

Volume 9, Issue 2 (4-2024)
CJHR 2024, 9(2): 75-84 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bagheri Sheykhangafshe F, Savabi Niri V, Zolfagharnia M, Bourbour Z, Esrfilian F. Acceptance and Commitment Therapy on Psychological Distress, Alexithymia, and Spiritual Health in Cardiovascular Disease. CJHR 2024; 9 (2) :75-84
URL: http://cjhr.gums.ac.ir/article-1-342-en.html
URL: http://cjhr.gums.ac.ir/article-1-342-en.html
Farzin Bagheri Sheykhangafshe1 

 , Vahid Savabi Niri2 , Maryam Zolfagharnia3 , Zeynab Bourbour4 , Forough Esrfilian *5
, Vahid Savabi Niri2 , Maryam Zolfagharnia3 , Zeynab Bourbour4 , Forough Esrfilian *5
, Vahid Savabi Niri2 , Maryam Zolfagharnia3 , Zeynab Bourbour4 , Forough Esrfilian *5
1- Department of Psychology, Faculty of Humanities, Tarbiat Modares University, Tehran, Iran
2- Department of Clinical Psychology, Faculty of Humanities, Ardabil Branch, Islamic Azad University, Ardabil, Iran
3- Department of Psychology, Faculty of Humanities, Ardabil Branch, Payame Noor University, Ardabil, Iran
4- Department of Clinical Psychology, Faculty of Humanities, Garmsar Branch, Islamic Azad University, Semnan, Iran
5- Department of Psychology, Faculty of Humanities, Tarbiat Modares University, Tehran, Iran ,esrafilian.fo@gmail.com
2- Department of Clinical Psychology, Faculty of Humanities, Ardabil Branch, Islamic Azad University, Ardabil, Iran
3- Department of Psychology, Faculty of Humanities, Ardabil Branch, Payame Noor University, Ardabil, Iran
4- Department of Clinical Psychology, Faculty of Humanities, Garmsar Branch, Islamic Azad University, Semnan, Iran
5- Department of Psychology, Faculty of Humanities, Tarbiat Modares University, Tehran, Iran ,
Keywords: Acceptance and Commitment Therapy, Psychological Distress, Alexithymia, Spiritual Health, Cardiovascular Disease
Full-Text [PDF 603 kb]
(576 Downloads)
| Abstract (HTML) (1128 Views)
Full-Text: (677 Views)
Introduction
Cardiovascular disease (CVD) is a notable health concern for women, often underestimated and historically believed to be associated with male gender [1]. However, it’s important to recognize that CVD affects women significantly, sometimes even more, and can exhibit distinct manifestations in females [2]. The prevalence of CVD varies by region and is influenced by factors like lifestyle choices, healthcare access, genetics, and socioeconomic status [3]. A study by Townsend et al. [4] highlighted a considerable occurrence of CVD in Europe, emerging as the primary cause of death for individuals under 70. In Iran, a review by Sarrafzadegan et al. [5] found that CVD was responsible for 46% of deaths and 23% of disease burden in the past four decades.
In CVD, anxiety, depression, and stress are among the psychological factors that may play a role in the occurrence or exacerbation of the disease. Psychological factors like anxiety, depression, and stress play a role in CVD, potentially triggering or exacerbating the condition [3]. Psychological distress encompasses negative emotions such as anxiety, depression, chronic stress, and mental suffering [6]. This distress can impact CVD development and progression, while CVD can reciprocally lead to psychological issues [7]. Unhealthy coping mechanisms, like overeating, smoking, sedentary behavior, and excessive alcohol consumption, can arise from psychological distress [8]. These behaviors contribute to CVD risk factors such as obesity, hypertension, and high cholesterol [9]. Research by Pimple et al. [10] revealed a strong link between psychological distress and CVD in women. Another study by Bouchard et al. [11] found that psychological distress and limited social support exacerbate CVD symptoms.
