

Volume 8, Issue 1 (1-2023)
CJHR 2023, 8(1): 45-52 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Zhalegholi S, Kasmaei P, Bakhshi F, Fattahi E, Jadgal M S, Mehrabian F et al . The application of Protection Motivation Theory in predicting AIDS prevention behaviors in drug addicts living in addiction treatment camps. CJHR 2023; 8 (1) :45-52
URL: http://cjhr.gums.ac.ir/article-1-284-en.html
URL: http://cjhr.gums.ac.ir/article-1-284-en.html
Sadegh Zhalegholi1 

 , Parisa Kasmaei * 2, Fataneh Bakhshi3 , Esmaeil Fattahi1 , Mohammad Saeed Jadgal4 , Fardin Mehrabian5 , Nooshin Rouhani-Tonekaboni5
, Parisa Kasmaei * 2, Fataneh Bakhshi3 , Esmaeil Fattahi1 , Mohammad Saeed Jadgal4 , Fardin Mehrabian5 , Nooshin Rouhani-Tonekaboni5
, Parisa Kasmaei * 2, Fataneh Bakhshi3 , Esmaeil Fattahi1 , Mohammad Saeed Jadgal4 , Fardin Mehrabian5 , Nooshin Rouhani-Tonekaboni5
1- Department of Health Education and Promotion, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
2- Research Center of Health and Environment, Department of Health Education and Promotion, School of Health, Guilan University of Medical Sciences, Rasht, Iran. , kasmayparisa@yahoo.com
3- Social Determinants of Health Research Center, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
4- Department of Public Health, School of Nursing, Iranshahr University of Medical Sciences, Chabahar, Iran.
5- Research Center of Health and Environment, Department of Health Education and Promotion, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
2- Research Center of Health and Environment, Department of Health Education and Promotion, School of Health, Guilan University of Medical Sciences, Rasht, Iran. , kasmayparisa@yahoo.com
3- Social Determinants of Health Research Center, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
4- Department of Public Health, School of Nursing, Iranshahr University of Medical Sciences, Chabahar, Iran.
5- Research Center of Health and Environment, Department of Health Education and Promotion, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
Full-Text [PDF 534 kb]
(226 Downloads)
| Abstract (HTML) (710 Views)
References
Full-Text: (174 Views)
1. Introduction
Acquired immunodeficiency syndrome (AIDS) is caused by infection with the human immunodeficiency virus (HIV), and the spectrum of the disease can range from a mild blood infection to severe immunodeficiency with life-threatening opportunistic infections and AIDS-related malignancies [1]. According to the report of the World Health Organization (WHO), by the end of 2021, the rate of HIV infection in Iran will rise to 53,000 people, and Iran is known as one of the most dangerous countries in the world in terms of HIV infection [2]. More than 90% of new cases of AIDS have been reported in developing countries (including Iran) [3]. The final goal of the AIDS care system by WHO is to control the AIDS epidemic by 2030. In order to achieve this goal, all countries of the world have committed to follow the 90-90-90 comprehensive strategy by the end of 2020. In this context, it was expected that about 90% of the infected people in the world would be identified, 90% of the identified cases would be treated with antiretroviral treatment, and the virus level of 90% of those receiving antiretroviral treatment would decrease significantly. According to this goal, by the end of 2019 in Iran, 37% of infected people have been identified and of these, 67% have received antiviral treatment and about 85% have had viral load suppression [4].
Addiction, as one of the most important ways of AIDS and other blood borne viral disease, has been increasing all over the world for various reasons during the last few decades [5, 6, 7]. Approximately 10% of HIV infections worldwide are among people who inject drugs [8]. Unemployment, poor economic situation, feeling of loneliness, homelessness, emotional and psychological pressures, and easy access are among the factors of a person’s tendency to abuse drugs [9]. According to an estimate by United Nation, about 1.3 million people in Iran have a serious problem of drug abuse [10].
