

Volume 9, Issue 1 (1-2024)
CJHR 2024, 9(1): 1-8 |
Back to browse issues page



Ethics code: IR.GUMS.REC.1398.276.
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ramaji T, Pakseresht S, Joukar F, Reza Soltani P, Atrkar Roshan Z, Mansour-Ghanaei F. Determination of vitamin D serum levels in women receiving vitamin supplementation: The PERSIAN Guilan Cohort Study. CJHR 2024; 9 (1) :1-8
URL: http://cjhr.gums.ac.ir/article-1-338-en.html
URL: http://cjhr.gums.ac.ir/article-1-338-en.html
Tayebeh Ramaji1 

 , Sedigheh Pakseresht2 , Farahnaz Joukar3 , Parvaneh Reza Soltani1 , Zahra Atrkar Roshan4 , Fariborz Mansour-Ghanaei * 5
, Sedigheh Pakseresht2 , Farahnaz Joukar3 , Parvaneh Reza Soltani1 , Zahra Atrkar Roshan4 , Fariborz Mansour-Ghanaei * 5
, Sedigheh Pakseresht2 , Farahnaz Joukar3 , Parvaneh Reza Soltani1 , Zahra Atrkar Roshan4 , Fariborz Mansour-Ghanaei * 5
1- Department of midwifery, School of nursing and midwifery, Guilan University of Medical Sciences, Rasht, Iran
2- Social Determinants of Health Research Center, Reproductive Health Research Center, Department of midwifery, School of nursing and midwifery, Guilan University of Medical Sciences, Rasht, Iran
3- Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran.
4- Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran
5- Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran , fmansourghanaei@gmail.com
2- Social Determinants of Health Research Center, Reproductive Health Research Center, Department of midwifery, School of nursing and midwifery, Guilan University of Medical Sciences, Rasht, Iran
3- Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran.
4- Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran
5- Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran , fmansourghanaei@gmail.com
Full-Text [PDF 510 kb]
(97 Downloads)
| Abstract (HTML) (281 Views)
Full-Text: (30 Views)
Introduction
Vitamin D is a fat-soluble vitamin and a hormone precursor [1] and is known as a very important indicator of health [2]. This vitamin is both a nutrient and a hormone precursor and has many benefits for human health. The health benefits of vitamin D go beyond bone health, as confirmed in various studies. In addition to regulating calcium metabolism, this vitamin also regulates insulin, reduces the risk of diabetes and cancer, produces renin, and helps to eliminate infectious agents and regulate cell growth¸ Strengthens the immune system¸ this vitamin also helps to cure many important diseases [2, 3]. Recently, vitamin D has attracted a great deal of attention around the world, and it has been attributed as a drug of the last decade due to its widespread deficiency in the world [3]. Vitamin D also plays a significant role in human fertility [4]¸and has several effects on pregnancy, maternal and fetal health [5]. Vitamin D is available in two forms: Vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol) [6]. Sources of vitamin D are nutrition, sunlight and supplements [7]. Vitamin D is measured through determination of 25 hydroxyvitamin D3, which is present in the serum. It is biologically neutral and has a half-life of 2-3 weeks [8, 9, 10]. Vitamin D deficiency usually refers to serum levels of 25-hydroxy D3 plasma <50 nmol per liter (20 ng/mL) [11]. The main risk factors for vitamin D deficiency include old age, dark skin pigmentation, and any barrier to the sun’s ultraviolet light reaching the skin, such as full body coverage, spending more time at home, and air pollution [12]. Vitamin D deficiency is a public health concern around the world [13]. Prevention, early diagnosis and treatment of vitamin D deficiency is a key tool to reduce the effects of vitamin D deficiency on the health of the body, especially in the elderly [14]. If left untreated, it can lead to reduced quality of life and increased costs due to a lack of proper attention to this health problem [13].
Vitamin D deficiency has been reported in all over the world [15]. Its prevalence is recorded in all age groups, including toddlers, school children, adult men and women, the elderly, pregnant women, and infants in rural and urban areas [16]. Vitamin D deficiency has affected more than one billion people worldwide [11]. In a review study by Chakhtoura et al¸ in the Middle East and North African region, prevalence of hypovitaminosis D among children and adolescents is 12-96%, in pregnant women, 90 to 54%, and in adults between 96 and 44% with an average of 25 hydroxy D3 between 11 and 20 ng/mL [17]. There is a high prevalence of vitamin D deficiency in Iran in different age groups [18]¸ In a review study by Tabarizi et al, the percentage of vitamin D deficiency in pregnant women was 60.4% and among adult women was 61.9% [4]. Inadequate intake of vitamin D from its main source, which is sunlight, due to the type of clothing worn by women, the presence of many cloudy and rainy days in the year, latitude, lack of exposure to sunlight, and the use of sunscreen creams are possible reasons for the prevalence of deficiency of vitamin D among women in northern Iran [3, 19].The complications of vitamin D deficiency can be prevented by effective preventive measures such as vitamin D supplementation. Therefore¸ a preventive policy¸ including distribution of vitamin D mega dose supplementation was implemented in recent years in Iran (50000 units of vitamin D supplement tablets per month), including in Guilan. But there is lack of awareness about the serum status of vitamin D in women covered by this project in Guilan. So, the aim of this study was to determine the serum levels of vitamin D in women participating supplementation program.
Materials and Methods
This study was conducted to investigate the serum status of vitamin D among women receiving vitamin supplementation participating in the PERSIAN Guilan Cohort study (PGCS). PGCS is a prospective, population-based cohort study in Guilan, the northern province of Iran, recruited between October 8, 2014, and January 20, 2017 [20], as part of the prospective epidemiological research studies in Iran (PERSIAN) [21]. Different districts of the province were chosen to include different socioeconomic status levels including urban areas and 39 villages. The sampling and data collection methods have been previously described in detail [20].