Emotions can have a significant impact on CVD, both in terms of its development and management. Suppressing and ignoring the emotions that exist in alexithymia can cause a late diagnosis of CVD. Alexithymia involves difficulties in recognizing, articulating, and managing one’s emotions [12]. Individuals with alexithymia struggle to understand and express feelings, having limited emotional awareness [13]. Research suggests a link between alexithymia and CVD, implying its role in heart-related conditions [14]. Alexithymia may hinder recognizing physical CVD symptoms like chest pain [15]. Aluja et al.’s study [16] highlighted a strong correlation between alexithymia and CVD, leading to poor treatment adherence. Similarly, Wiernik et al. [17] found elevated alexithymia linked to lower quality of life and mental well-being, increasing susceptibility to CVD risk.
Having meaning in life can reduce the symptoms of illness and pain. The relationship between CVD and spiritual health is intricate and captivating. Spiritual health encompasses a sense of connection to something beyond oneself, finding purpose and meaning in life [18]. This multifaceted concept includes religious beliefs, practices, and a broader sense of spirituality apart from organized religion [19]. Spirituality and religion offer coping mechanisms to handle stress and challenges [20]. Religious activities like prayer or meditation can lower stress, a significant CVD risk factor, thereby promoting better heart health [21]. Brewer et al. [22] found that high spiritual levels correlate with healthier lifestyles, reduced fast-food and cigarette consumption, and fewer CVD instances. Similarly, von Flach et al. [23] discovered that spiritual health mitigates psychological issues and CVD risk. It’s important to note that the impact of spiritual health on CVD can vary greatly from person to person. Not everyone is religious or spiritual, and individuals may have different belief systems. The key is that spiritual health, in whatever form it takes, can be a source of strength and support for individuals facing CVD. Healthcare providers should be sensitive to their patients’ spiritual beliefs and consider the role of spirituality in their overall well-being and health management [19].
Pharmaceutical and medical treatments can be effective to some extent, but after some time having mental health and accepting the disease is of great importance. Recent research has started examining the role of acceptance and commitment therapy (ACT) for women with CVD [24], recognizing their unique challenges influenced by physical and psychosocial factors [25]. ACT is a psychotherapy approach that promotes psychological flexibility by helping individuals accept difficult emotions and thoughts and aligning actions with values and goals [26]. Utilizing mindfulness, acceptance strategies, and behavioral changes [27], ACT’s emphasis on acceptance and mindfulness makes it suitable for addressing psychological factors in women with CVD [28]. ACT interventions have shown promise in reducing psychological distress among women with CVD, enabling them to better manage emotional burdens [29]. Rashidi et al. [30], Sheibani et al. [31], and Zhang et al. [32] collectively highlight ACT’s efficacy in improving psychological and spiritual well-being among individuals with CVD.
The importance of mental health in women with CVD is multifaceted. It encompasses risk reduction, early intervention, treatment adherence, improved quality of life, and overall better cardiovascular outcomes. A holistic approach to women’s cardiovascular care should include a focus on mental health, emphasizing the need for screening, assessment, and intervention for mental health concerns alongside traditional medical management. This integrated approach can lead to more effective care and a higher quality of life for women living with CVD. Psychological treatments are an integral part of the comprehensive care provided to patients with CVD. They can help manage stress, anxiety, depression, and other emotional factors, facilitate behavior change, and improve overall well-being, all of which can contribute to better cardiovascular outcomes and a higher quality of life for these patients. Healthcare providers must consider the psychological aspects of CVD and integrate psychological interventions into the overall treatment plan for these patients. The present study was conducted with the aim of the effectiveness of ACT on psychological distress, alexithymia, and spiritual health of women with CVD.
