as AVE greater than or equal to 0.50.
3. Results
A total number of 180 electronic questionnaires were collected. Two incomplete questionnaires were eliminated and the statistical analysis was carried out on 178 questionnaires. The mean age of participants was 72.5% were female. The majority of students (44.9%) were aged between 20 and 22 years old. Among the participants 84.8% were undergraduates, 11.8% were postgraduates, and 3.4% were Ph.D. students. Descriptive statistics of study variables are presented in Table 1.
.jpg)
The reliability of the variables was assessed by composite reliability. The results showed that the minimum and maximum composite reliability values were related to self-focus (0.75) and mental health (0.90), respectively, indicating the acceptable reliability of latent variables. The composite reliability coefficients of all variables were more than 0.70. The convergent validity of latent variables was tested with the Average Variance Extracted (AVE). The lowest AVE (0.52) was related to mental health and instability/negativity and the highest AVE (0.67) belonged to “feeling in-between”. Since the mean AVE was greater than 0.5, the convergent validity of latent variables was confirmed. Also, due to the larger CR values than AVE, there was a convergent validity condition (Table 1).
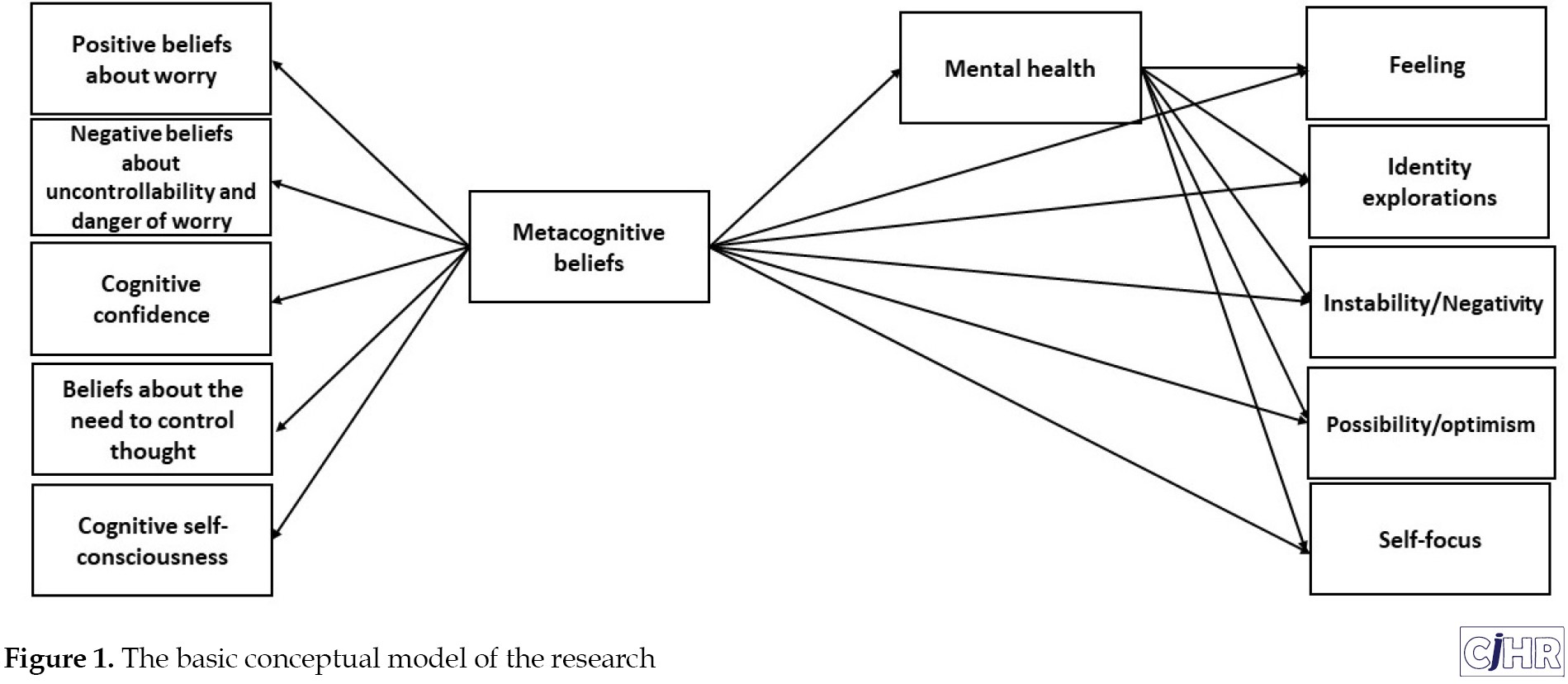
The research model was developed based on theoretical foundations [27]. In this model, “metacognitive beliefs” was the independent variable and its 5 components were regarded as indicators. Defined as a hidden variable, mental health was the mediating variable in this model that was measured with 12 items. The five components of EA were also added to the model as latent variables. “Focus on others” was not added to the model because it was not part of the EA framework. The first step was examining the factor loadings of indicators and eliminating the indicators with a factor loading less than 0.4. Figure 1 shows the basic conceptual model of the research.
