

Volume 9, Issue 1 (1-2024)
CJHR 2024, 9(1): 9-20 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Razmjooei F, Gholizadeh M, Barati hokmabadi T, Pashapour Badr M, Javidi M. Theory of Mind, Emotion Recognition and Social Cognition in Adolescents with Generalized Anxiety Disorder and Healthy Controls. CJHR 2024; 9 (1) :9-20
URL: http://cjhr.gums.ac.ir/article-1-337-en.html
URL: http://cjhr.gums.ac.ir/article-1-337-en.html
Foruzan Razmjooei1 

 , Mahdieh Gholizadeh2 , Tookktam Barati hokmabadi3 , Mehrangiz Pashapour Badr4 , Masumeh Javidi * 5
, Mahdieh Gholizadeh2 , Tookktam Barati hokmabadi3 , Mehrangiz Pashapour Badr4 , Masumeh Javidi * 5
, Mahdieh Gholizadeh2 , Tookktam Barati hokmabadi3 , Mehrangiz Pashapour Badr4 , Masumeh Javidi * 5
1- 1. Department of Psychology, Western Tehran Branch, Payame Noor University, Tehran, Iran.
2- Department of psychology, Allameh Tabataba'i University, Tehran, lran
3- Department of psychology, Sabzevar Branch, Islamic Azad University, Sabzevar,lran
4- Department of Psychology, East Azerbaijan Branch, Payame Noor University, Azerbaijan, Iran
5- Department of Cognitive sciences, Cognitive psychology, Western Tehran Branch, Payame Noor University, Tehran, Iran , Masumehjavidi98@gmail.com
2- Department of psychology, Allameh Tabataba'i University, Tehran, lran
3- Department of psychology, Sabzevar Branch, Islamic Azad University, Sabzevar,lran
4- Department of Psychology, East Azerbaijan Branch, Payame Noor University, Azerbaijan, Iran
5- Department of Cognitive sciences, Cognitive psychology, Western Tehran Branch, Payame Noor University, Tehran, Iran , Masumehjavidi98@gmail.com
Full-Text [PDF 546 kb]
(125 Downloads)
| Abstract (HTML) (227 Views)
Full-Text: (65 Views)
Introduction
Generalized anxiety disorder (GAD) is a chronic uncontrollable excessive anxiety towards a variety of topics. It is one of the most prevalent anxiety disorders, affecting approximately 6% worldwide [1]. The prevalence of GAD, which typically begins in young adulthood, is about 2% in the adult population; the lifetime prevalence of GAD is around 4.7% [2]. The disorder is commonly accompanied by other anxiety disorders and depression, and its incidence rate in Iran is 10% overall and 5.2% within a year [3]. The occurrence of anxiety disorders may be linked to a concept known as May’s theory of mind (ToM) [4, 5, 6, 7, 8, 9, 10]. The concept of a theory of mind entails comprehending the thoughts and emotions of another individual through their behaviors [11]. Theory of mind involves the capability to comprehend and discuss the thoughts, wants, and pretend play of individuals. Having an awareness of your own thoughts and recognizing that others might possess divergent beliefs, wishes, and intentions [12].
People with GAD are more likely to underestimate or overestimate their affect and hostile behavior toward others [13]. For example, Zainal & Newman (2018), demonstrated that GAD status significantly interacted with state anxiety to predict the accuracy of global reasoning, cognitive reasoning, positive reasoning, and negative reasoning. Anxiety, as opposed to relaxation, causes people with GAD to display more accurate overall reasoning and cognitive ToM than controls, especially for negative cues. Participants with anxious but not relaxed GAD also interpreted negative cues significantly better than the norms. These results remained after controlling for gender, executive function, social anxiety, and depressive symptoms [14]. Moreover, Baez et al. (2023), in a meta-analysis including studies assessing ToM in patients diagnosed with GAD or social anxiety disorder) SAD (showed significant differences between groups, with lower scores in patients than healthy controls [15]. In addition, a number of authors performed meta-regression analyses to explore the relationship of relevant variables with ToM performance in GAD and SAD patients. Results showed that ToM performance was not significantly dependent on age, sex, years of education, or severity of anxiety [16, 17, 18, 19].
Emotions are a prerequisite for understanding the social environment and adopting competitive social behaviors. These are emotions that form a necessary part of social relationships, and people learn through facial expressions without actually talking about the situation and the wishes, concerns, desires, and intentions of the other party [15]. Aydin et al. (2019), demonstrated that dysfunctional metacognitive beliefs and disrupted emotion recognition in GAD patients compared to healthy controls. Furthermore, poor emotion recognition predicted GAD [20]. Additionally, a meta-analysis, including studies assessing emotion recognition ability in patients diagnosed with GAD or SAD, found that patients showed poorer functioning than healthy people. It is worth mentioning that, despite the significant results, only two studies comparing SAD patients and healthy controls showed significantly lower performance in the patients’ overall scores [21, 22]. Another meta-analysis showed that emotion recognition abilities were not significantly influenced by age, sex, years of education, or severity of anxiety [23]. In addition, many authors’ detailed literature searches to identify studies on explicit emotion recognition in patients with anxiety disorders and major depression compared to healthy participants showed differences in emotion recognition impairment between patients and controls with corresponding confidence intervals computed for each study [24, 25]. According to studies, adults with anxiety disorders have a significantly impaired ability to recognize emotions. In children with anxiety disorders, no significant impairment in emotion recognition was observed [26].
Another variable associated with general anxiety is social cognition [27-32]. Social cognition can be defined as the mental activities that underlie social interactions. This includes mental state attribution, emotion recognition, attributional style, and social cognition. There is also evidence that social cognitive impairments precede the onset of psychosis [29]. Social cognition involves various psychological processes that allow individuals to benefit from their membership in a social group [30]. Social cognitive impairment may be associated with poor functional outcomes, symptoms, and disability in social anxiety disorder (SAD) and GAD [31]. Therefore, deficits in social cognition may partly explain functional decline and poorer quality of life in people with anxiety disorders [32]. Pearcey et al. (2021) demonstrated that increased social anxiety is associated with lower social-cognitive abilities. Moderation analyses revealed specific associations in studies examining social anxiety in participants with and without ASD over 7 years of age and in studies assessing the relationship between anxiety social and specific aspects of the theory of mind (ToM). No significant association was identified between social anxiety and emotion recognition [22]. According to some authors’ assessments. They concluded that in both groups, total scores on all measures of social cognition were related to each other and that there were significant positive correlations between social cognition and age as well as between cognition social and IQ [29].
The studies mentioned have given different results, so unfortunately, there are still gaps in our knowledge about whether the theory of mind, recognizing emotions, and social cognition are involved in generalized anxiety disorder. Furthermore, there has been no simultaneous research on the study of the theory of mind, emotion recognition, and social cognition in teenagers with GAD or without it. However, not much is known about the relationships among these dimensions of social behavior. This study is one of the first in this field and is, in fact, innovative in this sense. Therefore, the purpose of this study was to compare the theory of mind, emotion recognition, and social cognition in adolescents with and without generalized anxiety disorder.
Materials and Methods
Study type and population
This clinic-based case-control study was conducted among teenagers refereed to psychological centers in Tehran, in 2022-23. A total of 120 sample in two groups of 60 teenagers with GAD (as cases) and 60 sex-matched teenagers without GAD (as controls) were compared. The sample size was calculated based on previous results with an effect size of 0.95, considering a power of 95% and type I error of 0.05 [33].
Participants were enrolled into the study if they pass the following inclusion/exclusion criteria: Pre-screening procedures were used to ensure that participants with GAD had been previously diagnosed with GAD by a licensed clinical psychologist or medical doctor based on DSM-IV_TR criteria, the participants consisted of 15-18 teenagers paired with a parent; no suicidal attempts during the past 6 months. Exclusion criteria were history or current psychiatric or neurological disorder or lack of consent from the participant or their legal guardian.; Lack of consent to complete questionnaires, and incomplete questionnaires. After receiving permission from the responsible department of Payame Noor University and the respective principals, the researcher first prepared the list of six psychological centers in the district 7, and then purposefully selected sample members from among the files of people with generalized anxiety disorder in psychological centers based on the inclusion and exclusion criteria. In this study, healthy controls were selected as convenience sampling method. The control group included teenagers who had referred to the study centers for reasons other than generalized anxiety disorder, and were matched to the experimental group in terms of age and sex. Written informed consent for participation and publication was obtained from each participant or legal guardian, respectively.