In the absence of vaccine and treatment, the only way to control AIDS is health education to change risky behaviors [5]. To describe the factors affecting behavior, experts have presented a range of different theories and models [7]. Protection-Motivation Theory (PMT) is among health education models which focuses on cognitive factors affecting decision-making in the face of traumatic events. The PMT was developed by Rogers in 1975 to explain the effects of fear on health attitudes and behaviors. In this theory, adoption of protective behavior is directly influenced by the individual’s motivation for self-protection and environmental and personal factors combine as a potential health threat. This threat begins with two cognitive processes, including threat assessment and coping assessment. Threat appraisal examines maladaptive behaviors and factors affecting the likelihood of engaging in potentially unhealthy behaviors, which include intrinsic and extrinsic rewards of unhealthy behavior i.e. benefits of unhealthy behaviors, perceived vulnerability i.e. a person’s belief in vulnerability to health threats, and perceived severity i.e. a person’s belief in the seriousness of the health threat. Coping assessment assesses the ability to cope with and repel the threatened danger which includes perceived self-efficacy i.e. a person’s belief in the ability to successfully perform the proposed behavior, perceived response efficacy i.e. a person’s estimate of the effectiveness of the proposed behavior, and perceived response costs i.e. a person’s estimate of the costs and obstacles of performing protective behavior [11]. In order to create the intention to protect against the threat in the person, perceived severity and perceived Vulnerability should outweigh the rewards of the maladaptive response, and perceived response self-efficacy and efficacy should overcome the costs of the maladaptive response [12].
Considering that based on the searches by the authors, no similar study has been conducted in Iran regarding addiction and AIDS in addiction treatment camps using the PMT, this study was aimed to determine the predictive factors of AIDS prevention behaviors based on the PMT in drug addicts living in addiction treatment camps in city of Rasht, North of Iran.
2. Materials and Methods
Study type and population
The current research was a descriptive cross-sectional study in which the predictive factors of AIDS-preventive behaviors based on the PMT were investigated. The research community included drug addicts living in addiction treatment camps in city of Rasht. According to the prevention deputy of welfare organization, there was 20 camps with an average of 20 residents in each camp in Rasht. In this study one camp dedicated for women was excluded. The sample size was calculated based on the rule of thumb of 5 observations per 59 items of the questionnaire. Considering 10% attrition rate, a total of 320 sample was estimated. The sample were selected by a simple random sampling method using random numbers tables from the list of residents of 19 camps.
Measures and data collection
The data collection tool was a questionnaire consisting of 3 parts; the first part included demographic characteristics, the second part included the items of the PMT constructs (47 items) and the third part included the items of the preventive behaviors (12 items). Demographic characteristics included the variables of age, gender, level of education, employment status, marital status, place of residence, suffering from various diseases, having relatives or friends suffering from AIDS, and the way of drug use. All items of PMT constructs were scored on a 5-point Likert scale. The construct of perceived Vulnerability had 4 items and a higher score indicated a greater sense of vulnerability in drug-dependent patients to AIDS. The construct of perceived Severity also had 4 items and a higher score denoted a high degree of risk of contracting AIDS by drug dependent patients. The response efficiency construct had 6 questions with a higher score indicating the more confidence of drug-dependent patients for the effectiveness of preventive behavior in reducing the risk of health threats. The self-efficacy construct had 6 items with higher score indicating more confidence of drug dependent patients in their ability to perform preventive behavior against AIDS. The higher score of response cost construct with 7 items indicated the understanding of more obstacles for drug-dependent patients to perform preventive behavior against AIDS. The reward construct had 9 items and its higher score denoted receiving more rewards for not performing the preventive behavior. The higher scores of fear and protection motivation constructs with 3 and 8 items indicated the high f worry of the drug dependent patients of contracting AIDS and its complications and higher intention of drug dependent patients in performing preventive behavior against AIDS, respectively. Preventive behaviors included 12 items and its higher score indicated more preventive behaviors against AIDS in drug dependent patients.
To determine the validity of the questionnaire, it was given to 7 faculty members of medical sciences universities and according to their opinions, the content validity ratio (CVR) and content validity index (CVI) were calculated. Also, in order to determine the reliability, Cronbach’s alpha was calculated by 18 drug addicts apart from the studied population. Table 1 shows the number of items, reliability, and validity measure of constructs of PMT and AIDS prevention behaviors.
.jpg)
Statistical analysis
Data were described using Mean±SD or frequency and percent. Normalized mean was calculated to get the same range of values between 0 and 1. The normality of the continuous data was checked using the skewness index. Values greater than 1.96 or less than -1.96 were considered as violation from normal distribution. Due to the normality of the data, parametric tests including independent t-test and analysis of variance were used to compare the mean score of preventive behaviors according to demographic variables. The correlation between knowledge and different constructs of the model was estimated using Pearson correlation coefficient. To determine the adjusted relationship between knowledge and each of the constructs of PMT with the behavioral intention score, multivariate linear regression model was used. A significance level of less than 0.05 was considered. All statistical analysis was performed using SPSS software version 22.