 The evaluation of correlations in Table 2 showed that components of metacognitive beliefs had a positive relationship with mental health, a negative relationship with possibilities/optimism, and a positive relationship with the other four components of EA.
The evaluation of correlations in Table 2 showed that components of metacognitive beliefs had a positive relationship with mental health, a negative relationship with possibilities/optimism, and a positive relationship with the other four components of EA.
.jpg)
Mental health also exhibited a negative relationship with possibilities/optimism and a positive relationship with the other four components of EA.
Table 3 provides coefficients of direct effect.
.jpg)
.jpg)
T-values greater than 1.96 indicate the statistical significance of the coefficient. The effect size (f2) was used to determine the effect of each independent variable on the dependent variable. The results demonstrated that metacognitive beliefs significantly and directly affected mental health, and the effect size coefficient revealed a great effect (β=0.61, P=0.001, f2=0.60). Metacognitive beliefs also had a small significant and positive effect on negativity (β=0.24, P=0.010, f2=0.04). Moreover, mental health had a small direct and positive effect on instability/negativity (β=0.25, P=0.004, f2=0.05). Finally, mental health had a small direct and inverse effect on possibilities/optimism (β=-0.23, P=0.018, f2=0.03).
4. Discussion
The present study aimed to investigate the effects of metacognitive beliefs on dimensions of EA identity mediated by mental health in university students in Tehran. Metacognitive beliefs significantly and directly were associated with mental health and significantly and positively affected instability/negativity. Moreover, mental health had a significant and positive effect on instability/negativity and a significant and direct effect on possibilities/optimism. The results demonstrated a significant and indirect effects of metacognitive beliefs on possibilities/optimism and instability/negativity through mental health as mediator. This finding is consistent with the research results of previous study [27].
According to the self-regulatory executive function (S-REF) model, a specific style of limited and inflexible responses to thoughts, emotions, and threats is responsible for the prolonged and exacerbated mental disorders [27, 28]. This specific style is called the Cognitive-Attentional Syndrome (CAS). The S-REF model is responsible for vulnerability to emotional disorders, extreme self-focus attention pattern, irrational beliefs activity, and specific reflective processes. This theory also explains the involvement of cognitive and metacognitive factors in the top-down control of emotional disorders. This model is activated when individuals find inconsistency between their inner goals and external conditions. In other words, the S-REF model aims to minimize this inconsistency. This model employs specific strategies such as absorbing information into beliefs, suppressing thoughts, ruminating, preventing disturbing stimuli from entering consciousness or solving problems caused by incoherence, monitoring physical-mental states, and preparing for dangers to reduce this inconsistency. The S-REF model assumes that individuals with mental health problems are preoccupied with extreme monitoring of relevant information such as thoughts, postures, moods, and external threats. These processes prevent attention to new information that may reject negative beliefs and thus disrupt subsequent behaviors and cause distress [29, 30]. Accordingly, the specific strategies applied by individuals are always biased and bring negative information to their attention, resulting in a distorted perception of themselves and the world.
In this study, metacognitive beliefs had a direct relationship with instability/negativity. Metacognition is the awareness of one’s cognitive processes that often involves conscious efforts to control them [31]. It is also defined as awareness of one’s cognitive status that allows one to manage their performance during any behavior and then choose an appropriate cognitive-emotional regulation strategy [32]. Metacognitive theorists argue that most people experience cognitive and emotional states temporarily because they know how to get rid of and deal with their own ideas and thoughts [33]. According to the metacognitive theory, the maladaptive coping strategies and styles one uses to control cognitions and emotions can trigger maladaptive emotional responses; negative and positive metacognitive beliefs are involved in this process and monitor and control emotional states. This process can also cause a failure to monitor emotional states, cognitive and emotional regulation strategies, and maladaptive coping behaviors, which form part of one’s identity [34]. Therefore, it seems that instability, which arises from the metacognitive coping strategies and styles one may employ in the face of environmental events, not only results in personal failures but also makes one choose negative styles or strategies in dealing with future events.
This study found a direct relationship between metacognitive beliefs and possibilities/optimism. Metacognition is known as the ability to think about oneself in social processing. It is also defined as one’s ability to accurately predict and evaluate issues, situations, and opportunities. Focusing on the thinking style of individuals to explain their inability to effectively cope with the environment and achieve their goals, the metacognitive approach indicates that people’s problems are the result of their inflexible and repetitive thinking styles in response to negative thoughts, feelings, and beliefs. Based on this approach, thought and emotional disorders have roots in metacognition. Within the intimation processing, adaptive metacognitive processes can influence executive operations, performance design, review, inspection, and regulation of behaviors to effectively deal with the environment and seize opportunities. It can hence be concluded that there is a relationship between metacognition and organizing, because knowledge and awareness of cognitive processes should lead to their application through a self-regulation strategy [27]. It seems that metacognitive beliefs reduce one’s ability to think about and evaluate situations and, thus, cause thought disorder and poor self-regulation, as one may miss the opportunities and situations ahead and becomes pessimistic about future situations.