This cross-sectional analytical study was conducted on a subset of PGCS, which aimed to determine the serum level of vitamin D in women recieving vitamin D supplements (50000 IU pearl vitamin D). A total of 614 people (10.9%) out of 5633 eligible women were included. The desired information was collected through interviews from the women referring to the primary health service centers (health centers and comprehensive urban health service centers) in Some’e Sara district, Guilan Province. Demographic and social characteristics including weight, height, body mass index, age, employment status, level of education, marital status, place of residence status, housing area, alcohol consumption, and how to take vitamin D supplement tablets were collected using a data collection form. Weight was measured by a scale with minimal cloths without shoes in kilograms and height in a normal standing position using a tape measure. Body mass index (BMI) was measured as weight in kilogram divided by square of height in meter. BMI of the participants was classified in four categories of underweight (BMI <18.5), normal (BMI between 18.5 and 24.9), overweight (BMI between 25 and 29.9), and obese (BMI >30) [20].
In the second part to assess the serum status of vitamin D, 2 cc of venous blood samples were taken from 563 participants (51 non-participants in the study). Blood samples were collected from all individuals using Vacutainers (Greiner Bio-One International GmbH, Kremsmunster, Austria). Whole blood samples were collected in EDTA (K3) tubes (Becton Dickinson, France). Serum 25(OH)D3 was determined by using a commercially available electrochemiluminescence immunoassay with Roche Elecsys 2010 and Cobas E411 auto analyzer (Roche Diagnostics GmbH, Mannheim, Germany) [22]. Serum levels of vitamin D were then classified into deficient: 25(OH)D3<10, insufficient: 10-20, and sufficient: >20 ng/mL [23].
Data analysis was performed using SPSS statistical software, version 22 (SPSS Inc, Chicago, IL, USA). Descriptive and inferential statistics were also used in data analysis, so that categorical variables were presented as frequency (number) and percentage and quantitative variables as Mean±SD. Participants due to the concentration of 25-hydroxy D3 serum in to 3 categories of deficiency (<10), insufficient (between 10-20) and sufficient (>20 ng/mL) were divided, and the chi-square test was used to compare how to take vitamin D supplements (weekly, monthly, and annually) and individual-social specifications with serum vitamin D levels, and P<0.05 to statistically significant.
Results
Of the 5633 women participating in the cohort study, 614(10.9%) were vitamin D supplement users. The results of this study showed that Mean±SD age of subjects were 50.3±8.7 (ranged 36 to 70) years. Demographic and social characteristics of supplementary consumers showed that 42.8% the subjects were in the age group 40-50 years old, 48.2% were obese, 77.4% of them were unemployed, 29.8% had high school level of education, 88.1% are married, 87.5% have home as a owner, 63% have a residential house with an area of 71 to 116 square meters, 62.2% urban, 99.8% have no alcohol consumption, and 65.3% have an annual consumption Vitamin D supplementary tablets. The majority of participants (65.4%) had sufficient serum levels of vitamin D. The Mean±SD of serum vitamin D was 31.63±15.336 ng/mL (Table 1).

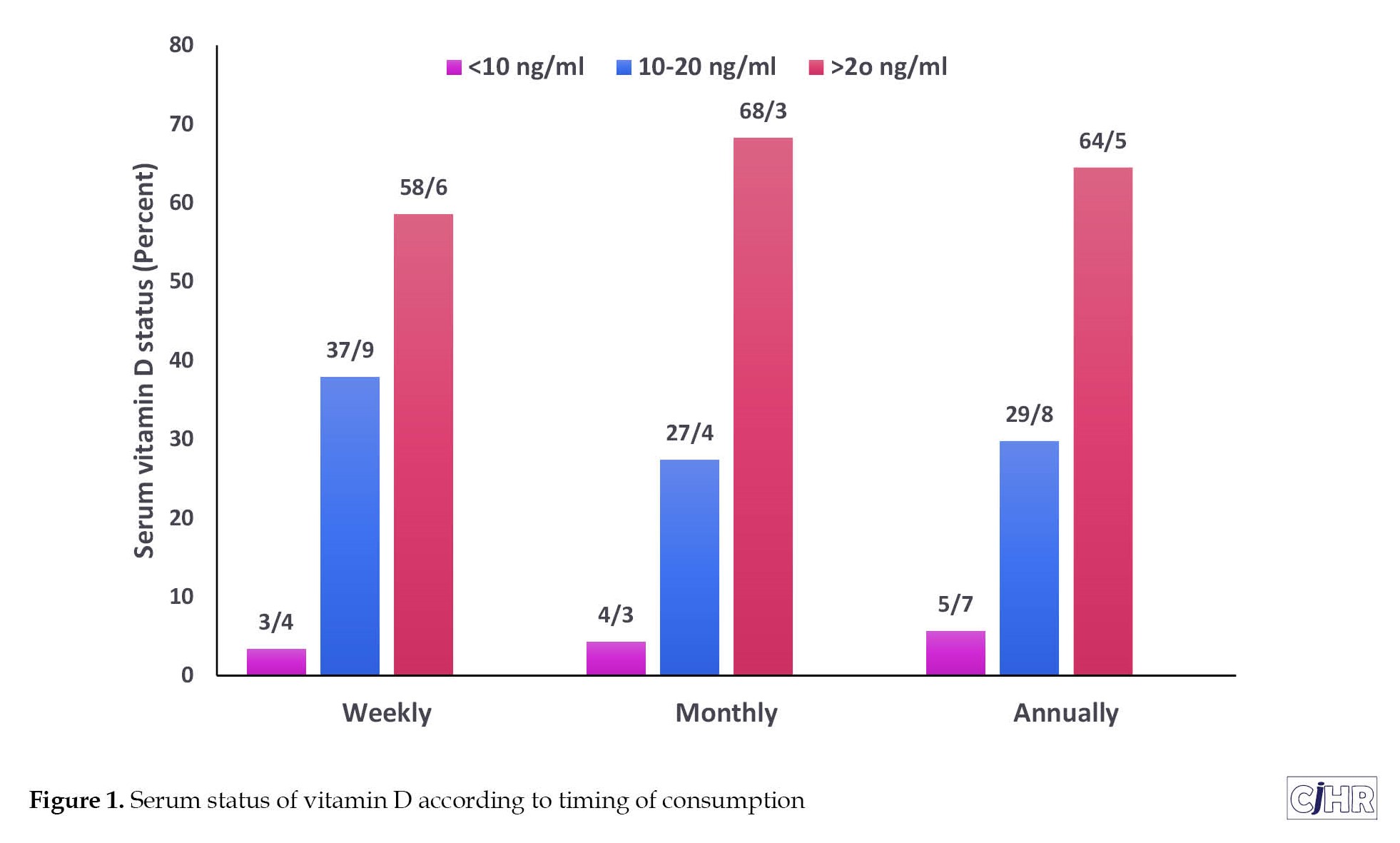
Regarding to the timing of consumption, 34 subjects were weekly (5.5%), 177 subjects were monthly (28.8%) and 401 subjects (65.3%) were annually taking the supplements. There was no significant difference between the timing of consumption and the status of Vitamin D serum level. The highest percentage of vitamin D deficiency (5.7%) was among annual consumers of vitamin D supplementary tablets (50000 IU mega doses) and the lowest percentage was among weekly consumers (3.4%) (P=0.960) (Figure 1).