Study procedure
Following with the coordination of the officials of the psychological centers, the target families and teenagers were contacted by phone to go to the psychological center of Karane located in the 7th region to complete the questionnaires. The researcher first interviewed all the teenagers and after explaining the objectives of the research. The researcher employed multiple methods to collect data, including self-report questionnaires completed by participants (the TOM & social cognition questionnaires), oral recordings conducted by the researcher, and interviews (Ekman 60-faces test [EK-60F]). The time of conducting the interviews and completing the questionnaires was about 120 hours and the researcher carried out the research in 36 days within two months. Data has been gathered from 60 participants diagnosed with GAD and from 60 normal control participants.
Measures
Theory of mind scale (TOM): The TOM questionnaire was created by Steerneman et al. in 1999 to assess the theory of mind in normal children, adolescents (Simon & Saunders), and those with widespread disorders, which has proven its validity as evidence [34]. This questionnaire provides information about a person’s social understanding, sensitivity, and insight, as well as the degree to which one can accept the feelings and thoughts of others. The main form of the scale includes 78 questions in 3 subtests. Subtests include Introduction to Theory of Mind (29 questions), Basic Statement of a True Theory of Mind (33 questions), and Advanced Aspects of Theory of Mind (16 questions) question). This scale was conducted as an interview, correct answers receive 1 point, and incorrect answers receive 0 points. The range of people’s scores on the subscales was 0 to 29 (first subset), 0 to 33 (second subset), and 0 to 16 (third subset). The total score of the instrument ranges from 38 to 190, and a higher score indicates a more favorable theory of mind. The researchers reported the scale’s reliability coefficient to be 0.72 the test’s concurrent validity to be 0.89 and its content validity to be 0.96 [34]. In Iran, the internal homogeneity of the test was calculated using Cronbach’s α coefficient of 0.86 [35]. In current study, the author found that the Cronbach’s α coefficient of this scale is 0.871.
Social cognition questionnaire: This questionnaire was created by Nejati, et al. with the aim of investigating the state of social cognition on students and teenagers [36]. The questionnaire has 19 items that are measured in a 5-point Likert scale. The scoring method of the questionnaire is such that the option includes almost never (1), rarely (2), sometimes (3), often (4) and almost always (5). This questionnaire has 4 subscales of reading the teacher’s mind, detecting educational threats, self-awareness, and understanding the educational environment. The total social cognition score (range 19-95) is calculated as the sum of the subscale scores. Cronbach’s α was also used to check the reliability of the scale, and the coefficient was 0.66 for self-awareness, 0.70 for reading the teacher’s mind, 0.55 for understanding the educational environment, and finally 0.72 for detecting educational threats [37]. In this research, the researcher found the Cronbach’s α coefficient of this scale to be 0.77.
Ekman 60-faces test (EK-60F): Paul Ekman & Wallace. Friesen created the Ekman 60 faces (1986) with the purpose of measuring emotion recognition ability [38]. This test is commonly used for research on mental and neurological disorders, including neurological diseases. Subjects were administered the EK-60F after a pre-test of basic semantic emotion recognition and were asked to verbally provide an example for each of the six emotions (e.g. “tell me that you feel happy” and “I feel happy” when I receive a gift). Any incorrect response resulted in exclusion from the current study. The EK-60F test comprises 60 weighted face images depicting the faces of 10 actors (6 females, 4 male), each expressing six basic emotions (i.e. happy, sad, angry, fear, surprise, disgust). Subjects were asked to respond verbally and choose the label that best described the facial expression the actor was displaying. According to the method of Ekman and Friesen, each image was displayed for 5 seconds [39]. The total test score is from 0 to 60, where a score of 60 represents the best possible performance and each basic sensation has a sub-score of up to 10 points. The reliability of the test in Iran was checked using Cronbach’s α method and the researchers reported a value of 0.79 for the reliability of this scale [40]. In this study, the author found that the Cronbach’s α coefficient of this scale was 0.81.
Statistical analysis
Data were described in terms of Mean±SD or frequency and percent. One-way analysis of variance and post hoc test were used to compare continues variables among four groups of male and female with and without GAD. All analysis was performed using SPSS software, version 27. P<0.05 was considered as significant.
Results
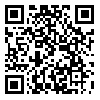
In this sex-matched case control study, 120 teenagers (30 females with generalized anxiety disorder, 30 females without generalized anxiety disorder, 30 males with generalized anxiety disorder, and 30 males without generalized anxiety disorder) from 6 psychological center were participated. The majority of the participants fell within the age range of 15 to 16 years (60.8%) and anxiety) and were in the field of humanities (45%) (Table 1).
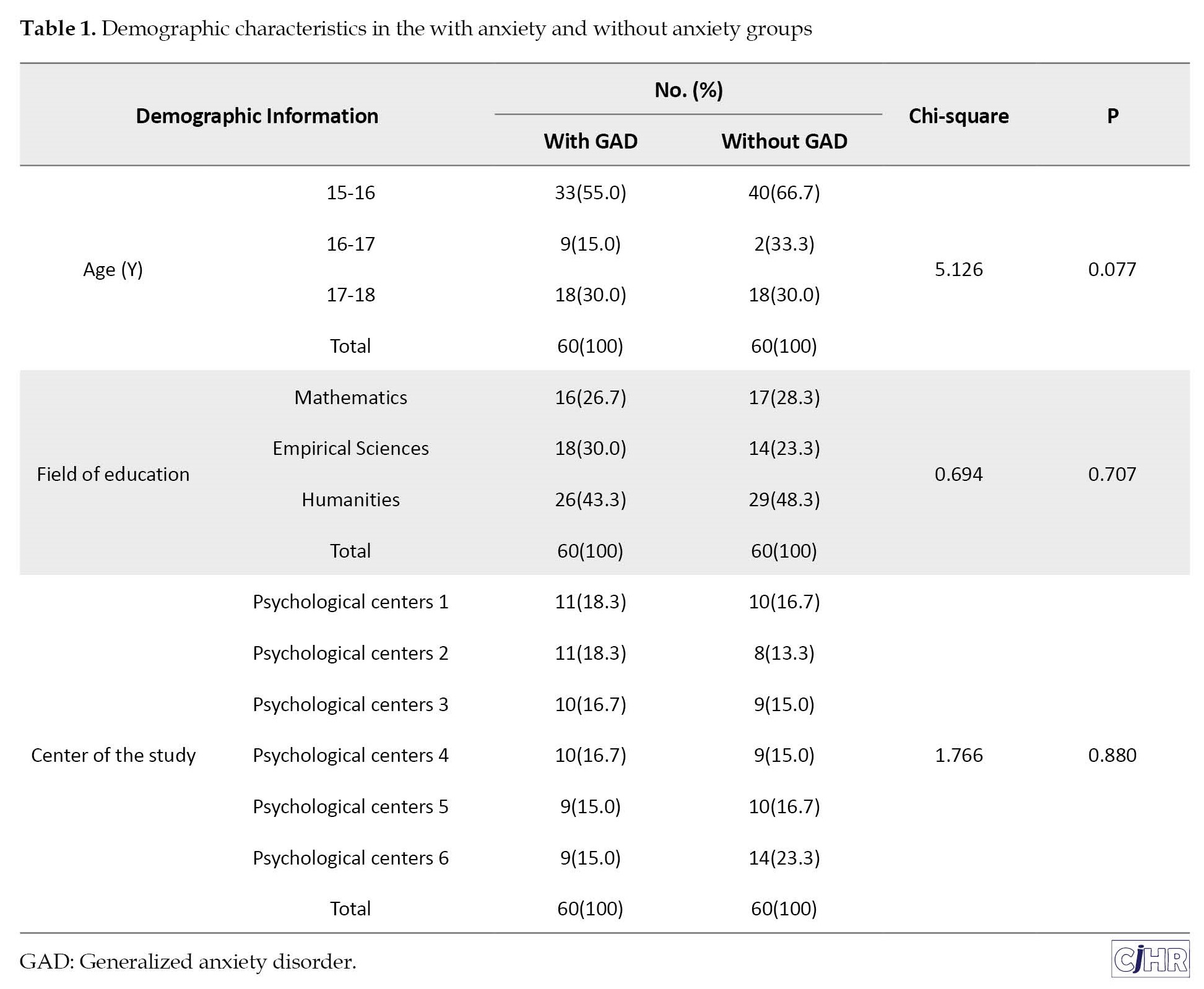
According to Table 2, the mean scores of research variables in the group without GAD in both males and females were higher than the group without GAD.