The findings of current study showed mediating role of mental health in the relationship of metacognitive beliefs with possibilities/optimism and instability/negativity. The metacognitive theory, as a tendency to focus attention and monitor the thoughts, has been proposed to explain how disturbing thoughts or doubts trigger metacognitions as well as cognitive and emotional reactions. Based on the metacognitive model, an emotional disorder means the selection of an emotion regulation strategy influenced by one’s metacognitive beliefs about the necessity and consequence of the chosen strategy [33]. However, all of these strategies negatively affect one’s attentional threshold for identifying information that contradicts wrong beliefs. The metacognitive theory plays an important role in beliefs about mental states, including beliefs about emotions and anxiety. Individual differences in metacognition are related to understanding the relationship between perceived stress and negative cognitions and emotions. A fundamental principle of this approach is that beliefs and metacognitive components guide thoughts and coping activities. Positive and negative beliefs about thoughts generally affect how individuals evaluate events and guide their cognition and performance. Those with a high level of cognitive self-awareness constantly pay attention to and control their thoughts as well as their mental functioning [32]. Accordingly, such individuals claim that they can control their emotions. Regardless of one’s efforts to stop metacognitive beliefs, this process leads to the development of annoying cognitions and negative emotion regulation strategies and also the emergence and persistence of negative emotions. Therefore, it seems that the metacognitive beliefs and coping strategies that people select based on their CAS to deal with their surrounding environment cause cognitive and emotional disturbance and reduce the mental health of individuals. As a result, such individuals take a negative and pessimistic identity style in dealing with events, which leads to the loss of opportunities.
The present study used non-probability sampling as well as self-report as a research tool, which can affect the results of the research. it is recommended to use more trustable methods such as interview in future studies. Other limitation of the present study was the small sample size which may induce random error and reduce study power.
5. Conclusion
According to the results, mental health had a mediating role in the relationship between metacognitive beliefs and EA identity in university students. Based on the study findings, it is necessary to pay special attention to metacognitive beliefs as a factor affecting some identity dimensions (e.g., instability/negativity and possibilities/optimism) and mental health as the mediator of the relationship between metacognitive beliefs and these identity dimensions to better understand the relationship between these variables. Considering the results, it is recommended to measure the meta-emotion structure and level of mental health in students. Besides, it is recommended to hold training workshops on metacognitive strategies training to improve their mental health and form identity styles. Finally, it is recommended to provide metacognitive therapies to students meeting the conditions.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethical Committee of Department of Psychology, Science and Research Branch, Islamic Azad University, Tehran, Iran (code: 123960146971).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
This article was extracted from a part of the Ph.D. dissertation of Camelia Sadati in the Department of Psychology, Science and Research Branch, Islamic Azad University, Tehran, Iran. The researchers wish to thank all the individuals who participated in the study.
References
Identity refers to a set of attitudes, characteristics, and spirits that distinguish one from others. Identity represents a comprehensive and coherent concept of self that is composed of goals, values, and beliefs to which a person strongly adheres [1]. According to evolutionary psychology, the end of adolescence i.e., around the age of 18 is defined as the beginning of adulthood. This definition does not consider the perception-related psychological concepts and the current cultural and economic developments in modern societies [2]. Arnett [3] presented the theory of emerging adulthood (EA) in the context of developmental-cultural psychology, which focuses on the age range of 18 to 25 years, i.e., from late adolescence to early adulthood. He argues that the signs and emotions of adulthood have completely changed for the youth, as they are dependent on individual and unknown aspects rather than social roles. Socioeconomic changes, increased length of study, increased marriage age, and prolonged waiting time for a stable job not only have caused human evolution and transition to adulthood to become a long and complex process but also have given special characteristics to this developmental period of life [4].
The theory of EA was presented within the identity characteristics as an intermediate developmental stage in five distinct identity dimensions [5]; 1- identity exploration that occurs in late adolescence, early twenties, and mid-twenties. Adolescents are looking for an answer to the fundamental question “Who am I?”, explore the options related to occupation and romantic affairs based on their personality background, surrounding environment, and facilities. 2- Possibilities/optimism: one may face many opportunities based on their potential abilities and try to positively seek information and make decisions about their future life. 3- Instability/negativity: the search for identity, social roles, and values of life may be accompanied by numerous and unstable choices, decisions, and plans for education, occupation, and romantic affairs. 4- Self-focus: Compared to the process of socialization in adolescence, this period is the beginning of individualism; individuals focus more on their thoughts so that they can achieve relative stability about social roles as well as their academic, occupational, and romantic choices and make important decisions in line with their life goals to be known an independent and self-sufficient person. 5- Feeling in-between: Identity discovery, instability, and negativity in this transitional period differentiate adolescence from adulthood. This stage of development is characterized by identity exploration, during which one feels he/she is no longer an adolescent but not yet a complete adult [6, 7].