Vitamin D is a fat-soluble vitamin and a hormone precursor [1] and is known as a very important indicator of health [2]. This vitamin is both a nutrient and a hormone precursor and has many benefits for human health. The health benefits of vitamin D go beyond bone health, as confirmed in various studies. In addition to regulating calcium metabolism, this vitamin also regulates insulin, reduces the risk of diabetes and cancer, produces renin, and helps to eliminate infectious agents and regulate cell growth¸ Strengthens the immune system¸ this vitamin also helps to cure many important diseases [2, 3]. Recently, vitamin D has attracted a great deal of attention around the world, and it has been attributed as a drug of the last decade due to its widespread deficiency in the world [3]. Vitamin D also plays a significant role in human fertility [4]¸and has several effects on pregnancy, maternal and fetal health [5]. Vitamin D is available in two forms: Vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol) [6]. Sources of vitamin D are nutrition, sunlight and supplements [7]. Vitamin D is measured through determination of 25 hydroxyvitamin D3, which is present in the serum. It is biologically neutral and has a half-life of 2-3 weeks [8, 9, 10]. Vitamin D deficiency usually refers to serum levels of 25-hydroxy D3 plasma <50 nmol per liter (20 ng/mL) [11]. The main risk factors for vitamin D deficiency include old age, dark skin pigmentation, and any barrier to the sun’s ultraviolet light reaching the skin, such as full body coverage, spending more time at home, and air pollution [12]. Vitamin D deficiency is a public health concern around the world [13]. Prevention, early diagnosis and treatment of vitamin D deficiency is a key tool to reduce the effects of vitamin D deficiency on the health of the body, especially in the elderly [14]. If left untreated, it can lead to reduced quality of life and increased costs due to a lack of proper attention to this health problem [13].
Vitamin D deficiency has been reported in all over the world [15]. Its prevalence is recorded in all age groups, including toddlers, school children, adult men and women, the elderly, pregnant women, and infants in rural and urban areas [16]. Vitamin D deficiency has affected more than one billion people worldwide [11]. In a review study by Chakhtoura et al¸ in the Middle East and North African region, prevalence of hypovitaminosis D among children and adolescents is 12-96%, in pregnant women, 90 to 54%, and in adults between 96 and 44% with an average of 25 hydroxy D3 between 11 and 20 ng/mL [17]. There is a high prevalence of vitamin D deficiency in Iran in different age groups [18]¸ In a review study by Tabarizi et al, the percentage of vitamin D deficiency in pregnant women was 60.4% and among adult women was 61.9% [4]. Inadequate intake of vitamin D from its main source, which is sunlight, due to the type of clothing worn by women, the presence of many cloudy and rainy days in the year, latitude, lack of exposure to sunlight, and the use of sunscreen creams are possible reasons for the prevalence of deficiency of vitamin D among women in northern Iran [3, 19].The complications of vitamin D deficiency can be prevented by effective preventive measures such as vitamin D supplementation. Therefore¸ a preventive policy¸ including distribution of vitamin D mega dose supplementation was implemented in recent years in Iran (50000 units of vitamin D supplement tablets per month), including in Guilan. But there is lack of awareness about the serum status of vitamin D in women covered by this project in Guilan. So, the aim of this study was to determine the serum levels of vitamin D in women participating supplementation program.
Materials and Methods
This study was conducted to investigate the serum status of vitamin D among women receiving vitamin supplementation participating in the PERSIAN Guilan Cohort study (PGCS). PGCS is a prospective, population-based cohort study in Guilan, the northern province of Iran, recruited between October 8, 2014, and January 20, 2017 [20], as part of the prospective epidemiological research studies in Iran (PERSIAN) [21]. Different districts of the province were chosen to include different socioeconomic status levels including urban areas and 39 villages. The sampling and data collection methods have been previously described in detail [20].
This cross-sectional analytical study was conducted on a subset of PGCS, which aimed to determine the serum level of vitamin D in women recieving vitamin D supplements (50000 IU pearl vitamin D). A total of 614 people (10.9%) out of 5633 eligible women were included. The desired information was collected through interviews from the women referring to the primary health service centers (health centers and comprehensive urban health service centers) in Some’e Sara district, Guilan Province. Demographic and social characteristics including weight, height, body mass index, age, employment status, level of education, marital status, place of residence status, housing area, alcohol consumption, and how to take vitamin D supplement tablets were collected using a data collection form. Weight was measured by a scale with minimal cloths without shoes in kilograms and height in a normal standing position using a tape measure. Body mass index (BMI) was measured as weight in kilogram divided by square of height in meter. BMI of the participants was classified in four categories of underweight (BMI <18.5), normal (BMI between 18.5 and 24.9), overweight (BMI between 25 and 29.9), and obese (BMI >30) [20].