Similarly, the mean value of all research variables in the females were higher than correspondent males in both groups.
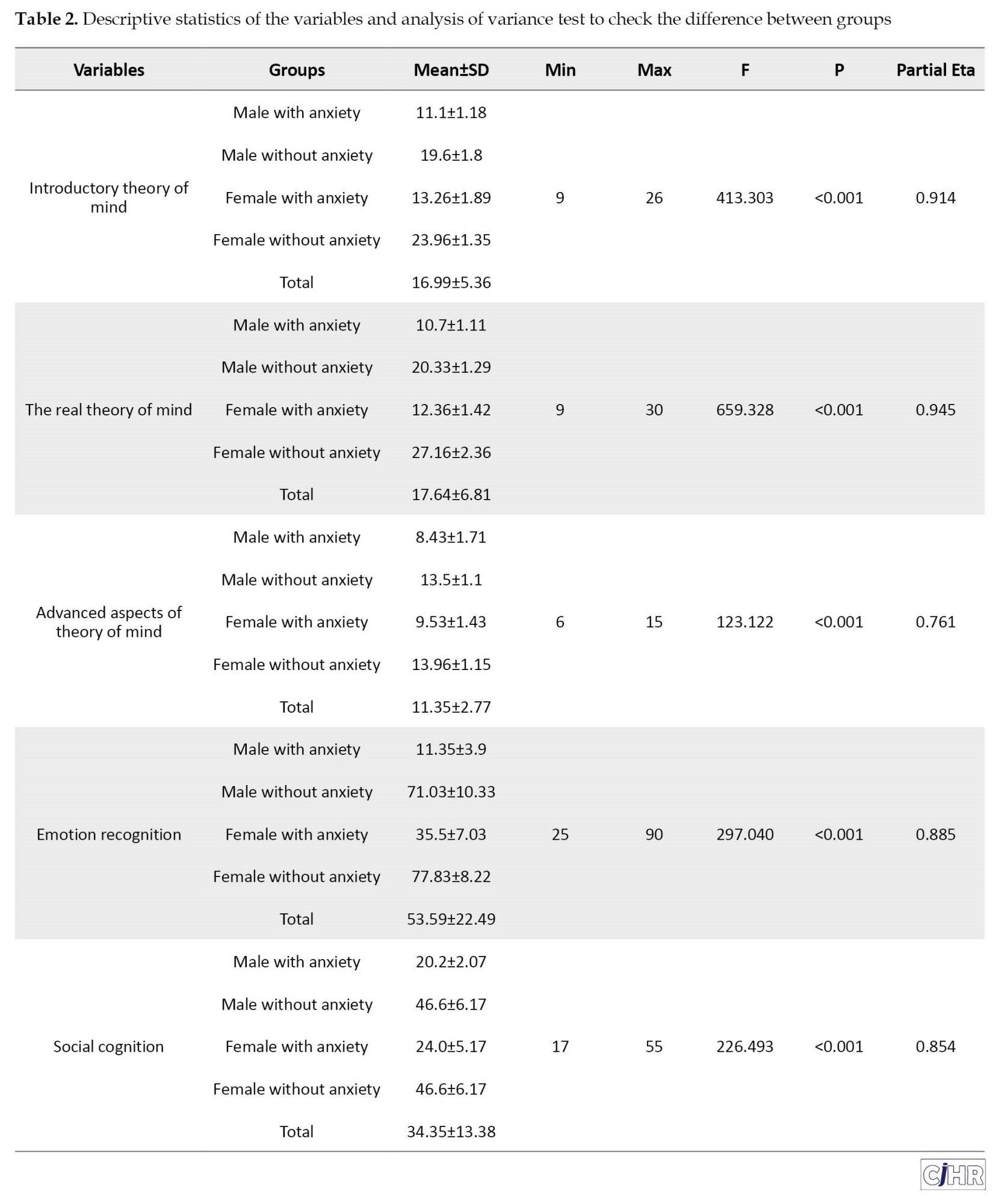
Table 3 demonstrates paired wise comparison of study variables according to sex and group of study using Tuckey’s post hoc test.
There was no significant difference between the non-GAD female group and the non-GAD male group in the advanced aspects of Theory of mind component (P=0.556). Also, female without anxiety and then male without anxiety had the highest mean score, and male with anxiety group and then female with anxiety group had the lowest mean score in the theory of mind component. All groups differ significantly in the emotion recognition and social cognition variables (P<0.05). Also, according to the current research, female without anxiety and then male without anxiety had the highest mean score, and male with anxiety group and then female with anxiety group had the lowest mean score in emotion recognition. However, there was no significant difference between the group of non-GAD females and the group of non-GAD males on the social cognition variable. Also, according to the present research, the female with anxiety group and then the male with anxiety group had the lowest average in social cognition.
Discussion
The current study compared the theory of mind, emotion recognition, and social cognition in teenagers with and without generalized anxiety disorder. The analysis comparing both groups, GAD and healthy controls revealed that patients showed significantly lower performance in ToM tasks. Earlier studies have shown that generalized anxiety is inversely associated with the theory of mind. This means that increased anxiety is associated with poor performance on theory of mind tasks [11, 12-14]. The result showed an inverse relationship between generalized anxiety and the theory of mind, which aligns with previous studies [11, 13, 15]. Additionally, research results in this area show that improving the theory of mind allows people to demonstrate appropriate responses in a variety of stressful and anxious situations [9, 10]. A different research article proposed that enhancing the theory of mind would cause increased individual flexibility and more appropriate responses to diverse situations, which could lower anxiety [13].
To explain the finding, it should be clarified that anxiety in general is associated with poor performance on theory of mind and empathy tasks. This finding means that anxious people perform worse and have more intense emotions on the theory of mind tasks than non-anxious people and that they focus more on what others are thinking and feeling toward their topic [15, 17]. Anxiety symptoms may be related to the theory of mental performance, as cognitive biases in perceiving others, as well as mocking and criticizing others, lead to expectations that they will be ridiculed and insulted. This can play a role in creating anxiety and leading to avoidance of various situations. Anxious people perform worse than others in decoding and theory-of-mind reasoning [45]. It also needs to be said that when people correctly guess the intentions and mental states of others, they will choose more appropriate behaviors and establish intimate relationships with others. This way, they will express their feelings and emotions in an interactive environment and reduce anxiety. However, people who have not fully developed their theory of mind will use inappropriate behaviors in communicating with others, which leads to a decrease in others’ desire to connect and ultimately increases their anxiety [41]. Based on previous research, there are numerous research that inconsistent with our results [16, 19]. One reason for inconsistency with early study is diversity test of ToM. It is important to note that some studies used more than one test of ToM, fulfilling inclusion criteria. This suggests significant heterogeneity seems to be associated with both the diversity of ToM tasks and the differences between GAD samples [17].