Identity exploration is a complex process involving metacognitive components [8]. Cognitive awareness, or metacognition, refers to high-level and effective processes in the dynamic interpretation, control, guidance, and evaluation of cognitive processes and products that improve human abilities to regulate cognitive activities through the interaction between knowledge, experiences, and cognitive strategies [9]. This process controls, regulates, and interprets thoughts and information processes and consciously, purposefully, and predictably revise cognitive goals and strategies that enable one to make choices and solve problems [10].
Through its judgmental function, metacognition can reduce psychological disturbances and improve mental health of individuals. Studies have shown that successful identity development in youth is directly related to psychological health, and identity variables can significantly predict mental health [11, 12]. On the other hand, the mental health of young people is highly influenced by the identity exploration processes, social origin of identity, and information processing styles. As a result, the coherence of identity dimensions and the development of a unified whole during EA can lead to the highest level of mental health [13].
In the theoretical model based on metacognitive theory, it is assumed that with the activation of dysfunctional and damaged metacognitive components, worries and experiences full of negative emotions and feelings of uncontrollability take on a pathological aspect, and people develop mental health problems [14]. People in this state are involved in thoughts, physical states, moods and external threats that prevent them from paying attention to new information that may not confirm negative beliefs; As a result, subsequent behaviors are disturbed and cause confusion in the person. Thus, people’s specific strategies are always biased and focus the individual’s attention on negative information. Because mental health is how people view themselves, others, and life, and what strategies they use to evaluate, make decisions, and choices in the face of significant developmental challenges and crises, this situation can lead to a style of negativity and a distorted perception of oneself and the environment [15]. Accordingly, the person uses avoidant identity styles in various ways, such as feeling frustrated and unable to control situations, failing to seize opportunities, and lacking self-esteem, and they lose the chance to achieve a successful identity and become an effective adult in the future [16].
Mental health problems increase during adolescence, even under normal conditions. About 15-20% of adolescents experience a period of depression in this stage of their lives [17]. It has been reported that about 19% of the emerging adolescents have experienced at least one mental disorder [18]. Therefore, it is necessary to identify young people aged 15 to 24 years as a high-risk group to be the target of special interventions [19]. Based on the above-mentioned items, there is a relationship between metacognitive factors and identity mediated by mental health. The literature review indicated that a few studies have dealt with the relationship between these three variables in a structural model. Accordingly, the present study aimed to investigate the relationship of metacognitive beliefs with the dimensions of EA identity mediated by mental health in university students.
2. Materials and Methods
In this descriptive-correlational study, the statistical population comprises all 18-25 years old university students of the public universities of Tehran in 2020-21. The research sample consisted of 178 participants (49 male and 129 female) selected through convenience and quota sampling method. One university was selected from each geographical direction of Tehran for a total of four public universities including; Amirkabir University of Technology, Iran University of Science and Technology; Shahid Beheshti and Sharif University of Technology. For each research variable (A total of 11 research variables), 10 samples and a total of 110 students plus 50 were considered as the sample size (160 students). The research data were collected using four questionnaires as an integrated electronic questionnaire due to the Covid-19 pandemic and the universities closure. The questionnaires were uploaded virtually to the official channel of the target public universities. Students were invited to participate in the research via Telegram and WhatsApp. The students were asked to select and mark an option based on the instructions mentioned in each paragraph of the questionnaire and submit it after completion.
Instruments
Arnett’s Inventory of the Dimensions of Emerging Adulthood (IDEA) designed by Reifman et al. contains 31 items [20]. It consists of six subscales, namely identity exploration, possibilities/optimism, instability/negativity, self-focus, feeling in-between, and other-focus. The responses were rated based on a 4-point Likert scale including; 1 strongly disagree, 2 moderately disagree, 3 moderately agree, and 4 strongly agree. The instruction asked the participants to imagine their five recent years (2 past years, the present year, and 2 coming years) and answer the questions on the basis of their personal characteristics and the level of their agreement. The items are accumulated in a subscale on average for each participant, then, the mean of the groups is calculated. The higher scores for all subscales signify the higher amount of the respective structure. The total score of the inventory was obtained from the accumulation of the scores of all subscales, except for the subscale of other-focus. The subscale of “other-focus” is not a part of the main conceptual framework of EA and it was not added to the total score of the other five subscales. Kiani and Hejazi [21] confirmed the validity and reliability (Cronbach’s alpha=0.80) of the Persian version of IDEA.
Metacognition Questionnaire-30 (MCQ-30) was Developed by Wells and Cartwright-Hatton [22]. The MCQ-30 consists of 30 items in five subscales: cognitive confidence, positive beliefs about worry, cognitive self-consciousness, negative beliefs about the uncontrollability of thoughts and danger, and beliefs about the need to control thoughts. The items are scored based on a 4-point Likert scale from 1: Totally Disagree to 4: Totally Agree. Shirinzadeh Dastgiri [23] reported a Cronbach’s alpha of 0.95 for the questionnaire.