Materials and Methods
The research design employed in this study was a randomized controlled clinical trial, utilizing a pre-test-post-test design supplemented with a control group. The statistical population under study consisted of women with CVD residing in the 6th district of Tehran during August and September the year 2021. After preparing a list of 30 patients (who had been diagnosed with CVD by a cardiologist), the researchers assigned 15 patients to the experimental and control groups by lottery. The determination of the sample size for this study was predicated upon earlier research and aligned with the parameters set forth by the G*Power software, version 3.1.9.7 (effect size=1.53, 1−β=0.97, and α=0.05) [33]. The inclusion criteria for participation in the study encompassed factors such as personal contentment, age range between 25 and 50 years (the disease is not due to old age), literacy for reading and writing, and the absence of psychiatric medication usage. Conversely, participants were excluded from the study if they failed to respond to questionnaire items, experienced an escalation in pain intensity, or missed more than two therapy sessions.
ACT
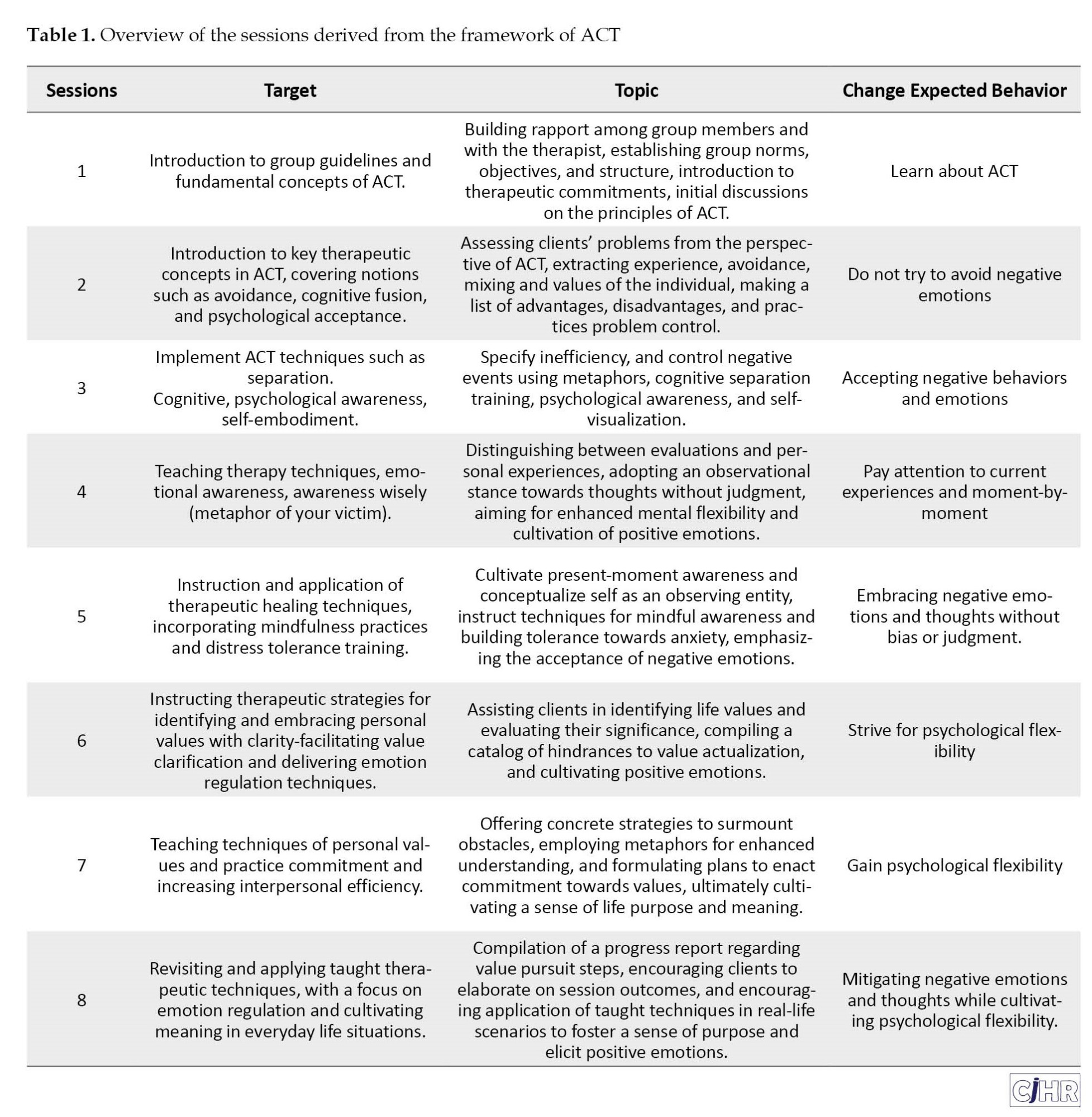
To select patients with CVD, two hospitals were referred. These individuals sought medical treatment for their condition at hospitals within the 6th district of Tehran (Gandhi and Mustafa Khomeini). Following the acquisition of consent from clinic authorities and patients, a total of 30 women diagnosed with CVD by their cardiologists were assigned to the intervention and control groups. The research questionnaires were completed by members of both groups in the form of a pre-test. Due to the unfavorable conditions of the disease, it was tried to collect the pre-test scores in person and online (questionnaire link in Google form). ACT sessions by a therapist specializing in chronic diseases in the psychology clinic were then performed in eight 90-minute weekly group sessions for the experimental group, while the control group did not receive any intervention. To prevent the exchange of information between the members of the groups, they were asked not to discuss the content of the meetings with each other. For this reason, there was no dropout in the groups. ACT was designed based on the ACT programs proposed by Hayes et al. [34] and also taking into account the key characteristics in the design of ACT programs (Table 1).
To comply with ethical principles, after collecting the post-test, treatment sessions were also held for the control group.
Measurement tools
Psychological distress scale (DASS-42)