In the second part to assess the serum status of vitamin D, 2 cc of venous blood samples were taken from 563 participants (51 non-participants in the study). Blood samples were collected from all individuals using Vacutainers (Greiner Bio-One International GmbH, Kremsmunster, Austria). Whole blood samples were collected in EDTA (K3) tubes (Becton Dickinson, France). Serum 25(OH)D3 was determined by using a commercially available electrochemiluminescence immunoassay with Roche Elecsys 2010 and Cobas E411 auto analyzer (Roche Diagnostics GmbH, Mannheim, Germany) [22]. Serum levels of vitamin D were then classified into deficient: 25(OH)D3<10, insufficient: 10-20, and sufficient: >20 ng/mL [23].
Data analysis was performed using SPSS statistical software, version 22 (SPSS Inc, Chicago, IL, USA). Descriptive and inferential statistics were also used in data analysis, so that categorical variables were presented as frequency (number) and percentage and quantitative variables as Mean±SD. Participants due to the concentration of 25-hydroxy D3 serum in to 3 categories of deficiency (<10), insufficient (between 10-20) and sufficient (>20 ng/mL) were divided, and the chi-square test was used to compare how to take vitamin D supplements (weekly, monthly, and annually) and individual-social specifications with serum vitamin D levels, and P<0.05 to statistically significant.
Results
Of the 5633 women participating in the cohort study, 614(10.9%) were vitamin D supplement users. The results of this study showed that Mean±SD age of subjects were 50.3±8.7 (ranged 36 to 70) years. Demographic and social characteristics of supplementary consumers showed that 42.8% the subjects were in the age group 40-50 years old, 48.2% were obese, 77.4% of them were unemployed, 29.8% had high school level of education, 88.1% are married, 87.5% have home as a owner, 63% have a residential house with an area of 71 to 116 square meters, 62.2% urban, 99.8% have no alcohol consumption, and 65.3% have an annual consumption Vitamin D supplementary tablets. The majority of participants (65.4%) had sufficient serum levels of vitamin D. The Mean±SD of serum vitamin D was 31.63±15.336 ng/mL (Table 1).
Regarding to the timing of consumption, 34 subjects were weekly (5.5%), 177 subjects were monthly (28.8%) and 401 subjects (65.3%) were annually taking the supplements. There was no significant difference between the timing of consumption and the status of Vitamin D serum level. The highest percentage of vitamin D deficiency (5.7%) was among annual consumers of vitamin D supplementary tablets (50000 IU mega doses) and the lowest percentage was among weekly consumers (3.4%) (P=0.960) (Figure 1).
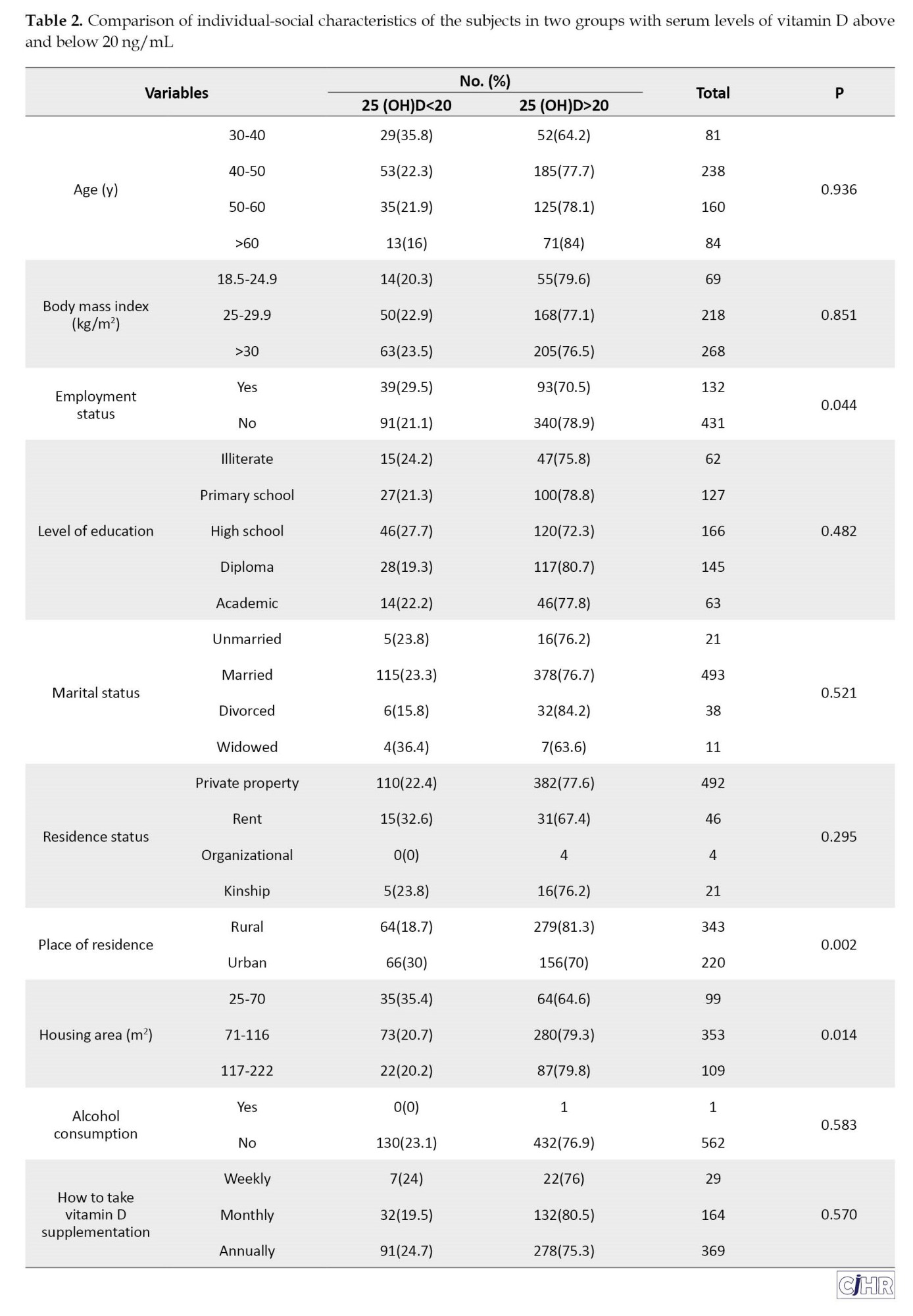
Comparison of demographic characteristics of the subjects in the two groups of subjects with serum levels of vitamin D above and below 20 ng/mL showed a significant association between employment status, place of residence, and housing area with vitamin D level (P<0.05). The employed subject had higher percentage of vitamin D serum level below than 20 ng/mL (29.5%) compared to employed subjects (21.1%). Urban residence and residence in small housing area had higher percentage of low vitamin D (P<0.05) (Table 2).