Goldberg’s 12-item General Health Questionnaire (GHQ-12) constituents 12 items, and measure the mental health. Each item is scored from 0 to 3 (0=less than usual, 1=no more than usual, 2=rather more than usual, and 3=much more than usual). GHQ-12 examines a person’s mental state over the past four weeks (one month) include symptoms such as abnormal thoughts and feelings and aspects of observable behavior. The score range of this questionnaire is 0 to 36 [24, 25]. Rahmati Najarkolaei [26] reported a Cronbach’s alpha of 0.85 for the questionnaire.
Statistical analyses
According to the research principles, a model was developed and the model parameters were estimated by the method of partial least squares. Metacognitive beliefs were exogenous variables. Mental health was the mediating variable of the model, which was defined as a latent variable. EA components were introduced as endogenous, dependent, and latent variables. To measure the fit of the research conceptual model, Structural Equation Modeling (SEM) was used, which is a kind of latent variable analysis, which allows sets of multiple regression equations to be tested simultaneously to test the relationships between variables. After specifying the model, an estimation of overall goodness of fit of the model with the observed data was performed. Research data were described through mean and standard deviation. Correlation matrix was reported using Pearson correlation coefficient. Data analysis was conducted in SPSS software, version 22 and SEM was performed using SmartPLS-3 software. The reliability of the variables was evaluated in Composite Reliability (CR), which is a measure of the internal fit of the model, in the SmartPLS-3 software. Convergent validity of latent variables was tested with the Average Variance Extracted (AVE). Convergent validity was defined as AVE greater than or equal to 0.50.
3. Results
A total number of 180 electronic questionnaires were collected. Two incomplete questionnaires were eliminated and the statistical analysis was carried out on 178 questionnaires. The mean age of participants was 72.5% were female. The majority of students (44.9%) were aged between 20 and 22 years old. Among the participants 84.8% were undergraduates, 11.8% were postgraduates, and 3.4% were Ph.D. students. Descriptive statistics of study variables are presented in Table 1.
The reliability of the variables was assessed by composite reliability. The results showed that the minimum and maximum composite reliability values were related to self-focus (0.75) and mental health (0.90), respectively, indicating the acceptable reliability of latent variables. The composite reliability coefficients of all variables were more than 0.70. The convergent validity of latent variables was tested with the Average Variance Extracted (AVE). The lowest AVE (0.52) was related to mental health and instability/negativity and the highest AVE (0.67) belonged to “feeling in-between”. Since the mean AVE was greater than 0.5, the convergent validity of latent variables was confirmed. Also, due to the larger CR values than AVE, there was a convergent validity condition (Table 1).
The research model was developed based on theoretical foundations [27]. In this model, “metacognitive beliefs” was the independent variable and its 5 components were regarded as indicators. Defined as a hidden variable, mental health was the mediating variable in this model that was measured with 12 items. The five components of EA were also added to the model as latent variables. “Focus on others” was not added to the model because it was not part of the EA framework. The first step was examining the factor loadings of indicators and eliminating the indicators with a factor loading less than 0.4. Figure 1 shows the basic conceptual model of the research.
Mental health also exhibited a negative relationship with possibilities/optimism and a positive relationship with the other four components of EA.
Table 3 provides coefficients of direct effect.
T-values greater than 1.96 indicate the statistical significance of the coefficient. The effect size (f2) was used to determine the effect of each independent variable on the dependent variable. The results demonstrated that metacognitive beliefs significantly and directly affected mental health, and the effect size coefficient revealed a great effect (β=0.61, P=0.001, f2=0.60). Metacognitive beliefs also had a small significant and positive effect on negativity (β=0.24, P=0.010, f2=0.04). Moreover, mental health had a small direct and positive effect on instability/negativity (β=0.25, P=0.004, f2=0.05). Finally, mental health had a small direct and inverse effect on possibilities/optimism (β=-0.23, P=0.018, f2=0.03).
4. Discussion
The present study aimed to investigate the effects of metacognitive beliefs on dimensions of EA identity mediated by mental health in university students in Tehran. Metacognitive beliefs significantly and directly were associated with mental health and significantly and positively affected instability/negativity. Moreover, mental health had a significant and positive effect on instability/negativity and a significant and direct effect on possibilities/optimism. The results demonstrated a significant and indirect effects of metacognitive beliefs on possibilities/optimism and instability/negativity through mental health as mediator. This finding is consistent with the research results of previous study [27].
According to the self-regulatory executive function (S-REF) model, a specific style of limited and inflexible responses to thoughts, emotions, and threats is responsible for the prolonged and exacerbated mental disorders [27, 28]. This specific style is called the Cognitive-Attentional Syndrome (CAS). The S-REF model is responsible for vulnerability to emotional disorders, extreme self-focus attention pattern, irrational beliefs activity, and specific reflective processes. This theory also explains the involvement of cognitive and metacognitive factors in the top-down control of emotional disorders. This model is activated when individuals find inconsistency between their inner goals and external conditions. In other words, the S-REF model aims to minimize this inconsistency. This model employs specific strategies such as absorbing information into beliefs, suppressing thoughts, ruminating, preventing disturbing stimuli from entering consciousness or solving problems caused by incoherence, monitoring physical-mental states, and preparing for dangers to reduce this inconsistency. The S-REF model assumes that individuals with mental health problems are preoccupied with extreme monitoring of relevant information such as thoughts, postures, moods, and external threats. These processes prevent attention to new information that may reject negative beliefs and thus disrupt subsequent behaviors and cause distress [29, 30]. Accordingly, the specific strategies applied by individuals are always biased and bring negative information to their attention, resulting in a distorted perception of themselves and the world.