Additionally, adolescents with GAD performed worse than controls in facial emotion recognition in terms of accuracy. Based on the results obtained in this study, there were significant differences in emotional recognition in the groups of females with and without generalized anxiety disorder. Moreover, there were significant differences in the emotional recognition in the groups of males with and without generalized anxiety disorder. This means that with the increase of emotion recognition, the level of anxiety decreases and with the decrease of emotion recognition, the level of anxiety increases [20-24]. Some studies in the literature addressing emotion recognition in GAD demonstrate impairments [24, 26], while others find no significant differences between patients and healthy controls [18, 19]. To explain this problem, it can be said that experiencing excitement is a factor that affects social relationships and self-confidence. So, the more these people know about emotions, the more confident they will be, and therefore their anxiety will decrease. People can positively evaluate the current situation by using emotional awareness strategies and reduce anxiety by focusing on re-planning, making appropriate decisions, and using self-help strategies. Additionally, a lack of ability to recognize emotions can cause aggressive behaviors and disrupt decision-making processes by reducing inhibition and increasing physiological arousal [24-25].
Another explanation is that the symptoms of GAD are linked to a malfunction in the emotional areas of the brain, rather than the regions responsible for cognition and comprehension. A collection of brain regions, including the amygdala, insula, periaqueductal gray matter, locus coeruleus, and hypothalamus, collaborate to commence the initial process of managing stress. The responsibility for handling stressful situations and preparing the body for a reaction lies with these specific regions of the brain. Studies indicate that people suffering from generalized anxiety disorder demonstrate amygdala brain activity resembling that of scared animals [41].
Our findings replicated Fitzpatrick et al. (2018) in that this study also showed that adolescents with GAD have difficulty perceiving feelings based on recognizing emotion in facial expressions [17]. Fitzpatrick et al. also demonstrated that in their sample of adolescents with and without autism, there was no relationship between ToM and emotion recognition. The cognitive component of ToM (understanding the mental state of others) and the emotional component (making inferences about someone’s emotional state) may not involve a singular process [17]. It is also possible that the static nature of the facial emotion recognition task lacked the resolution necessary to uncover potentially subtle relationships. It is striking to notice the diversity of tests used to assess the recognition of emotions in the included studies. Some studies used static visual facial stimuli; in some studies, the intensity of emotions varied; in other articles, the facial expressions showed the same emotion intensity; and some used moving images for the assessment. In addition, methods of presenting photographs varied concerning the total number of photographs, the time presented, and so on. Although these differences may have affected the results and data interpretation, these methodological differences did not seem to represent a source of heterogeneity [18].
According to the findings of this study, there were significant differences in social cognition between the females with generalized anxiety disorder and healthy controls. Similar to previous studies, there were significant differences in social cognition between males with generalized anxiety disorder and healthy controls. Some studies report that children with SAD have poorer social skills than children with other anxiety disorders or non-anxious children [27-30]. However, others suggest that neither SAD (measured using semi-structured clinical assessments) nor social anxiety symptoms are significantly associated with dimensions of social cognition such as perspective taking and broad measures of understanding other’s thoughts and beliefs [42].
A systematic search identified 52 studies. Results showed mixed evidence for the association between social anxiety and lower-level social cognitive processes (emotion recognition and affect sharing) and a trend for a negative association with higher-level social cognitive processes (theory of mind and empathic accuracy) [43]. Specifically, cognitive deficits have been linked to worse functional outcomes such as poor self-care, decreased ability to live independently, poor social skills, inability to maintain successful employment, and poor compliance with medication regimens [41]. A meta-analysis found that social cognition explained 16% of the variance in community functioning while neuro-cognition explained only 6%. Community functioning was most strongly associated with the theory of mind followed by social perception and knowledge, verbal fluency, and emotion perception and processing [44]. Also, researchers conducted a review of 15 studies and concluded that social cognition acts as a mediator between neuro-cognition and functional outcomes [45].
A lack of consistent associations between social anxiety and social cognition may not be surprising given that some social cognition tasks require the ability to understand cognitive information (i.e. thoughts), whilst others require the ability to understand affective information. As such, it is plausible that the relationship differs between social anxiety and different domains/phenotypes of social cognition ability (henceforward referred to as social cognition; e.g. recognizing emotions or understanding other’s thoughts/beliefs) in children and adolescents [22, 41]. Authors explaining is that social perception provides the ability and facilities for a person to know himself better communicate with his world and others and make constructive decisions in this field. When people want to form their beliefs, they pay more attention to the opinions of others, and on this basis, social cognition leads to coherence in goals and attitudes. If more confidence and control accompanies people’s interaction with the environment, their behavior in dealing with events will be far more logical and mature, and they will experience less anxiety. But people who have social perception deficits rarely pay attention to the feelings of others and their relationships with others are often very low and incomplete they are known as social immatures and these people have a high level of social rejection that is seen as a result of a deficiency in social cognition. In fact, these people have a very weak performance in this type of cognition, which is precisely related to the social and psychological world and not the physical and logical world. This issue leads to an increase in their anxiety. So, by improving social perception, the level of anxiety can also be reduced.
Conclusion
Results showed that adolescents and young adults with generalized anxiety disorder were more susceptible to disturbances in theory of mind, emotional perception, and social cognition, especially females, compared with adolescents and adolescents without generalized anxiety disorder. Therefore, their strategies for controlling their thoughts and metacognitive beliefs lead them to emotional and neurological problems. Therefore, it is appropriate to teach them to practice alternative strategies to deal with threats. Not worrying and being able to control one’s emotions are essential skills for developing relationships, satisfying friendships, and social interactions in adolescents. Therefore, to increase the validity of the results and reduce the dropout effect, more samples should be followed in future studies. It is also recommended to control for gender in future studies and to conduct this study separately on women and boys. Further studies using ecological measures with larger, more homogeneous samples are needed to better identify factors that influence social cognitive outcomes in GAD.
Considering that every research has limitations, the current research also had limitations. Among them, due to the limited statistical population of the research, one should act with caution in the field of generalization of the findings, interpretation and etiological documentation of the investigated variables. Also, collecting data based on self-report scales and the non-clinical nature of the research samples is another limitation of this research. Likewise, lack of control of intervening variables was another limitation of this research.
Ethical Considerations
Compliance with ethical guidelines
The present study is in line with the Helsinki declaration. Furthermore, conducting this research, the ethical instructions of the Payame Noor University have been observed and prior to conducting the current work, the researchers obtained the approval of the Ethics Review Committee of Payame Noor University with the code of IR.PNU.REC.13401.321.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Tookktam Barati hokmabadi; Mehrangiz Pashapour Badr; Investigation, data collection, data analysis: Foruzan Razmjooei, Masumeh Javidi and Mahdieh Gholizadeh; Methodology and writing original draft: Masumeh Javidi and Tookktam Barati Hokmabadi; Review & editing: Foruzan Razmjooei, Masumeh Javidi, Mahdieh Gholizadeh and Mehrangiz Pashapour Badr.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors express their gratitude to all those who willingly took part in this research.
References
Generalized anxiety disorder (GAD) is a chronic uncontrollable excessive anxiety towards a variety of topics. It is one of the most prevalent anxiety disorders, affecting approximately 6% worldwide [1]. The prevalence of GAD, which typically begins in young adulthood, is about 2% in the adult population; the lifetime prevalence of GAD is around 4.7% [2]. The disorder is commonly accompanied by other anxiety disorders and depression, and its incidence rate in Iran is 10% overall and 5.2% within a year [3]. The occurrence of anxiety disorders may be linked to a concept known as May’s theory of mind (ToM) [4, 5, 6, 7, 8, 9, 10]. The concept of a theory of mind entails comprehending the thoughts and emotions of another individual through their behaviors [11]. Theory of mind involves the capability to comprehend and discuss the thoughts, wants, and pretend play of individuals. Having an awareness of your own thoughts and recognizing that others might possess divergent beliefs, wishes, and intentions [12].