Discussion
The aim of this study was to determination the serum level of vitamin D in vitamin D supplement consumers among women participating in the Persian Guilan cohort study. The results of this study showed that despite taking vitamin D supplementation in the subjects, one third of them still did not have a sufficient serum level of vitamin D (serum level more than 20 ng/mL). Moderate to severe vitamin D deficiency was reported to be over 45% in different age groups among males and females in some urban areas in Iran [18, 24]. In the research of Mousavi Bahar et al., the prevalence of vitamin D deficiency was 38.73% in Hamedan City [25]. While in the study of Abbasian et al. the prevalence of vitamin D deficiency among pregnant women in Shahroudi was 1.1% [26], the study of Shahabi et al. showed the prevalence of vitamin D deficiency to be 80.96% among women working in Kerman hospital [27]. It seems that factors such as geographical location, humidity above 70% and the climate of Guilan, which has a temperate and often “cloudy and rainy” climate, as well as the clothing and style of clothing worn by women¸ this causes subjects to be deprived of direct sunlight skin contact, and restricting access to fortified foods or not using foods rich in vitamin D is effective in causing this deficiency in the present study.
Kaddam et al. [28] reported a vitamin D deficiency of 44% in their study, as well as 3.2% deficiency in the study of Tangoh et al. [29]¸ 26.5% in the study of Fung et al. [30], 85.7% of deficiency in the study of Binobead et al. [31], and 98.8% of deficiency was reported in the study of Roomi et al. [32]. Since various factors, including environmental and lifestyle factors, as well as demographic factors, determine the concentration of 25 hydroxy D3 serum. Some studies suggest that the rate consumption of vitamin D, sex, outdoor activity, geographical location, season, age and body fat are the main determinants of serum 25-hydroxy D3 concentrations [33, 34]. Therefore, the difference between the results of the present study and other studies can be due to differences in geographical location, age range, sex, sample size, research community, exposure to sunlight, differences in vitamin D cut off and season. According to the results of this study, out of a total of 5633 women participating in the project, only 10.9% of them included 614 subjects taking vitamin D supplements, in terms of how to take the supplement, only 28.8% of them took supplements monthly. In a study by Binobead et al. [31], 20.6% of participants, Fung et al. [30], 75% of women and 40% of men and Darling et al. [35], 39% of women were taking vitamin D supplementation.
In the present study, the prevalence of deficiency in urban areas (30%) was higher than in rural areas. It seems that the results of this study can be due to low level of awareness and knowledge of subjects about vitamin D, less access to supplements, not taking vitamin D supplement, incorrect use of vitamin D supplements (50000 IU of tablets per month), spending most of the time of the day indoor and use any type of coverage to prevent sunlight from reaching the surface of the skin (such as hats, gloves and sun protect cream).
There was no significant association between BMI with serum vitamin D levels in a study by Iqbal et al. [36], in a study by Safarzadeh et al. [37], Joshi & Mandul [38] and Man et al. [39] between age and BMI, Tangoh et al. [29] between marital status and level of education and Binobead et al. [31] between employment status with serum vitamin D levels no found significant association. While in studies by Altowijri et al. [40] and Rabenberg et al. [41] there was a significant relationship between BMI with serum vitamin D levels. In a study by Suryanarayana et al. [42] between level of education and BMI. Binobead et al. [31] between age and BMI with serum vitamin D levels significant relationship was reported. A study by Man et al. [39], found association between alcohol consumption and serum levels of vitamin D. No found significant association between serum vitamin D levels with place of residence and the marital status in the study Altowijri et al. [40].
In a study by Jaaskelainen et al. [43] and Naugler et al. [44], a significant relationship was reported between higher education and high income with increased serum levels of vitamin D. However, in Daly et al.'s study [45], there was no relationship between the level of education and high income with increase in serum levels of vitamin D. Rabenberg et al. [41], also found that socioeconomic status was lower with low serum levels of vitamin D. Differences in the results of the present study with the studied results could be due to differences in age range, community and sample size, geographical location, differences in nutritional, cultural, and lifestyle habits.
Conclusion
The present study revealed that the majority of participants did not follow the correct consumption pattern, one third of people still did not have enough vitamin D levels despite taking supplements, also between employment status, place of residence and housing area were significantly associated with vitamin D levels, while there was no significant association between age, BMI, marital status, alcohol consumption, level of education, and how to take vitamin D supplementation with serum vitamin D levels. Therefore, based on the results obtained, managers and health officials should improve the awareness of subjects in the community on ways to prevent vitamin D deficiency, improve lifestyle, counseling and encourage subjects to take supplements and create the necessary facilities such as sports facilities and enrichment projects of eating foods with vitamin D to improve vitamin D status, reduce the risk of developing deficiency and prevent side effects.
The limitations of this research include the impossibility of identifying women with diseases that interfere with the absorption of vitamin D, the lack of investigating the duration of exposure to sunlight during the day, the type of supplement consumed, and the cross-sectional nature of the research.
Ethical Considerations
Compliance with ethical guidelines
The present study was approved by ethics committee of Guilan University of Medical Sciences (Code: IR.GUMS.REC.1398.276).
Funding
The paper was extracted from the master's thesis of Tayebeh Ramaji, approved by Department of Midwifery, School of Nursing and Midwifery, Guilan University of Medical Sciences. All the data of this study was related to the PERSIAN Guilan cohort study under the supervision of Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Science.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors thank all participants for participating in this study and the personnel of Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Science for supporting this study.