In this study, metacognitive beliefs had a direct relationship with instability/negativity. Metacognition is the awareness of one’s cognitive processes that often involves conscious efforts to control them [31]. It is also defined as awareness of one’s cognitive status that allows one to manage their performance during any behavior and then choose an appropriate cognitive-emotional regulation strategy [32]. Metacognitive theorists argue that most people experience cognitive and emotional states temporarily because they know how to get rid of and deal with their own ideas and thoughts [33]. According to the metacognitive theory, the maladaptive coping strategies and styles one uses to control cognitions and emotions can trigger maladaptive emotional responses; negative and positive metacognitive beliefs are involved in this process and monitor and control emotional states. This process can also cause a failure to monitor emotional states, cognitive and emotional regulation strategies, and maladaptive coping behaviors, which form part of one’s identity [34]. Therefore, it seems that instability, which arises from the metacognitive coping strategies and styles one may employ in the face of environmental events, not only results in personal failures but also makes one choose negative styles or strategies in dealing with future events.
This study found a direct relationship between metacognitive beliefs and possibilities/optimism. Metacognition is known as the ability to think about oneself in social processing. It is also defined as one’s ability to accurately predict and evaluate issues, situations, and opportunities. Focusing on the thinking style of individuals to explain their inability to effectively cope with the environment and achieve their goals, the metacognitive approach indicates that people’s problems are the result of their inflexible and repetitive thinking styles in response to negative thoughts, feelings, and beliefs. Based on this approach, thought and emotional disorders have roots in metacognition. Within the intimation processing, adaptive metacognitive processes can influence executive operations, performance design, review, inspection, and regulation of behaviors to effectively deal with the environment and seize opportunities. It can hence be concluded that there is a relationship between metacognition and organizing, because knowledge and awareness of cognitive processes should lead to their application through a self-regulation strategy [27]. It seems that metacognitive beliefs reduce one’s ability to think about and evaluate situations and, thus, cause thought disorder and poor self-regulation, as one may miss the opportunities and situations ahead and becomes pessimistic about future situations.
The findings of current study showed mediating role of mental health in the relationship of metacognitive beliefs with possibilities/optimism and instability/negativity. The metacognitive theory, as a tendency to focus attention and monitor the thoughts, has been proposed to explain how disturbing thoughts or doubts trigger metacognitions as well as cognitive and emotional reactions. Based on the metacognitive model, an emotional disorder means the selection of an emotion regulation strategy influenced by one’s metacognitive beliefs about the necessity and consequence of the chosen strategy [33]. However, all of these strategies negatively affect one’s attentional threshold for identifying information that contradicts wrong beliefs. The metacognitive theory plays an important role in beliefs about mental states, including beliefs about emotions and anxiety. Individual differences in metacognition are related to understanding the relationship between perceived stress and negative cognitions and emotions. A fundamental principle of this approach is that beliefs and metacognitive components guide thoughts and coping activities. Positive and negative beliefs about thoughts generally affect how individuals evaluate events and guide their cognition and performance. Those with a high level of cognitive self-awareness constantly pay attention to and control their thoughts as well as their mental functioning [32]. Accordingly, such individuals claim that they can control their emotions. Regardless of one’s efforts to stop metacognitive beliefs, this process leads to the development of annoying cognitions and negative emotion regulation strategies and also the emergence and persistence of negative emotions. Therefore, it seems that the metacognitive beliefs and coping strategies that people select based on their CAS to deal with their surrounding environment cause cognitive and emotional disturbance and reduce the mental health of individuals. As a result, such individuals take a negative and pessimistic identity style in dealing with events, which leads to the loss of opportunities.
The present study used non-probability sampling as well as self-report as a research tool, which can affect the results of the research. it is recommended to use more trustable methods such as interview in future studies. Other limitation of the present study was the small sample size which may induce random error and reduce study power.
5. Conclusion
According to the results, mental health had a mediating role in the relationship between metacognitive beliefs and EA identity in university students. Based on the study findings, it is necessary to pay special attention to metacognitive beliefs as a factor affecting some identity dimensions (e.g., instability/negativity and possibilities/optimism) and mental health as the mediator of the relationship between metacognitive beliefs and these identity dimensions to better understand the relationship between these variables. Considering the results, it is recommended to measure the meta-emotion structure and level of mental health in students. Besides, it is recommended to hold training workshops on metacognitive strategies training to improve their mental health and form identity styles. Finally, it is recommended to provide metacognitive therapies to students meeting the conditions.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethical Committee of Department of Psychology, Science and Research Branch, Islamic Azad University, Tehran, Iran (code: 123960146971).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
This article was extracted from a part of the Ph.D. dissertation of Camelia Sadati in the Department of Psychology, Science and Research Branch, Islamic Azad University, Tehran, Iran. The researchers wish to thank all the individuals who participated in the study.