People with GAD are more likely to underestimate or overestimate their affect and hostile behavior toward others [13]. For example, Zainal & Newman (2018), demonstrated that GAD status significantly interacted with state anxiety to predict the accuracy of global reasoning, cognitive reasoning, positive reasoning, and negative reasoning. Anxiety, as opposed to relaxation, causes people with GAD to display more accurate overall reasoning and cognitive ToM than controls, especially for negative cues. Participants with anxious but not relaxed GAD also interpreted negative cues significantly better than the norms. These results remained after controlling for gender, executive function, social anxiety, and depressive symptoms [14]. Moreover, Baez et al. (2023), in a meta-analysis including studies assessing ToM in patients diagnosed with GAD or social anxiety disorder) SAD (showed significant differences between groups, with lower scores in patients than healthy controls [15]. In addition, a number of authors performed meta-regression analyses to explore the relationship of relevant variables with ToM performance in GAD and SAD patients. Results showed that ToM performance was not significantly dependent on age, sex, years of education, or severity of anxiety [16, 17, 18, 19].
Emotions are a prerequisite for understanding the social environment and adopting competitive social behaviors. These are emotions that form a necessary part of social relationships, and people learn through facial expressions without actually talking about the situation and the wishes, concerns, desires, and intentions of the other party [15]. Aydin et al. (2019), demonstrated that dysfunctional metacognitive beliefs and disrupted emotion recognition in GAD patients compared to healthy controls. Furthermore, poor emotion recognition predicted GAD [20]. Additionally, a meta-analysis, including studies assessing emotion recognition ability in patients diagnosed with GAD or SAD, found that patients showed poorer functioning than healthy people. It is worth mentioning that, despite the significant results, only two studies comparing SAD patients and healthy controls showed significantly lower performance in the patients’ overall scores [21, 22]. Another meta-analysis showed that emotion recognition abilities were not significantly influenced by age, sex, years of education, or severity of anxiety [23]. In addition, many authors’ detailed literature searches to identify studies on explicit emotion recognition in patients with anxiety disorders and major depression compared to healthy participants showed differences in emotion recognition impairment between patients and controls with corresponding confidence intervals computed for each study [24, 25]. According to studies, adults with anxiety disorders have a significantly impaired ability to recognize emotions. In children with anxiety disorders, no significant impairment in emotion recognition was observed [26].
Another variable associated with general anxiety is social cognition [27-32]. Social cognition can be defined as the mental activities that underlie social interactions. This includes mental state attribution, emotion recognition, attributional style, and social cognition. There is also evidence that social cognitive impairments precede the onset of psychosis [29]. Social cognition involves various psychological processes that allow individuals to benefit from their membership in a social group [30]. Social cognitive impairment may be associated with poor functional outcomes, symptoms, and disability in social anxiety disorder (SAD) and GAD [31]. Therefore, deficits in social cognition may partly explain functional decline and poorer quality of life in people with anxiety disorders [32]. Pearcey et al. (2021) demonstrated that increased social anxiety is associated with lower social-cognitive abilities. Moderation analyses revealed specific associations in studies examining social anxiety in participants with and without ASD over 7 years of age and in studies assessing the relationship between anxiety social and specific aspects of the theory of mind (ToM). No significant association was identified between social anxiety and emotion recognition [22]. According to some authors’ assessments. They concluded that in both groups, total scores on all measures of social cognition were related to each other and that there were significant positive correlations between social cognition and age as well as between cognition social and IQ [29].
The studies mentioned have given different results, so unfortunately, there are still gaps in our knowledge about whether the theory of mind, recognizing emotions, and social cognition are involved in generalized anxiety disorder. Furthermore, there has been no simultaneous research on the study of the theory of mind, emotion recognition, and social cognition in teenagers with GAD or without it. However, not much is known about the relationships among these dimensions of social behavior. This study is one of the first in this field and is, in fact, innovative in this sense. Therefore, the purpose of this study was to compare the theory of mind, emotion recognition, and social cognition in adolescents with and without generalized anxiety disorder.
Materials and Methods
Study type and population
This clinic-based case-control study was conducted among teenagers refereed to psychological centers in Tehran, in 2022-23. A total of 120 sample in two groups of 60 teenagers with GAD (as cases) and 60 sex-matched teenagers without GAD (as controls) were compared. The sample size was calculated based on previous results with an effect size of 0.95, considering a power of 95% and type I error of 0.05 [33].
Participants were enrolled into the study if they pass the following inclusion/exclusion criteria: Pre-screening procedures were used to ensure that participants with GAD had been previously diagnosed with GAD by a licensed clinical psychologist or medical doctor based on DSM-IV_TR criteria, the participants consisted of 15-18 teenagers paired with a parent; no suicidal attempts during the past 6 months. Exclusion criteria were history or current psychiatric or neurological disorder or lack of consent from the participant or their legal guardian.; Lack of consent to complete questionnaires, and incomplete questionnaires. After receiving permission from the responsible department of Payame Noor University and the respective principals, the researcher first prepared the list of six psychological centers in the district 7, and then purposefully selected sample members from among the files of people with generalized anxiety disorder in psychological centers based on the inclusion and exclusion criteria. In this study, healthy controls were selected as convenience sampling method. The control group included teenagers who had referred to the study centers for reasons other than generalized anxiety disorder, and were matched to the experimental group in terms of age and sex. Written informed consent for participation and publication was obtained from each participant or legal guardian, respectively.
Study procedure
Following with the coordination of the officials of the psychological centers, the target families and teenagers were contacted by phone to go to the psychological center of Karane located in the 7th region to complete the questionnaires. The researcher first interviewed all the teenagers and after explaining the objectives of the research. The researcher employed multiple methods to collect data, including self-report questionnaires completed by participants (the TOM & social cognition questionnaires), oral recordings conducted by the researcher, and interviews (Ekman 60-faces test [EK-60F]). The time of conducting the interviews and completing the questionnaires was about 120 hours and the researcher carried out the research in 36 days within two months. Data has been gathered from 60 participants diagnosed with GAD and from 60 normal control participants.
Measures
Theory of mind scale (TOM): The TOM questionnaire was created by Steerneman et al. in 1999 to assess the theory of mind in normal children, adolescents (Simon & Saunders), and those with widespread disorders, which has proven its validity as evidence [34]. This questionnaire provides information about a person’s social understanding, sensitivity, and insight, as well as the degree to which one can accept the feelings and thoughts of others. The main form of the scale includes 78 questions in 3 subtests. Subtests include Introduction to Theory of Mind (29 questions), Basic Statement of a True Theory of Mind (33 questions), and Advanced Aspects of Theory of Mind (16 questions) question). This scale was conducted as an interview, correct answers receive 1 point, and incorrect answers receive 0 points. The range of people’s scores on the subscales was 0 to 29 (first subset), 0 to 33 (second subset), and 0 to 16 (third subset). The total score of the instrument ranges from 38 to 190, and a higher score indicates a more favorable theory of mind. The researchers reported the scale’s reliability coefficient to be 0.72 the test’s concurrent validity to be 0.89 and its content validity to be 0.96 [34]. In Iran, the internal homogeneity of the test was calculated using Cronbach’s α coefficient of 0.86 [35]. In current study, the author found that the Cronbach’s α coefficient of this scale is 0.871.
Social cognition questionnaire: This questionnaire was created by Nejati, et al. with the aim of investigating the state of social cognition on students and teenagers [36]. The questionnaire has 19 items that are measured in a 5-point Likert scale. The scoring method of the questionnaire is such that the option includes almost never (1), rarely (2), sometimes (3), often (4) and almost always (5). This questionnaire has 4 subscales of reading the teacher’s mind, detecting educational threats, self-awareness, and understanding the educational environment. The total social cognition score (range 19-95) is calculated as the sum of the subscale scores. Cronbach’s α was also used to check the reliability of the scale, and the coefficient was 0.66 for self-awareness, 0.70 for reading the teacher’s mind, 0.55 for understanding the educational environment, and finally 0.72 for detecting educational threats [37]. In this research, the researcher found the Cronbach’s α coefficient of this scale to be 0.77.