3. Results
The present study was conducted on 320 patients. The demographic characteristics of the study participants are detailed in Table 2.
.jpg)
.jpg)
The mean age of the study participants was 34.0±9.11 years old. In terms of gender, all 320 people (100%) were men. 136 people (42.5%) had secondary education. Table 3 depicts descriptive statistics of PMT construct and prevention behaviors against AIDS.
.jpg)
According to the percent of normalized mean, the score of all constructs were higher than mean except for knowledge. The mean percent of knowledge score was 42.6%.
The correlation matrix of constructs of PMT and HIV prevention behaviors is shown in Table 4.
.jpg)
There was weak significant direct correlation between preventive behaviors with perceived self-efficacy (r=0.20), knowledge (r=0.16), reward (r=0.15), response cost (r=0.14), response efficiency (r=0.13), and fear (r=0.11).
In this study two dependent variables i.e. preventive behaviors and protection motivation were explored using separate multivariate linear regression models. Table 5 shows the final model with a backward approach in predicting the protection motivation construct based on the knowledge variable and the constructs of the PMT.
.jpg)
The perceived self-efficacy construct based on the standardized coefficient (0.33) is the most important predictive variable in the model.The model accounted for 38% of variance of dependent variable.
Table 6 shows the final model with a backward approach in predicting HIV prevention behaviors based on the knowledge and PMT constructs.
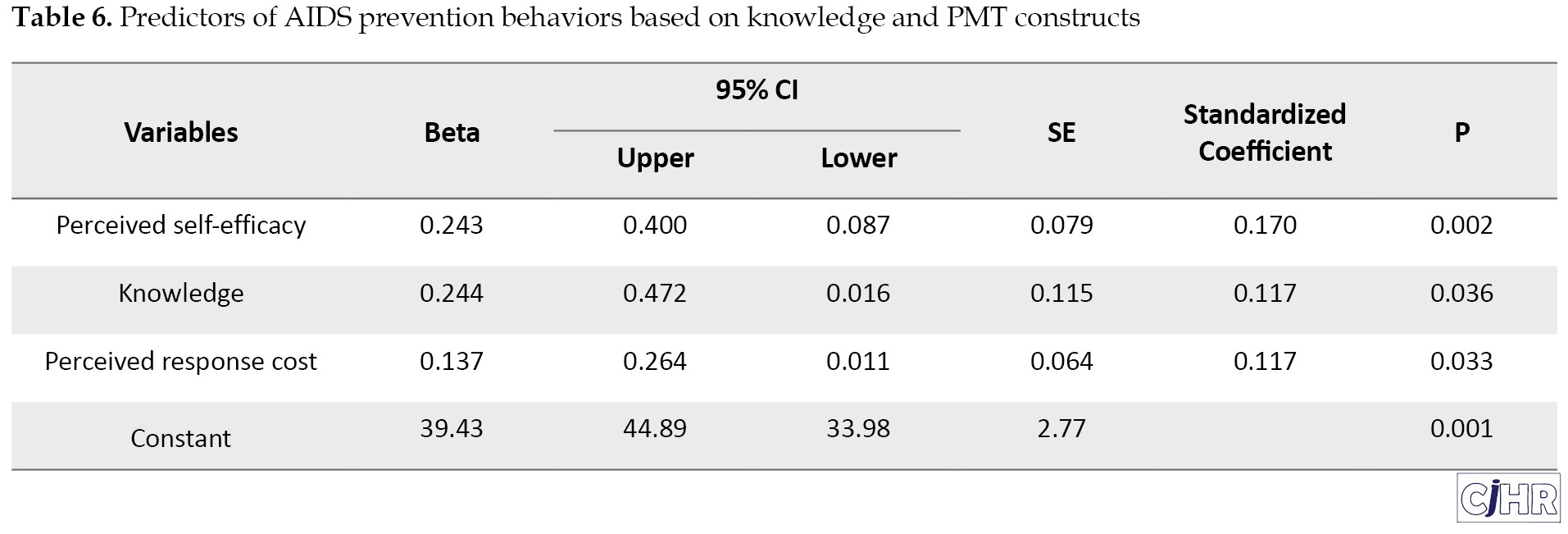
The perceived self-efficacy construct based on the standardized coefficient of 0.17 is the most important predictive variable in the model. the model explained 7% of variation of the prevention behaviors against AIDS.