References
Discussion
The aim of this study was to determination the serum level of vitamin D in vitamin D supplement consumers among women participating in the Persian Guilan cohort study. The results of this study showed that despite taking vitamin D supplementation in the subjects, one third of them still did not have a sufficient serum level of vitamin D (serum level more than 20 ng/mL). Moderate to severe vitamin D deficiency was reported to be over 45% in different age groups among males and females in some urban areas in Iran [18, 24]. In the research of Mousavi Bahar et al., the prevalence of vitamin D deficiency was 38.73% in Hamedan City [25]. While in the study of Abbasian et al. the prevalence of vitamin D deficiency among pregnant women in Shahroudi was 1.1% [26], the study of Shahabi et al. showed the prevalence of vitamin D deficiency to be 80.96% among women working in Kerman hospital [27]. It seems that factors such as geographical location, humidity above 70% and the climate of Guilan, which has a temperate and often “cloudy and rainy” climate, as well as the clothing and style of clothing worn by women¸ this causes subjects to be deprived of direct sunlight skin contact, and restricting access to fortified foods or not using foods rich in vitamin D is effective in causing this deficiency in the present study.
Kaddam et al. [28] reported a vitamin D deficiency of 44% in their study, as well as 3.2% deficiency in the study of Tangoh et al. [29]¸ 26.5% in the study of Fung et al. [30], 85.7% of deficiency in the study of Binobead et al. [31], and 98.8% of deficiency was reported in the study of Roomi et al. [32]. Since various factors, including environmental and lifestyle factors, as well as demographic factors, determine the concentration of 25 hydroxy D3 serum. Some studies suggest that the rate consumption of vitamin D, sex, outdoor activity, geographical location, season, age and body fat are the main determinants of serum 25-hydroxy D3 concentrations [33, 34]. Therefore, the difference between the results of the present study and other studies can be due to differences in geographical location, age range, sex, sample size, research community, exposure to sunlight, differences in vitamin D cut off and season. According to the results of this study, out of a total of 5633 women participating in the project, only 10.9% of them included 614 subjects taking vitamin D supplements, in terms of how to take the supplement, only 28.8% of them took supplements monthly. In a study by Binobead et al. [31], 20.6% of participants, Fung et al. [30], 75% of women and 40% of men and Darling et al. [35], 39% of women were taking vitamin D supplementation.
In the present study, the prevalence of deficiency in urban areas (30%) was higher than in rural areas. It seems that the results of this study can be due to low level of awareness and knowledge of subjects about vitamin D, less access to supplements, not taking vitamin D supplement, incorrect use of vitamin D supplements (50000 IU of tablets per month), spending most of the time of the day indoor and use any type of coverage to prevent sunlight from reaching the surface of the skin (such as hats, gloves and sun protect cream).
There was no significant association between BMI with serum vitamin D levels in a study by Iqbal et al. [36], in a study by Safarzadeh et al. [37], Joshi & Mandul [38] and Man et al. [39] between age and BMI, Tangoh et al. [29] between marital status and level of education and Binobead et al. [31] between employment status with serum vitamin D levels no found significant association. While in studies by Altowijri et al. [40] and Rabenberg et al. [41] there was a significant relationship between BMI with serum vitamin D levels. In a study by Suryanarayana et al. [42] between level of education and BMI. Binobead et al. [31] between age and BMI with serum vitamin D levels significant relationship was reported. A study by Man et al. [39], found association between alcohol consumption and serum levels of vitamin D. No found significant association between serum vitamin D levels with place of residence and the marital status in the study Altowijri et al. [40].
In a study by Jaaskelainen et al. [43] and Naugler et al. [44], a significant relationship was reported between higher education and high income with increased serum levels of vitamin D. However, in Daly et al.'s study [45], there was no relationship between the level of education and high income with increase in serum levels of vitamin D. Rabenberg et al. [41], also found that socioeconomic status was lower with low serum levels of vitamin D. Differences in the results of the present study with the studied results could be due to differences in age range, community and sample size, geographical location, differences in nutritional, cultural, and lifestyle habits.
Conclusion
The present study revealed that the majority of participants did not follow the correct consumption pattern, one third of people still did not have enough vitamin D levels despite taking supplements, also between employment status, place of residence and housing area were significantly associated with vitamin D levels, while there was no significant association between age, BMI, marital status, alcohol consumption, level of education, and how to take vitamin D supplementation with serum vitamin D levels. Therefore, based on the results obtained, managers and health officials should improve the awareness of subjects in the community on ways to prevent vitamin D deficiency, improve lifestyle, counseling and encourage subjects to take supplements and create the necessary facilities such as sports facilities and enrichment projects of eating foods with vitamin D to improve vitamin D status, reduce the risk of developing deficiency and prevent side effects.
The limitations of this research include the impossibility of identifying women with diseases that interfere with the absorption of vitamin D, the lack of investigating the duration of exposure to sunlight during the day, the type of supplement consumed, and the cross-sectional nature of the research.
Ethical Considerations
Compliance with ethical guidelines
The present study was approved by ethics committee of Guilan University of Medical Sciences (Code: IR.GUMS.REC.1398.276).
Funding
The paper was extracted from the master's thesis of Tayebeh Ramaji, approved by Department of Midwifery, School of Nursing and Midwifery, Guilan University of Medical Sciences. All the data of this study was related to the PERSIAN Guilan cohort study under the supervision of Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Science.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors thank all participants for participating in this study and the personnel of Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Science for supporting this study.