Ekman 60-faces test (EK-60F): Paul Ekman & Wallace. Friesen created the Ekman 60 faces (1986) with the purpose of measuring emotion recognition ability [38]. This test is commonly used for research on mental and neurological disorders, including neurological diseases. Subjects were administered the EK-60F after a pre-test of basic semantic emotion recognition and were asked to verbally provide an example for each of the six emotions (e.g. “tell me that you feel happy” and “I feel happy” when I receive a gift). Any incorrect response resulted in exclusion from the current study. The EK-60F test comprises 60 weighted face images depicting the faces of 10 actors (6 females, 4 male), each expressing six basic emotions (i.e. happy, sad, angry, fear, surprise, disgust). Subjects were asked to respond verbally and choose the label that best described the facial expression the actor was displaying. According to the method of Ekman and Friesen, each image was displayed for 5 seconds [39]. The total test score is from 0 to 60, where a score of 60 represents the best possible performance and each basic sensation has a sub-score of up to 10 points. The reliability of the test in Iran was checked using Cronbach’s α method and the researchers reported a value of 0.79 for the reliability of this scale [40]. In this study, the author found that the Cronbach’s α coefficient of this scale was 0.81.
Statistical analysis
Data were described in terms of Mean±SD or frequency and percent. One-way analysis of variance and post hoc test were used to compare continues variables among four groups of male and female with and without GAD. All analysis was performed using SPSS software, version 27. P<0.05 was considered as significant.
Results
In this sex-matched case control study, 120 teenagers (30 females with generalized anxiety disorder, 30 females without generalized anxiety disorder, 30 males with generalized anxiety disorder, and 30 males without generalized anxiety disorder) from 6 psychological center were participated. The majority of the participants fell within the age range of 15 to 16 years (60.8%) and anxiety) and were in the field of humanities (45%) (Table 1).
According to Table 2, the mean scores of research variables in the group without GAD in both males and females were higher than the group without GAD.
Similarly, the mean value of all research variables in the females were higher than correspondent males in both groups.
Table 3 demonstrates paired wise comparison of study variables according to sex and group of study using Tuckey’s post hoc test.
There was no significant difference between the non-GAD female group and the non-GAD male group in the advanced aspects of Theory of mind component (P=0.556). Also, female without anxiety and then male without anxiety had the highest mean score, and male with anxiety group and then female with anxiety group had the lowest mean score in the theory of mind component. All groups differ significantly in the emotion recognition and social cognition variables (P<0.05). Also, according to the current research, female without anxiety and then male without anxiety had the highest mean score, and male with anxiety group and then female with anxiety group had the lowest mean score in emotion recognition. However, there was no significant difference between the group of non-GAD females and the group of non-GAD males on the social cognition variable. Also, according to the present research, the female with anxiety group and then the male with anxiety group had the lowest average in social cognition.
Discussion
The current study compared the theory of mind, emotion recognition, and social cognition in teenagers with and without generalized anxiety disorder. The analysis comparing both groups, GAD and healthy controls revealed that patients showed significantly lower performance in ToM tasks. Earlier studies have shown that generalized anxiety is inversely associated with the theory of mind. This means that increased anxiety is associated with poor performance on theory of mind tasks [11, 12-14]. The result showed an inverse relationship between generalized anxiety and the theory of mind, which aligns with previous studies [11, 13, 15]. Additionally, research results in this area show that improving the theory of mind allows people to demonstrate appropriate responses in a variety of stressful and anxious situations [9, 10]. A different research article proposed that enhancing the theory of mind would cause increased individual flexibility and more appropriate responses to diverse situations, which could lower anxiety [13].
To explain the finding, it should be clarified that anxiety in general is associated with poor performance on theory of mind and empathy tasks. This finding means that anxious people perform worse and have more intense emotions on the theory of mind tasks than non-anxious people and that they focus more on what others are thinking and feeling toward their topic [15, 17]. Anxiety symptoms may be related to the theory of mental performance, as cognitive biases in perceiving others, as well as mocking and criticizing others, lead to expectations that they will be ridiculed and insulted. This can play a role in creating anxiety and leading to avoidance of various situations. Anxious people perform worse than others in decoding and theory-of-mind reasoning [45]. It also needs to be said that when people correctly guess the intentions and mental states of others, they will choose more appropriate behaviors and establish intimate relationships with others. This way, they will express their feelings and emotions in an interactive environment and reduce anxiety. However, people who have not fully developed their theory of mind will use inappropriate behaviors in communicating with others, which leads to a decrease in others’ desire to connect and ultimately increases their anxiety [41]. Based on previous research, there are numerous research that inconsistent with our results [16, 19]. One reason for inconsistency with early study is diversity test of ToM. It is important to note that some studies used more than one test of ToM, fulfilling inclusion criteria. This suggests significant heterogeneity seems to be associated with both the diversity of ToM tasks and the differences between GAD samples [17].
Additionally, adolescents with GAD performed worse than controls in facial emotion recognition in terms of accuracy. Based on the results obtained in this study, there were significant differences in emotional recognition in the groups of females with and without generalized anxiety disorder. Moreover, there were significant differences in the emotional recognition in the groups of males with and without generalized anxiety disorder. This means that with the increase of emotion recognition, the level of anxiety decreases and with the decrease of emotion recognition, the level of anxiety increases [20-24]. Some studies in the literature addressing emotion recognition in GAD demonstrate impairments [24, 26], while others find no significant differences between patients and healthy controls [18, 19]. To explain this problem, it can be said that experiencing excitement is a factor that affects social relationships and self-confidence. So, the more these people know about emotions, the more confident they will be, and therefore their anxiety will decrease. People can positively evaluate the current situation by using emotional awareness strategies and reduce anxiety by focusing on re-planning, making appropriate decisions, and using self-help strategies. Additionally, a lack of ability to recognize emotions can cause aggressive behaviors and disrupt decision-making processes by reducing inhibition and increasing physiological arousal [24-25].
Another explanation is that the symptoms of GAD are linked to a malfunction in the emotional areas of the brain, rather than the regions responsible for cognition and comprehension. A collection of brain regions, including the amygdala, insula, periaqueductal gray matter, locus coeruleus, and hypothalamus, collaborate to commence the initial process of managing stress. The responsibility for handling stressful situations and preparing the body for a reaction lies with these specific regions of the brain. Studies indicate that people suffering from generalized anxiety disorder demonstrate amygdala brain activity resembling that of scared animals [41].
Our findings replicated Fitzpatrick et al. (2018) in that this study also showed that adolescents with GAD have difficulty perceiving feelings based on recognizing emotion in facial expressions [17]. Fitzpatrick et al. also demonstrated that in their sample of adolescents with and without autism, there was no relationship between ToM and emotion recognition. The cognitive component of ToM (understanding the mental state of others) and the emotional component (making inferences about someone’s emotional state) may not involve a singular process [17]. It is also possible that the static nature of the facial emotion recognition task lacked the resolution necessary to uncover potentially subtle relationships. It is striking to notice the diversity of tests used to assess the recognition of emotions in the included studies. Some studies used static visual facial stimuli; in some studies, the intensity of emotions varied; in other articles, the facial expressions showed the same emotion intensity; and some used moving images for the assessment. In addition, methods of presenting photographs varied concerning the total number of photographs, the time presented, and so on. Although these differences may have affected the results and data interpretation, these methodological differences did not seem to represent a source of heterogeneity [18].
According to the findings of this study, there were significant differences in social cognition between the females with generalized anxiety disorder and healthy controls. Similar to previous studies, there were significant differences in social cognition between males with generalized anxiety disorder and healthy controls. Some studies report that children with SAD have poorer social skills than children with other anxiety disorders or non-anxious children [27-30]. However, others suggest that neither SAD (measured using semi-structured clinical assessments) nor social anxiety symptoms are significantly associated with dimensions of social cognition such as perspective taking and broad measures of understanding other’s thoughts and beliefs [42].
A systematic search identified 52 studies. Results showed mixed evidence for the association between social anxiety and lower-level social cognitive processes (emotion recognition and affect sharing) and a trend for a negative association with higher-level social cognitive processes (theory of mind and empathic accuracy) [43]. Specifically, cognitive deficits have been linked to worse functional outcomes such as poor self-care, decreased ability to live independently, poor social skills, inability to maintain successful employment, and poor compliance with medication regimens [41]. A meta-analysis found that social cognition explained 16% of the variance in community functioning while neuro-cognition explained only 6%. Community functioning was most strongly associated with the theory of mind followed by social perception and knowledge, verbal fluency, and emotion perception and processing [44]. Also, researchers conducted a review of 15 studies and concluded that social cognition acts as a mediator between neuro-cognition and functional outcomes [45].