4. Discussion
The results of this study revealed that PMT model could appropriately predict protection motivation but it was a poor predictor for prevention behaviors against AIDS. Among PMT constructs, perceived self-efficacy was the strongest predictors for protection motivation, followed by perceived response-efficacy. In agree with the result of this study, self-efficacy was the most important predictor for intention to providing dental care to HIV/AIDS patients [13], sexual behaviors in students [14], and exercise of control over AIDS infection [15]. In the study by Azadeh et al. [16] the self-efficacy construct was effective in the willingness of employees to protect themselves from illness. In the results of many other studies, self-efficacy has been introduced as the most important precondition for behavior change and the strongest predictor of protection motivation [17].
Perceived self-efficacy has an abstract aspect and does not relate to one’s ability, but rather one’s judgment of one’s ability to successfully perform a behavior. Perception abilities and competence in a specific domain motivate people to perform behaviors in which they excel. The feeling of efficacious and skilled in person performance may encourage one to engage more in the target behavior [18]. The people who have a higher level of self-efficacy, have greater sense of control and have higher goals and committed, and so their behavior becomes more favorable [19].
It is expected that the effectiveness of the suggested preventive behavior will increase the response [20]. The findings of this study confirm previous studies that response efficacy of public health actions may increase levels of acceptance of personal preventive behaviors [21, 22, 23, 24, 25].
In current study, the PMT model was not a suitable predictor of AIDS preventive behaviors. In contrast, the PMT model was reported to be a useful framework for some of health-related behaviors such as predicting Rabies protective behaviors among school students [26].There are many reasons that prohibit the desired change in behavior despite of having high motivation. Lack of intention is one of the obstacles that is not evaluate in PMT model. It is suggested that future research consider a wide range of psychosocial barriers that may play a role in adopting the desired preventive behaviors against AIDS.
Also, based on the findings of this study, a significant difference was observed between the groups according to the history of AIDS. Drug addicts with a history of AIDS disease in their relatives and acquaintances showed significantly more preventive behaviors than those who did not have AIDS patients in their relatives and acquaintances which states, that group of drug-dependent patients who have AIDS patients in their relatives and acquaintances take more preventive behaviors due to increased Vulnerability and perceived severity. In the study of Khodavisi et al., there was no significant relationship between the history of addiction and hepatitis B in the family and the adoption of hepatitis B prevention behaviors.
5. Conclusion
In the present study, according to the data of the linear regression model, drug dependent patients showed a high motivation to adopt AIDS preventive behaviors, but it seems that due to the low intention of this group, this high motivation does not reach the stage of protective behavior. Therefore, it is recommended to conduct more studies in the future in the field of existing obstacles to convert protection motivation into behavior.
Ethical Considerations
Compliance with ethical guidelines
Ethical consideration: the study protocol has been approved by Guilan University of Medical Science (Code: IR.GUMS.REC.1400.481.
Funding
This article is part of the thesis of the master’s degree in health education and health promotion of the first author and was conducted with the financial support of the Research Vice-chancellor of Guilan University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
The authors consider it necessary to acknowledge and thank the efforts of university research experts and people participating in the study.
Acquired immunodeficiency syndrome (AIDS) is caused by infection with the human immunodeficiency virus (HIV), and the spectrum of the disease can range from a mild blood infection to severe immunodeficiency with life-threatening opportunistic infections and AIDS-related malignancies [1]. According to the report of the World Health Organization (WHO), by the end of 2021, the rate of HIV infection in Iran will rise to 53,000 people, and Iran is known as one of the most dangerous countries in the world in terms of HIV infection [2]. More than 90% of new cases of AIDS have been reported in developing countries (including Iran) [3]. The final goal of the AIDS care system by WHO is to control the AIDS epidemic by 2030. In order to achieve this goal, all countries of the world have committed to follow the 90-90-90 comprehensive strategy by the end of 2020. In this context, it was expected that about 90% of the infected people in the world would be identified, 90% of the identified cases would be treated with antiretroviral treatment, and the virus level of 90% of those receiving antiretroviral treatment would decrease significantly. According to this goal, by the end of 2019 in Iran, 37% of infected people have been identified and of these, 67% have received antiviral treatment and about 85% have had viral load suppression [4].