References
- Berkman ET, Livingston JL, Kahn LE. Finding the “self” in self-regulation: The identity-value model. Psychol Inq. 2017; 28(2-3):77-98. [DOI:10.1080/1047840X.2017.1323463] [PMID] [PMCID]
- Sawyer SM, Azzopardi PS, Wickremarathne D, Patton GC. The age of adolescence. Lancet Child Adolesc Health. 2018; 2(3):223-8. [DOI:10.1016/S2352-4642(18)30022-1]
- Arnett JJ. Suffering, selfish, slackers? Myths and reality about emerging adults. J Youth Adolesc. 2007; 36:23-9. [DOI:10.1007/s10964-006-9157-z]
- Wood D. Emerging adulthood as a critical stage in the life Course. In: Halfon N, Forrest C, Lerner R, Faustman E, editors. Handbook of life course health development. Cham: Springer; 2018. https://books.google.com/books?id=pZQVuAEACAAJ&printsec=frontcover&dq=editions:ISBN3319471414
- Arnett JJ. Emerging adulthood: The winding road from the late teens through the twenties. 2th ed. New York: Oxford University Press; 2015. [DOI:10.1093/oxfordhb/9780199795574.013.9]
- Ryan RM, Deci EL. Self-determination theory: Basic psychological needs in motivation, development, and wellness. New York: Guilford Publications; 2017. [DOI:10.1521/978.14625/28806]
- Beyers W, Luyckx K. Ruminative exploration and reconsideration of commitment as risk factors for suboptimal identity development in adolescence and emerging adulthood. J Adolesc. 2016; 47:169-78. [DOI:10.1016/j.adolescence.2015.10.018] [PMID]
- Amini F, Ramezani K, Maredpour A. Effectiveness of mindfulness group training on hope and resilience of people with gender dysphoria. Caspian J Health Res. 2022; 7(1):35-42. [DOI:10.32598/CJHR.7.1.395.1]
- Jia X, Li W, Cao L. The role of metacognitive components in creative thinking. Front Psychol. 2019; 10:2404. [DOI:10.3389/fpsyg.2019.02404] [PMID] [PMCID]
- Teng MF, Qin C, Wang C. Validation of metacognitive academic writing strategies and the predictive effects on academic writing performance in a foreign language context. Metacogn Learn. 2022; 17(1):167-90. [DOI:10.1007/s11409-021-09278-4] [PMID] [PMCID]
- Bonfils KA, Luther L, George S, Buck KD, Lysaker PH. The role of metacognitive self-reflectivity in emotional awareness and subjective indices of recovery in schizophrenia. J Nerv Ment Dis. 2016; 204(12):903-8. [DOI:10.1097/NMD.0000000000000599] [PMID] [PMCID]
- Gonzales-Backen MA, Dumka LE, Millsap RE, Yoo HC, Schwartz SJ, Zamboanga BL, et al. The role of social and personal identities in self-esteem among ethnic minority college students. Identity (Mahwah, N J). 2015; 15(3):202-20. [DOI:10.1080/15283488.2015.1055532] [PMID] [PMCID]
- Schwartz SJ, Hardy SA, Zamboanga BL, Meca A, Waterman AS, Picariello S, et al. Identity in young adulthood: Links with mental health and risky behavior. J Appl Dev Psychol. 2015; 36:39-52. [DOI:10.1016/j.appdev.2014.10.001] [PMID] [PMCID]
- Ellis DM, Hudson JL. The metacognitive model of generalized anxiety disorder in children and adolescents. Clin Child Fam Psychol Rev. 2010; 13(2):151-63. [DOI:10.1007/s10567-010-0065-0] [PMID]
- Nair B, Otaki F. Promoting university students’ mental health: A systematic literature review introducing the 4m-model of individual-level interventions. Front Public Health. 2021; 9:699030. [DOI:10.3389/fpubh.2021.699030] [PMID] [PMCID]
- Jung E, Pick O, Schlüter-Müller S, Schmeck K, Goth K. Identity development in adolescents with mental problems. Child Adolesc Psychiatry Ment Health. 2013; 7(1):26. [DOI:10.1186/1753-2000-7-26] [PMID] [PMCID]
- Ariyazangane E, Borna M R, Joharifard R. Relation of anger rumination and self-criticism with social maladjustment with the mediating role of psychological flexibility in adolescent boys and girls. Caspian J Health Res. 2022; 7(1):5-14. [DOI:10.32598/CJHR.7.1.381.1]
- Gomes AP, Soares ALG, Kieling C, Rohde LA, Gonçalves H. Mental disorders and suicide risk in emerging adulthood: the 1993 Pelotas birth cohort. Rev Saude Publica. 2019; 53:96. [DOI:10.11606/s1518-8787.20190530012356] [PMID] [PMCID]