A lack of consistent associations between social anxiety and social cognition may not be surprising given that some social cognition tasks require the ability to understand cognitive information (i.e. thoughts), whilst others require the ability to understand affective information. As such, it is plausible that the relationship differs between social anxiety and different domains/phenotypes of social cognition ability (henceforward referred to as social cognition; e.g. recognizing emotions or understanding other’s thoughts/beliefs) in children and adolescents [22, 41]. Authors explaining is that social perception provides the ability and facilities for a person to know himself better communicate with his world and others and make constructive decisions in this field. When people want to form their beliefs, they pay more attention to the opinions of others, and on this basis, social cognition leads to coherence in goals and attitudes. If more confidence and control accompanies people’s interaction with the environment, their behavior in dealing with events will be far more logical and mature, and they will experience less anxiety. But people who have social perception deficits rarely pay attention to the feelings of others and their relationships with others are often very low and incomplete they are known as social immatures and these people have a high level of social rejection that is seen as a result of a deficiency in social cognition. In fact, these people have a very weak performance in this type of cognition, which is precisely related to the social and psychological world and not the physical and logical world. This issue leads to an increase in their anxiety. So, by improving social perception, the level of anxiety can also be reduced.
Conclusion
Results showed that adolescents and young adults with generalized anxiety disorder were more susceptible to disturbances in theory of mind, emotional perception, and social cognition, especially females, compared with adolescents and adolescents without generalized anxiety disorder. Therefore, their strategies for controlling their thoughts and metacognitive beliefs lead them to emotional and neurological problems. Therefore, it is appropriate to teach them to practice alternative strategies to deal with threats. Not worrying and being able to control one’s emotions are essential skills for developing relationships, satisfying friendships, and social interactions in adolescents. Therefore, to increase the validity of the results and reduce the dropout effect, more samples should be followed in future studies. It is also recommended to control for gender in future studies and to conduct this study separately on women and boys. Further studies using ecological measures with larger, more homogeneous samples are needed to better identify factors that influence social cognitive outcomes in GAD.
Considering that every research has limitations, the current research also had limitations. Among them, due to the limited statistical population of the research, one should act with caution in the field of generalization of the findings, interpretation and etiological documentation of the investigated variables. Also, collecting data based on self-report scales and the non-clinical nature of the research samples is another limitation of this research. Likewise, lack of control of intervening variables was another limitation of this research.
Ethical Considerations
Compliance with ethical guidelines
The present study is in line with the Helsinki declaration. Furthermore, conducting this research, the ethical instructions of the Payame Noor University have been observed and prior to conducting the current work, the researchers obtained the approval of the Ethics Review Committee of Payame Noor University with the code of IR.PNU.REC.13401.321.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Tookktam Barati hokmabadi; Mehrangiz Pashapour Badr; Investigation, data collection, data analysis: Foruzan Razmjooei, Masumeh Javidi and Mahdieh Gholizadeh; Methodology and writing original draft: Masumeh Javidi and Tookktam Barati Hokmabadi; Review & editing: Foruzan Razmjooei, Masumeh Javidi, Mahdieh Gholizadeh and Mehrangiz Pashapour Badr.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors express their gratitude to all those who willingly took part in this research.
References
- Alahmari K, Duh H, Skarbez R. Outcomes of virtual reality technology in the management of generalised anxiety disorder: A systematic review and meta-analysis. Behav Inf Technol. 2023; 42(14):2353-65. [DOI:10.1080/0144929X.2022.2118078]
- Madonna D, Delvecchio G, Soares JC, Brambilla P. Structural and functional neuroimaging studies in generalized anxiety disorder: A systematic review. Braz J Psychiatry. 2019; 41(4):336-62. [DOI:10.1590/1516-4446-2018-0108] [PMID]
- Ghaderi F, Akrami N, Namdari K, Abedi A. [Developing an integrated psychotherapy model of generalized anxiety disorder comorbid with emotional disorders; a qualitative approach (Persian)]. Iran J Rehabil Res. 2020; 6(4):70-82. [DOI:10.29252/ijrn-06048]
- Ho MK, Saxe R, Cushman F. Planning with theory of mind. Trends Cogn Sci. 2022; 26(11):959-71. [DOI:10.1016/j.tics.2022.08.003] [PMID]
- Rakoczy H. Foundations of theory of mind and its development in early childhood. Nat Rev Psychol. 2022; 1(4):223-35. [DOI:10.1038/s44159-022-00037-z]
- Nestor BA, Sutherland S, Garber J. Theory of mind performance in depression: A meta-analysis. J Affect Disord. 2022; 303:233-44. [DOI:10.1016/j.jad.2022.02.028] [PMID]
- Kosinski M. Theory of mind might have spontaneously emerged in large language models. arXiv preprint. 2023. [DOI:10.48550/arXiv.2302.02083]
- Shteynberg G, Hirsh JB, Wolf W, Bargh JA, Boothby EB, Colman AM, et al. Theory of collective mind. Trends Cogn Sci. 2023; 27(11):1019-31. [Link]
- Gazelle H, Lundin JK, Bosacki SL. Theory of mind, gender, gains in friendships versus peer acceptance and anxious solitude from middle childhood through early adolescence. Soc Dev. 2023; 32(2):651-71. [DOI:10.1111/sode.12654]
- McCauley JB, Harris MA, Zajic MC, Swain-Lerro LE, Oswald T, McIntyre N, et al. Self-esteem, internalizing symptoms, and theory of mind in youth with autism spectrum disorder. J Clin Child Adolesc Psychol. 2019; 48(3):400-11. [DOI:10.1080/15374416.2017.1381912] [PMID]
- Castellano-Navarro A, Guillen-Salazar F, Albiach-Serrano A. Competitive children, cooperative mothers? Effect of various social factors on the retrospective and prospective use of theory of mind. J Exp Child Psychol. 2020; 190:104715. [DOI:10.1016/j.jecp.2019.104715] [PMID]
- Wang Z, Luo Y, Zhang Y, Chen L, Zou Y, Xiao J, et al. Heart rate variability in generalized anxiety disorder, major depressive disorder and panic disorder: A network meta-analysis and systematic review. J Affect Disord. 2023; 330:259-66. [DOI:10.1016/j.jad.2023.03.018] [PMID]
- Caputi M, Bosacki S. The role of gender in the relation among anxiety, theory of mind, and well-being in early adolescents. J Early Adolesc. 2023; 43(7):845-66. [DOI:10.1177/02724316221130440]
- Zainal NH, Newman MG. Worry amplifies theory-of-mind reasoning for negatively valenced social stimuli in generalized anxiety disorder. J Affect Disord. 2018; 227:824-33. [DOI:10.1016/j.jad.2017.11.084] [PMID]
- Baez S, Tangarife MA, Davila-Mejia G, Trujillo-Güiza M, Forero DA. Performance in emotion recognition and theory of mind tasks in social anxiety and generalized anxiety disorders: A systematic review and meta-analysis. Front Psychiatry. 2023; 14:1192683. [DOI:10.3389/fpsyt.2023.1192683] [PMID]