Addiction, as one of the most important ways of AIDS and other blood borne viral disease, has been increasing all over the world for various reasons during the last few decades [5, 6, 7]. Approximately 10% of HIV infections worldwide are among people who inject drugs [8]. Unemployment, poor economic situation, feeling of loneliness, homelessness, emotional and psychological pressures, and easy access are among the factors of a person’s tendency to abuse drugs [9]. According to an estimate by United Nation, about 1.3 million people in Iran have a serious problem of drug abuse [10].
In the absence of vaccine and treatment, the only way to control AIDS is health education to change risky behaviors [5]. To describe the factors affecting behavior, experts have presented a range of different theories and models [7]. Protection-Motivation Theory (PMT) is among health education models which focuses on cognitive factors affecting decision-making in the face of traumatic events. The PMT was developed by Rogers in 1975 to explain the effects of fear on health attitudes and behaviors. In this theory, adoption of protective behavior is directly influenced by the individual’s motivation for self-protection and environmental and personal factors combine as a potential health threat. This threat begins with two cognitive processes, including threat assessment and coping assessment. Threat appraisal examines maladaptive behaviors and factors affecting the likelihood of engaging in potentially unhealthy behaviors, which include intrinsic and extrinsic rewards of unhealthy behavior i.e. benefits of unhealthy behaviors, perceived vulnerability i.e. a person’s belief in vulnerability to health threats, and perceived severity i.e. a person’s belief in the seriousness of the health threat. Coping assessment assesses the ability to cope with and repel the threatened danger which includes perceived self-efficacy i.e. a person’s belief in the ability to successfully perform the proposed behavior, perceived response efficacy i.e. a person’s estimate of the effectiveness of the proposed behavior, and perceived response costs i.e. a person’s estimate of the costs and obstacles of performing protective behavior [11]. In order to create the intention to protect against the threat in the person, perceived severity and perceived Vulnerability should outweigh the rewards of the maladaptive response, and perceived response self-efficacy and efficacy should overcome the costs of the maladaptive response [12].
Considering that based on the searches by the authors, no similar study has been conducted in Iran regarding addiction and AIDS in addiction treatment camps using the PMT, this study was aimed to determine the predictive factors of AIDS prevention behaviors based on the PMT in drug addicts living in addiction treatment camps in city of Rasht, North of Iran.
2. Materials and Methods
Study type and population
The current research was a descriptive cross-sectional study in which the predictive factors of AIDS-preventive behaviors based on the PMT were investigated. The research community included drug addicts living in addiction treatment camps in city of Rasht. According to the prevention deputy of welfare organization, there was 20 camps with an average of 20 residents in each camp in Rasht. In this study one camp dedicated for women was excluded. The sample size was calculated based on the rule of thumb of 5 observations per 59 items of the questionnaire. Considering 10% attrition rate, a total of 320 sample was estimated. The sample were selected by a simple random sampling method using random numbers tables from the list of residents of 19 camps.
Measures and data collection
The data collection tool was a questionnaire consisting of 3 parts; the first part included demographic characteristics, the second part included the items of the PMT constructs (47 items) and the third part included the items of the preventive behaviors (12 items). Demographic characteristics included the variables of age, gender, level of education, employment status, marital status, place of residence, suffering from various diseases, having relatives or friends suffering from AIDS, and the way of drug use. All items of PMT constructs were scored on a 5-point Likert scale. The construct of perceived Vulnerability had 4 items and a higher score indicated a greater sense of vulnerability in drug-dependent patients to AIDS. The construct of perceived Severity also had 4 items and a higher score denoted a high degree of risk of contracting AIDS by drug dependent patients. The response efficiency construct had 6 questions with a higher score indicating the more confidence of drug-dependent patients for the effectiveness of preventive behavior in reducing the risk of health threats. The self-efficacy construct had 6 items with higher score indicating more confidence of drug dependent patients in their ability to perform preventive behavior against AIDS. The higher score of response cost construct with 7 items indicated the understanding of more obstacles for drug-dependent patients to perform preventive behavior against AIDS. The reward construct had 9 items and its higher score denoted receiving more rewards for not performing the preventive behavior. The higher scores of fear and protection motivation constructs with 3 and 8 items indicated the high f worry of the drug dependent patients of contracting AIDS and its complications and higher intention of drug dependent patients in performing preventive behavior against AIDS, respectively. Preventive behaviors included 12 items and its higher score indicated more preventive behaviors against AIDS in drug dependent patients.