References
- Maldonado G, Paredes C, Guerrero R, Ríos C. Determination of vitamin D status in a population of Ecuadorian subjects. ScientificWorldJournal. 2017; 2017:3831275.[DOI:10.1155/2017/3831275] [PMID]
- Pfotenhauer KM, Shubrook JH. Vitamin D deficiency, its role in health and disease, and current supplementation recommendations. J Am Osteopath Assoc. 2017; 117(5):301-5. [DOI:10.7556/jaoa.2017.055] [PMID]
- Hossein nezhad A, Holick MF. Vitamin D for health: A global perspective. Mayo Clin Proc. 2013; 88(7):720-55. [DOI:10.1016/j.mayocp.2013.05.011] [PMID]
- Tabrizi R, Moosazadeh M, Akbari M, Dabbaghmanesh MH, Mohamadkhani M, Asemi Z, et al. High prevalence of vitamin D deficiency among Iranian population:A systematic review and meta-analysis. Iran J Med Sci. 2018 ; 43(2):125-39. [PMID]
- Pacifici GM. Effects of vitamin D in neonates and young infants. Int J Pediatr. 2016 ; 4(1):1273-85. [Link]
- Kulie T, Groff A, Redmer J, Hounshell J, Schrager S. Vitamin D: An evidence-based review. J Am Board Fam Med. 2009; 22(6):698-706. [DOI:10.3122/jabfm.2009.06.090037] [PMID]
- Holick MF. Vitamin D deficiency. N Engl J Med. 2007; 357(3):266-81. [DOI:10.1056/NEJMra070553] [PMID]
- Jameson JL, Kasper DL, Hauser SL, Longo DL, Loscalzo J. Harrison’s Principles of Internal Medicine , 20e. New York: McGraw-Hill Medical; 2018. [Link]
- Prusik K, Kortas J, Prusik K, Mieszkowski J, Jaworska J, Skrobot W, et al. Nordic walking training causes a decrease in blood cholesterol in elderly women supplemented with vitamin D. Front Endocrinol (Lausanne). 2018; 9:42. [DOI:10.3389/fendo.2018.00042] [PMID]
- Raymond JL, Morrow K. Krause’s food & the nutrition care process. Amsterdam: Elsevier; 2016. [Link]
- Holick MF, Chen TC. Vitamin D deficiency: A worldwide problem with health onsequences. Am J Clin Nutr. 2008; 87(4):1080S-6S. [DOI:10.1093/ajcn/87.4.1080S] [PMID]
- Munns CF, Shaw N, Kiely M, Specker BL, Thacher TD, Ozono k, et al. Global consensus recommendations on prevention and management of nutritional rickets. Horm Res Paediatr. 2016 ; 85(2):83-106. [DOI:10.1159/000443136] [PMID]
- Aguiar M, Andronis L, Pallan M, Högler W, Frew E. Preventing vitamin D deficiency (VDD): A systematic review of economic evaluations. Eur J Public Health. 2017; 27(2):292-301. [DOI:10.1093/eurpub/ckw270] [PMID]
- Bjelakovic G, Gluud LL, Nikolova D, Whitfield K, Wetterslev J, Simonetti RG, et al. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst Rev. 2014; (1):CD007470. [PMID]
- Palacios C, Gonzalez L. Is vitamin D deficiency a major global public health problem? J Steroid Biochem Mol Biol. 2014; 144 Pt A:138-45. [DOI:10.1016/j.jsbmb.2013.11.003] [PMID]
- Azizi F, Hatami H, Janghorbani M. [Epidemiology and control of common diseases in Iran (Persian). Tehran: Khosravi publication; 2011. [Link]
- Chakhtoura M, Rahme M, Chamoun N, El-Hajj Fuleihan G. Vitamin D in the Middle East and North Africa. Bone Rep. 2018; 8:135-46. [DOI:10.1016/j.bonr.2018.03.004] [PMID]
- Zebhi A, Pakseresht S, Mokhtari N, Mahdevi Roshan M, Kazemnezhad Leyli E, Monfared A. Osteoporosis preventive lifestyle and vitamin D status among nursing students of Guilan University of Medical Sciences. J Holist Nurs Midwifery. 2019; 29(2):113-21. [DOI:10.32598/JHNM.29.2.113]
- Joukar F, Naghipour M, Hassanipour S, Fakhrieh Asl S, Pourshams A, Mansour-Ghanaei F. Vitamin D deficiency associated with reproductive factors in northern Iranian women: The Persian guilan cohort study (PGCS). Clin Nutr ESPEN. 2020; 38:271-6. [DOI:10.1016/j.clnesp.2020.03.022] [PMID]
- Mansour Ghanaei F, Joukar F, Naghipour MR, Sepanlou SG, Poustchi H, Mojtahedi K, et al. The Persian Guilan cohort study (PGCS). Arch Iran Med. 2019; 22(1):39-45. [PMID]
- Poustchi H, Eghtesad S, Kamangar F, Etemadi A, Keshtkar AA, Hekmatdoost A, et al. Prospective epidemiological research studies in Iran (the Persian cohort study): Rationale, objectives, and design. Am J Epidemiol. 2017; 187(4):647-55. [DOI:10.1093/aje/kwx314] [PMID]
- Joukar F, Naghipour M, Hassanipour S, Salari A, Alizadeh A, Saeidi-Saedi H, et al. Association of serum levels of vitamin D with blood pressure status in northern Iranian population: The Persian Guilan Cohort Study (PGCS). Int J Gen Med. 2020; 13:99-104. [DOI:10.2147/IJGM.S244472] [PMID]
- Elmadfa I, Meyer AL, Wottawa D, Wagner K , Hasenegger V. Vitamin D intake and status in Austria and its effects on some health indicators. Austin J Nutr Metab. 2017; 4(2):1050. [Link]
- Sobhani AR, Heidarnzhad Z, Mansour Ghanaei M, Salamt F. Association between vitamin D and gestational diabetes. J of Univ of Med Sci. 2016; 25(98):45-50. Error! Hyperlink reference not valid.