- Santarelli G, Innocenti M, Faggi V, Miglietta V, Colpizzi I, Galassi F, et al. Preliminary evidence for a Theory of Mind impairment in patients with Anxiety Disorders. Eur Psychiatry. 2022; 65(S1):S185-6. [DOI:10.1192/j.eurpsy.2022.489]
- Fitzpatrick P, Frazier JA, Cochran D, Mitchell T, Coleman C, Schmidt RC. Relationship between theory of mind, emotion recognition, and social synchrony in adolescents with and without autism. Front Psychol. 2018; 9:1337. [DOI:10.3389/fpsyg.2018.01337] [PMID]
- Maoz K, Eldar S, Stoddard J, Pine DS, Leibenluft E, Bar-Haim Y. Angry-happy interpretations of ambiguous faces in social anxiety disorder. Psychiatry Res. 2016; 241:122-7.[DOI:10.1016/j.psychres.2016.04.100] [PMID]
- Tseng HH, Huang YL, Chen JT, Liang KY, Lin CC, Chen SH. Facial and prosodic emotion recognition in social anxiety disorder. Cogn Neuropsychiatry. 2017; 22(4):331-45. [DOI:10.1080/13546805.2017.1330190] [PMID]
- Aydın O, Balıkçı K, Çökmüş FP, Ünal Aydın P. The evaluation of metacognitive beliefs and emotion recognition in panic disorder and generalized anxiety disorder: Effects on symptoms and comparison with healthy control. Nord J Psychiatry. 2019; 73(4-5):293-301. [DOI:10.1080/08039488.2019.1623317] [PMID]
- Rappaport LM, Di Nardo N, Brotman MA, Pine DS, Leibenluft E, Roberson-Nay R, et al. Pediatric anxiety associated with altered facial emotion recognition. J Anxiety Disord. 2021; 82:102432. [DOI:10.1016/j.janxdis.2021.102432] [PMID]
- Pearcey S, Gordon K, Chakrabarti B, Dodd H, Halldorsson B, Creswell C. Research review: The relationship between social anxiety and social cognition in children and adolescents: A systematic review and meta-analysis. J Child Psychol Psychiatry. 2021; 62(7):805-21. [DOI:10.1111/jcpp.13310] [PMID]
- Rutter LA, Scheuer L, Vahia IV, Forester BP, Smoller JW, Germine L. Emotion sensitivity and self-reported symptoms of generalized anxiety disorder across the lifespan: A population-based sample approach. Brain Behav. 2019; 9(6):e01282. [DOI:10.1002/brb3.1282] [PMID]
- Tetik D, Gica S, Bestepe EE, Buyukavsar A, Gulec H. Emotional information processing and assessment of cognitive functions in social anxiety disorder: An event-related potential study. Clin EEG Neurosci. 2022; 53(2):104-13.[DOI:10.1177/1550059420981506] [PMID]
- Oh KS, Lee WH, Kim S, Shin DW, Shin YC, Lim SW. Impaired facial expression recognition in patients with social anxiety disorder: A case-control study. Cogn Neuropsychiatry. 2018; 23(4):218-28. [DOI:10.1080/13546805.2018.1462695] [PMID]
- Vidal-Ribas P, Brotman MA, Salum GA, Kaiser A, Meffert L, Pine DS, et al. Deficits in emotion recognition are associated with depressive symptoms in youth with disruptive mood dysregulation disorder. Depress Anxiety. 2018; 35(12):1207-17. [DOI:10.1002/da.22810] [PMID]
- Pawluk EJ, Koerner N, Kuo JR, Antony MM. An experience sampling investigation of emotion and worry in people with generalized anxiety disorder. J Anxiety Disord. 2021; 84:102478. [DOI:10.1016/j.janxdis.2021.102478] [PMID]
- Barbato M, Liu L, Bearden CE, Cadenhead KS, Cornblatt BA, Keshavan M, et al. Migrant status, clinical symptoms and functional outcome in youth at clinical high risk for psychosis: Findings from the NAPLS-3 study. Soc Psychiatry Psychiatr Epidemiol. 2023; 58(4):559-68. [DOI:10.1007/s00127-022-02383-y] [PMID]
- Henry JD, Grainger SA, von Hippel W. Determinants of social cognitive aging: Predicting resilience and risk. Annu Rev Psychol. 2023; 74:167-92. [DOI:10.1146/annurev-psych-033020-121832] [PMID]
- Gkika S, Wittkowski A, Wells A. Social cognition and metacognition in social anxiety: A systematic review. Clin Psychol Psychother. 2018; 25(1):10-30. [PMID]
- Epley N, Kardas M, Zhao X, Atir S, Schroeder J. Undersociality: Miscalibrated social cognition can inhibit social connection. Trends Cogn Sci. 2022; 26(5):406-18. [DOI:10.1016/j.tics.2022.02.007] [PMID]
- Roheger M, Hranovska K, Martin AK, Meinzer M. A systematic review and meta-analysis of social cognition training success across the healthy lifespan. Sci Rep. 2022; 12(1):3544. [DOI:10.1038/s41598-022-07420-z] [PMID]
- Hashemi N, Babakhani F, Sheikhhoseini R. The effect of water yoga exercises on the intensity and pain duration in girls with primary dysmenorrhea. Women Health Bull. 2022; 9(2):61-9. [Link]
- Muris P, Steerneman P, Meesters C, Merckelbach H, Horselenberg R, van den Hogen T, et al. The TOM test: A new instrument for assessing theory of mind in normal children and children with pervasive developmental disorders. J Autism Dev Disord. 1999; 29(1):67-80. [DOI:10.1023/A:1025922717020] [PMID]
- Koosali F, Sadeghi J, Barjasteh H, Kiapour A. [The modeling role of emotional processing in the relationship between theories of mind with academic performance in bilingual students (Persian)]. Iran J Educ Soc. 2022; 7(2):266-76. [Link]
- Nejati V, Kamari S, Jafari S. [Construction and examine the psychometric characteristics of student social cognition questionnaire (SHAD) (Persian)]. Soc Cogn. 2018; 7(2):123-44. [DOI:10.30473/sc.2018.29262.1931]
- Rihani B, Derakhshan M, Shafiei M, Alizadeh M, Zarei R. [Intelligence believes and academic engagement: Original research mediating role of social cognition (Persian)]. Educ Psychol Q. 2021; 17(60):249-70. [Link]
- Ekman P, Friesen WV. Measuring facial movement. Environ Psychol Nonverbal Behav. 1976; 1:56-75. [DOI:10.1007/BF01115465]
- O’Sullivan M, Ekman P, Geher G. Facial expression recognition and emotional intelligence. In: Leeland KB, editor. Face recognition: New research. New York: Nova Science Publishers; 2008. [Link]
- Alipor A, Hassani F, Dosti R. [Comparison of the ability to recognize facial emotional states with the premiere hand control in women receiving treatment for botulinum (Botox) and normal people (Persian)]. Soc Cogn. 2019; 8(1):39-50. [Link]
- Li J, Zhong Y, Ma Z, Wu Y, Pang M, Wang C, et al. Emotion reactivity-related brain network analysis in generalized anxiety disorder: A task fMRI study. BMC Psychiatry. 2020; 20(1):429. [PMID]
- Colonnesi C, Nikolić M, de Vente W, Bögels SM. Social anxiety symptoms in young children: Investigating the interplay of theory of mind and expressions of shyness. J Abnorm Child Psychol. 2017; 45(5):997-1011. [DOI:10.1007/s10802-016-0206-0] [PMID]
- Alvi T, Kumar D, Tabak BA. Social anxiety and behavioral assessments of social cognition: A systematic review. J Affect Disord. 2022; 311:17-30. [DOI:10.1016/j.jad.2022.04.130] [PMID]
- Velikonja T, Fett AK, Velthorst E. Patterns of nonsocial and social cognitive functioning in adults with autism spectrum disorder: A systematic review and meta-analysis. JAMA Psychiatry. 2019; 76(2):135-51. [DOI:10.1001/jamapsychiatry.2018.3645] [PMID]
- Yilmaz G, Yildirim EA, Tabakcı AS. Comparison of social-evaluative anxiety and theory of mind functions in social anxiety disorder, schizophrenia, and healthy controls. Psychopathology. 2023; 56(6):440-52. [DOI:10.1159/000529880] [PMID]
Article Type: Original Contributions |
Subject:
Health Management
Received: 2023/10/1 | Accepted: 2024/01/16 | Published: 2024/01/1
Received: 2023/10/1 | Accepted: 2024/01/16 | Published: 2024/01/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Contact Information
cjhr Office, Guilan University of Medical Sciences
P.O.Box 93345-41938, Rasht, Iran
Journal Tel: +9813 33335820
Publisher Tel: +9821 453 55 000
Email: cjhr.gums@gmail.com