To determine the validity of the questionnaire, it was given to 7 faculty members of medical sciences universities and according to their opinions, the content validity ratio (CVR) and content validity index (CVI) were calculated. Also, in order to determine the reliability, Cronbach’s alpha was calculated by 18 drug addicts apart from the studied population. Table 1 shows the number of items, reliability, and validity measure of constructs of PMT and AIDS prevention behaviors.
Statistical analysis
Data were described using Mean±SD or frequency and percent. Normalized mean was calculated to get the same range of values between 0 and 1. The normality of the continuous data was checked using the skewness index. Values greater than 1.96 or less than -1.96 were considered as violation from normal distribution. Due to the normality of the data, parametric tests including independent t-test and analysis of variance were used to compare the mean score of preventive behaviors according to demographic variables. The correlation between knowledge and different constructs of the model was estimated using Pearson correlation coefficient. To determine the adjusted relationship between knowledge and each of the constructs of PMT with the behavioral intention score, multivariate linear regression model was used. A significance level of less than 0.05 was considered. All statistical analysis was performed using SPSS software version 22.
3. Results
The present study was conducted on 320 patients. The demographic characteristics of the study participants are detailed in Table 2.
The mean age of the study participants was 34.0±9.11 years old. In terms of gender, all 320 people (100%) were men. 136 people (42.5%) had secondary education. Table 3 depicts descriptive statistics of PMT construct and prevention behaviors against AIDS.
According to the percent of normalized mean, the score of all constructs were higher than mean except for knowledge. The mean percent of knowledge score was 42.6%.
The correlation matrix of constructs of PMT and HIV prevention behaviors is shown in Table 4.
There was weak significant direct correlation between preventive behaviors with perceived self-efficacy (r=0.20), knowledge (r=0.16), reward (r=0.15), response cost (r=0.14), response efficiency (r=0.13), and fear (r=0.11).
In this study two dependent variables i.e. preventive behaviors and protection motivation were explored using separate multivariate linear regression models. Table 5 shows the final model with a backward approach in predicting the protection motivation construct based on the knowledge variable and the constructs of the PMT.
The perceived self-efficacy construct based on the standardized coefficient (0.33) is the most important predictive variable in the model.The model accounted for 38% of variance of dependent variable.
Table 6 shows the final model with a backward approach in predicting HIV prevention behaviors based on the knowledge and PMT constructs.
The perceived self-efficacy construct based on the standardized coefficient of 0.17 is the most important predictive variable in the model. the model explained 7% of variation of the prevention behaviors against AIDS.
4. Discussion
The results of this study revealed that PMT model could appropriately predict protection motivation but it was a poor predictor for prevention behaviors against AIDS. Among PMT constructs, perceived self-efficacy was the strongest predictors for protection motivation, followed by perceived response-efficacy. In agree with the result of this study, self-efficacy was the most important predictor for intention to providing dental care to HIV/AIDS patients [13], sexual behaviors in students [14], and exercise of control over AIDS infection [15]. In the study by Azadeh et al. [16] the self-efficacy construct was effective in the willingness of employees to protect themselves from illness. In the results of many other studies, self-efficacy has been introduced as the most important precondition for behavior change and the strongest predictor of protection motivation [17].
Perceived self-efficacy has an abstract aspect and does not relate to one’s ability, but rather one’s judgment of one’s ability to successfully perform a behavior. Perception abilities and competence in a specific domain motivate people to perform behaviors in which they excel. The feeling of efficacious and skilled in person performance may encourage one to engage more in the target behavior [18]. The people who have a higher level of self-efficacy, have greater sense of control and have higher goals and committed, and so their behavior becomes more favorable [19].
It is expected that the effectiveness of the suggested preventive behavior will increase the response [20]. The findings of this study confirm previous studies that response efficacy of public health actions may increase levels of acceptance of personal preventive behaviors [21, 22, 23, 24, 25].
In current study, the PMT model was not a suitable predictor of AIDS preventive behaviors. In contrast, the PMT model was reported to be a useful framework for some of health-related behaviors such as predicting Rabies protective behaviors among school students [26].There are many reasons that prohibit the desired change in behavior despite of having high motivation. Lack of intention is one of the obstacles that is not evaluate in PMT model. It is suggested that future research consider a wide range of psychosocial barriers that may play a role in adopting the desired preventive behaviors against AIDS.