- Mousavi Bahar H, Komaki M, Karimi N, Hamzehei R. [Prevalence of Vitamin D deficiency and its related factors in residents of Hamadan City (Persian)]. Iran J Diabetes Metab. 2018; 18(1):49-54. [Link]
- Abbasian M, Chaman R, Amiri M, Ajami ME, Jafari Koshki T, Rohani H, et al. Vitamin D deficiency in pregnant women and their neonates. Glob J Health Sci. 2016; 8(9):54008.[DOI:10.5539/gjhs.v8n9p83] [PMID]
- Shahabi M, Ghiasi A, Rezazadeh M, Saeidi SJ, Soltani P, Davari M, et al. [Measurement of serum level of vitamin D in staff of a military hospital In order to health promotion of them (Persian)]. J Nurse Physician Whitin War. 2015; 3 (7):53-8. [Link]
- Kaddam IM, Al-Shaikh AM, Abaalkhail BA, Asseri KS, Al-Saleh YM, Al-Qarni AA, et al. Prevalence of vitamin D deficiency and its associated factors in three regions of Saudi Arabia. Saudi Med J. 2017; 38(4):381-90. [DOI:10.15537/smj.2017.4.18753] [PMID]
- Tangoh DA, Apinjoh TO, Mahmood Y, Nyingchu RV, Tangunyi BA, Nji EN, et al. Vitamin D status and its associated risk factors among adults in the Southwest Region of Cameroon. J Nutr Metab. 2018; 2018:4742574. [DOI:10.1155/2018/4742574] [PMID]
- Fung JL, Hartman TJ, Schleicher RL, Goldman MB. Association of vitamin D intake and serum levels with fertility: Results from the lifestyle and fertility study. Fertil Steril. 2017; 108(2):302-11. [DOI:10.1016/j.fertnstert.2017.05.037] [PMID]
- Binobead MA, Al-Qahtani WH, Al Bader NA, AlSedairy SA, Arzoo S. Prevalence of vitamin D deficiency and the effect of anthropometric and lifestyle factors on thevitamin D statuses of healthy women residing in Riyadh. Prog Nutr. 2019; 21(2):299-308. [Link]
- Roomi MA, Farooq A, Ullah E, Lone KP. Hypovitaminosis D and its association with lifestyle factors. Pak J Med Sci. 2015; 31(5):1236-40. [DOI:10.12669/pjms.315.7196] [PMID]
- Mithal A, Wahl DA, Bonjour JP, Burckhadt P, Dawson Hughes J, Eisman A, et al. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos Int. 2009; 20(11):1807-20. [DOI:10.1007/s00198-009-0954-6] [PMID]
- Mai XM, Chen Y, Camargo CA Jr, Langhammer A. Crosssectional and prospective cohort study of serum 25-hydroxyvitamin D level and obesity in adults: The HUNT study. Am J Epidemiol. 2012; 175(10):1029-36. [DOI:10.1093/aje/kwr456] [PMID]
- Darling AL, Blackbourn DJ, Ahmadi KA, Lanham New SA. Vitamin D supplement use and associated demographic, dietary and lifestyle factors in South Asians (n 8024) aged 40-69 years: Analysis of the UK Biobank Cohort. Public Health Nutr. 2018; 21(14):2678-88. [DOI:10.1017/S1368980018001404] [PMID]
- Iqbal K, Islam N, Mehboobali N, Asghar A, Iqbal SP, Iqbal MP. Relationship of sociodemographic factors with serum levels of vitamin D in a healthy population of Pakistan. Pak J Pharm Sci. 2019; 32(1):29-33. [PMID]
- Safarzadeh A, Esfahani MP, Yekta AH, Salehi S, Hassabi M. Determination of effect of oral vitamin D to improve ventilatory threshold in healthy young adults with vitamin D deficiency. Novel Biomed. 2019; 7(1):17-23. [Link]
- Joshi VS, Mandul R. Vitamin D status in medical students and risk factor analysis. Ann Med Physiol. 2018; 2(1):11-6. [DOI:10.23921/amp.2018v2i1.289803]
- Man RE, Li LJ, Cheng CY, Wong TY, Lamoureux E, Sabanayagam C. Prevalence and determinants of suboptimal vitamin d levels in a multiethnic Asian population. Nutrients. 2017; 9(3):313. [DOI:10.3390/nu9030313] [PMID]
- Altowijri A, Alloubani A, Abdulhafiz I, Saleh A. Impact of nutritional and environmental factors on vitamin D deficiency. Asian Pac J Cancer Prev. 2018; 19(9):2569-2574. [PMID]
- Rabenberg M, Scheidt-Nave C, Busch MA, Rieckmann N, Hintzpeter B, Mensink GB. Vitamin D status among adults in Germany - results from the German health interview and examination survey for adults (DEGS1). BMC Public Health. 2015; 15:641. [DOI:10.1186/s12889-015-2016-7] [PMID]
- Suryanarayana P, Arlappa N, Sai Santhosh V, Balakrishna N, Lakshmi Rajkumar P, Prasad U, et al. Prevalence of vitamin D deficiency and its associated factors among the urban elderly population in Hyderabad metropolitan city, South India. Ann Hum Biol. 2018; 45(2):133-9. [DOI:10.1080/03014460.2018.1425479] [PMID]
- Jaaskelainen T, Knekt P, Marniemi J, Sares-Jaske L, Mannisto S, Heliovaara M, et al. Vitamin D status is associated with sociodemographic factors, lifestyle and metabolic health. Eur J Clin Nutr. 2013; 52(2):513-25. [DOI:10.1007/s00394-012-0354-0] [PMID]
- Naugler C, Zhang J, Henne D, Woods P, Hemmelgarn BR. Association of vitamin D status with socio-demographic factors in Calgary, Alberta: An ecological study using census Canada data. BMC Public Health. 2013; 13:316. [DOI:10.1186/1471-2458-13-316] [PMID]
- Daly RM, Gagnon C, Lu ZX, Magliano DJ, Dunstan DW, Sikaris KA, et al. Prevalence of vitamin D deficiency and its determinants in Australian adults aged 25 years and older: A national, population-based study. Clin Endocrinol (Oxf). 2012; 77(1):26-35. [DOI:10.1111/j.1365-2265.2011.04320.x] [PMID]
Article Type: Original Contributions |
Subject:
Epidemiology
Received: 2023/10/8 | Accepted: 2023/12/18 | Published: 2024/01/1
Received: 2023/10/8 | Accepted: 2023/12/18 | Published: 2024/01/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Contact Information
cjhr Office, Guilan University of Medical Sciences
P.O.Box 93345-41938, Rasht, Iran
Journal Tel: +9813 33335820
Publisher Tel: +9821 453 55 000
Email: cjhr.gums@gmail.com