- Hochberg ZE, Konner M. Emerging adulthood, a pre-adult life-history stage. Front Endocrinol (Lausanne). 2020; 10:918. [DOI:10.3389/fendo.2019.00918] [PMID] [PMCID]
- Reifman A, Arnett JJ, Colwell MJ. Emerging adulthood: Theory, assessment and application. J Youth Dev. 2007. 2007; 2(1):12. [DOI:10.5195/jyd.2007.359]
- Kiani M, Hejazi E. [The concept of the transition to adulthood among Iranian emerging adults: A cultural and social perspective (Persian)]. Cult Psychol. 2017; 1(1):25-51. https://www.sid.ir/en/Journal/ViewPaper.aspx?ID=684348
- Wells A, Cartwright-Hatton S. A short form of the metacognitions questionnaire: Properties of the MCQ-30. Behav Res Ther. 2004; 42(4):385-96. [DOI:10.1016/S0005-7967(03)00147-5]
- Shirinzadeh Dastgiri S, Goudarzi MA, Rahimi Changiz, Naziri GH. [Study of factor structure, validity and reliability of metacognition questionnaire-30 (Persian)]. J Psychol. 2009; 12(1):445-61. https://www.sid.ir/en/Journal/ViewPaper.aspx?ID=152935
- Hystad SW, Johnsen BH. The dimensionality of the 12-item General Health Questionnaire (GHQ-12): Comparisons of factor structures and invariance across samples and time. Front Psychol. 2020; 11:1300. [DOI:10.3389/fpsyg.2020.01300] [PMID] [PMCID]
- Montazeri A, Harirchi AM, Shariati M, Garmaroudi G, Ebadi M, Fateh A. The 12-item General Health Questionnaire (GHQ-12): Translation and validation study of the Iranian version. Health Qual Life Outcomes. 2003; 1(1):66. [DOI:10.1186/1477-7525-1-19]
- Rahmati Najarkolaei F, Raiisi F, Rahnama P, Gholami Fesharaki M, Zamani O, Jafari MR, et al. Factor structure of the Iranian version of 12-item general health questionnaire. Iran Red Crescent Med J. 2014; 16(9):e11794. [DOI:10.5812/ircmj.11794] [PMID] [PMCID]
- Capobianco L, Faija C, Husain Z, Wells A. Metacognitive beliefs and their relationship with anxiety and depression in physical illnesses: A systematic review. PLoS One. 2020; 15(9):e0238457. [DOI:10.1371/journal.pone.0238457] [PMID] [PMCID]
- Reinholdt-Dunne ML, Blicher A, Nordahl H, Normann N, Esbjørn BH, Wells A. Modeling the relationships between metacognitive beliefs, attention control and symptoms in children with and without anxiety disorders: A test of the S-REF model. Front Psychol. 2019; 10:1205. [DOI:10.3389/fpsyg.2019.01205] [PMID] [PMCID]
- Gutierrez R, Hirani T, Curtis L, Ludlow AK. Metacognitive beliefs mediate the relationship between anxiety sensitivity and traits of obsessive-compulsive symptoms. BMC Psychol. 2020; 8(1):1-7. [DOI: 10.1186/s40359-020-00412-6] [PMID: 32336292] [PMCID: PMC7184693]
- Bright M, Parker S, French P, Fowler D, Gumley A, Morrison AP, et al. Metacognitive beliefs as psychological predictors of social functioning: An investigation with young people at risk of psychosis. Psychiatry Res. 2018; 262:520-6. [DOI:10.1016/j.psychres.2017.09.037] [PMID] [PMCID]
- Yuki S, Nakatani H, Nakai T, Okanoya K, Tachibana RO. Regulation of action selection based on metacognition in humans via a ventral and dorsal medial prefrontal cortical network. Cortex. 2019; 119:336-49. [DOI:10.1016/j.cortex.2019.05.001] [PMID]
- Kukla M, Lysaker PH. Metacognition over time is related to neurocognition, social cognition, and intrapsychic foundations in psychosis. Schizophr Res Cogn. 2020; 19:100149. [DOI:10.1016/j.scog.2019.100149] [PMID] [PMCID]
- Rochat L, Manolov R, Billieux J. Efficacy of metacognitive therapy in improving mental health: A meta-analysis of single-case studies. J Clin Psychol. 2018; 74(6):896-915. [DOI:10.1002/jclp.22567] [PMID]
- Johnson SU, Hoffart A. Metacognitive therapy versus cognitive behavioral therapy: A network approach. Front Psychol. 2018; 9:2382. [DOI:10.3389/fpsyg.2018.02382] [PMID] [PMCID]
Article Type: Original Contributions |
Subject:
Health Education and Promotion
Received: 2022/01/9 | Accepted: 2022/04/15 | Published: 2022/07/1
Received: 2022/01/9 | Accepted: 2022/04/15 | Published: 2022/07/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