Also, based on the findings of this study, a significant difference was observed between the groups according to the history of AIDS. Drug addicts with a history of AIDS disease in their relatives and acquaintances showed significantly more preventive behaviors than those who did not have AIDS patients in their relatives and acquaintances which states, that group of drug-dependent patients who have AIDS patients in their relatives and acquaintances take more preventive behaviors due to increased Vulnerability and perceived severity. In the study of Khodavisi et al., there was no significant relationship between the history of addiction and hepatitis B in the family and the adoption of hepatitis B prevention behaviors.
5. Conclusion
In the present study, according to the data of the linear regression model, drug dependent patients showed a high motivation to adopt AIDS preventive behaviors, but it seems that due to the low intention of this group, this high motivation does not reach the stage of protective behavior. Therefore, it is recommended to conduct more studies in the future in the field of existing obstacles to convert protection motivation into behavior.
Ethical Considerations
Compliance with ethical guidelines
Ethical consideration: the study protocol has been approved by Guilan University of Medical Science (Code: IR.GUMS.REC.1400.481.
Funding
This article is part of the thesis of the master’s degree in health education and health promotion of the first author and was conducted with the financial support of the Research Vice-chancellor of Guilan University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
The authors consider it necessary to acknowledge and thank the efforts of university research experts and people participating in the study.
References
- Fauci S, Folkers GK, Lane HC. Human immunodeficiency virus disease: AIDS and related disorders. In: Kasper DL, Nivatpumin PJ, Brown CD, Hemnes AR, editors. Harrison’s principles of internal medicine. New York: McGrow Hill; 2001. [Link]
- Jadgal KM, Alizadeh Siuki H, Shamaian Razavi N. The using of health belief model on AIDS preventive behaviors among health volunteers. J Res Health. 2015; 5(1):58-64. [Link]
- Movahed E, Morowatisharifabad MA, Farokhzadian J, Nikooie R, Hosseinzadeh M, Askarishahi M, et al. Antiretroviral therapy adherence among people living with HIV: Directed content analysis based on information-motivation-beh avioral skills model. Int Q Community Health Educ. 2019; 40(1):47-56. [DOI:10.1177/0272684X19858029] [PMID]
- Nyamathi A, Ekstrand M, Heylen E, Ramakrishna P, Yadav K, Sinha S, et al. Relationships among adherence and physical and mental health among women living with HIV in rural India. AIDS Behav. 2018; 22:867-76. [DOI:10.1007/s10461-016-1631-3] [PMID] [PMCID]
- Nabipour S, Ayu Said M, Hussain Habil M. Burden and nutritional deficiencies in opiate addiction-systematic review article. Iran J Public Health. 2014; 43(8):1022-32. [Link]
- Bakhshi F, Nezamdust F, Leili EK. The relationship between social capital and mental health in individuals living with HIV in North of Iran. HIV AIDS Rev. Int J HIV Relat Probl. 2021; 20(1):33-8. [DOI:10.5114/hivar.2021.105110]
- Kazmi SA, Rauf A, Alshahrani MM, Awadh AAA, Iqbal Z, Soltane R, et al. Hepatitis B among university population: Prevalence, associated risk factors, knowledge assessment, and treatment management. Viruses. 2022; 14(9):1936. [DOI:10.3390/v14091936] [PMID] [PMCID]
- World Health Organisation (WHO). Report on the global AIDS epidemic. Geneva: World Health Organisation; 2022. [Link]
- Valadbaigi E, Nickbakht A, lashkari A. [Tendency to drug use among high school students (case study: Marivan high schools) (Persian)]. Soc Welfare. 2017; 17(64):237-59. [Link]
- Joint United Nations Programme on HIV/AIDS (UNAIDS). 90-90-90-an ambitious treatment target to help end the AIDS epidemic [Internet]. 2017 [Updated 2023 January 16] Available from: [Link]
- Jadgal MS, Vahedian-Shahroodi M, Lale-Monfared E, Tehrani H, Gholian-Aval M, et al. The study of domestic accidents prevention behaviors based on protection motivation theory among mothers with children less than 6 years covered by health centers in Torbat- Heydariyeh City (Persian)]. J Saf Promot Inj Prev. 2019; 7(3):159-65. [Link]
- Keshavarz P, Tahmasebi R, Noroozi A. [Predictor factors for household accident prevention behavior based on protection-motivation theory in children under 5 years (Persian)]. J Hayat. 2020; 25 (4):444-57. [Link]
- Ebadifard-Azar F, Dehdari T, Laka S, Dehdari L, Khanipour A. [Determinants of intention of dentists for providing dental care to HIV/AIDS-infected patients based on protection motivation theory (Persian)]. Iran J Health Educ Health Promot. 2015; 2(4):281-10. [Link]
- Kasen S, Vaughan RD, Walter HJ. Self-efficacy for AIDS preventive behaviors among tenth grade students. Health Educ Q. 1992; 19(2):187-202. [DOI:10.1177/109019819201900204] [PMID]
- Bandura A. Perceived self-efficacy in the exercise of control over AIDS infection. Eval Program Plann. 1990; 13(1):9-17. [DOI:10.1016/0149-7189(90)90004-G]
- Azadeh M, Ramezani T, Taheri-Kharameh Z. [Factors affecting workplace protective behaviors against covid-19 disease in employees of crowded public offices: Application of protection motivation theory (Persian)]. Iran Occup Health. 2020; 17(Special Issue Covid-19):1-11. [Link]
- Matlabi M, Esmaeili R, Mohammadzadeh F, Hassanpour-Nejad H. [The effect of educational intervention based on the protection motivation theory in promotion of preventive behaviors against covid-19 (Persian)]. Health Syst Res. 2022; 18(1)30-8. [DOI:10.48305/jhsr.v18i1.1445]
- Pender NJ, Murdaugh CL, Parsons MA. Health promotion in nursing practice. Hoboken: Prentice Hall; 2006. [Link]
- Kelishadi R, Ardalan G, Gheyratmand R, Sheikholeslam R, Majdzadeh SR, Delavari AR, et al. [Can the dietary habits of our society provide future health of children and adolescents? (Persian)]. Caspian study. Iran J Pediatr. 2005; 15:97-109. [Link]
- Norman P, Boer H, Seydel ER. Protection motivation theory. In: Conner M, Norman P, editors. Predicting health behaviour: Research and practice with social cognition models. Maidenhead: Open University Press; 2005. [Link]
- Yu Y, Fai Lau JT, Chun Lau MM. Competing or interactive effect between perceived response efficacy of governmental social distancing behaviors and personal freedom on social distancing behaviors in the Chinese adult general population in Hong Kong. Int J Health Policy Manag. 2022; 11(4):498-507. [DOI:10.34172/ijhpm.2020.195]
- de Zwart O, Veldhuijzen IK, Richardus JH, Brug J. Monitoring of risk perceptions and correlates of precautionary behaviour related to human avian influenza during 2006-2007 in the Netherlands: Results of seven consecutive surveys. BMC Infect Dis. 2010; 10:114. [DOI:10.1186/1471-2334-10-114] [PMID] [PMCID]
- Lau JT, Griffiths S, Choi KC, Lin C. Prevalence of preventive behaviors and associated factors during early phase of the H1N1 influenza epidemic. Am J Infect Control. 2010; 38 (5):374-80. [DOI:10.1016/j.ajic.2010.03.002] [PMID] [PMCID]
- Lau JT, Kim JH, Tsui H, Griffiths S. Perceptions related to human avian influenza and their associations with anticipated psychological and behavioral responses at the onset of outbreak in the Hong Kong Chinese general population. Am J Infect Control. 2007; 35(1):38-49. [DOI:10.1016/j.ajic.2006.07.010] [PMID] [PMCID]
- Bults M, Beaujean DJ, de Zwart O, Kok G, van Empelen P, van Steenbergen JE, et al. Perceived risk, anxiety, and behavioural responses of the general public during the early phase of the influenza A (H1N1) pandemic in the Netherlands: Results of three consecutive online surveys. BMC Public Health. 2011; 11:2. [DOI:10.1186/1471-2458-11-2] [PMID] [PMCID]
- Laorujisawat M, Wattanaburanon A, Abdullakasim P, Maharachpong N. Protection motivation theory and rabies protective behaviors among school students in Chonburi Province, Thailand. J Prev Med Public Health. 2021; 54(6):431-40. [DOI:10.3961/jpmph.21.457] [PMID] [PMCID]
Article Type: Original Contributions |
Subject:
Health Education and Promotion
Received: 2022/09/12 | Accepted: 2022/12/20 | Published: 2023/01/1
Received: 2022/09/12 | Accepted: 2022/12/20 | Published: 2023/01/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Contact Information
cjhr Office, Guilan University of Medical Sciences
P.O.Box 93345-41938, Rasht, Iran
Journal Tel: +9813 33335820
Publisher Tel: +9821 453 55 000
Email: cjhr.gums@gmail.com