The concise version of the DASS-42, grouped into three subscales: Depression, anxiety, and stress [35]. Each subscale has 14 questions, rated on a Likert scale of zero to three. Participants assess the extent of their experience of each condition over the past week, using a 4-point intensity/frequency scale. Scores for each subscale range from 0 to 42, where higher scores indicate greater psychological distress [34]. In the Iranian context, Cronbach’s α coefficients for anxiety, depression, and stress are 0.85, 0.90, and 0.82, respectively [36]. In the present study, the content validity index (CVI) and content validity ratio index (CVR) were used to measure the content validity of the questionnaire. The CVI and CVR of the questionnaire were 0.83 and 0.87, respectively, which show the validity of the desired content of the DASS-42. Also, Cronbach’s α coefficients for anxiety (0.86), depression (0.84), and stress (0.81) subscales showed reliable consistency.
Toronto alexithymia scale (TAS-20)
The 20-item alexithymia scale, developed by Bagby et al. [37] includes three subscales: Difficulty identifying feelings, difficulty describing feelings, and externally oriented thinking. Responses are assessed on a five-point Likert scale, ranging from 1 (completely disagree) to 5 (completely agree). Scores range from 20 to 100. Bagby et al. [37] established reliability with Cronbach’s α of 0.81 and test re-test reliability of 0.77. In Iran, Cronbach’s α ranged from 0.71 to 0.83, and test re-test reliability from 0.61 to 0.69 [38]. In the present study, the CVI and CVR were used to measure the content validity of the questionnaire. The CVI and CVR of the questionnaire were 0.89 and 0.81, respectively, which show the validity of the desired content of the DASS-42. Also, Cronbach’s α for subscales were 0.81, 0.86, and 0.84, indicating good internal consistency.
Spiritual health questionnaire (SHQ)
The SHQ was developed by Bufford et al. [39] and comprises 10 items with even numbers assessing existential health, and 10 items with odd numbers evaluating religious health. The combined spiritual health score, ranging from 20 to 120, results from both subsets’ cumulative scores. Respondents’ answers follow a six-point Likert scale. Bufford et al. [39] established the scale’s validity and reliability at 0.86 and 0.91, respectively, among students. In Iran, the questionnaire exhibited a Cronbach’s α coefficient of 0.85 [40]. In the present study, the CVI and CVR were used to measure the content validity of the questionnaire. The CVI and CVR of the questionnaire were 0.84 and 0.83, respectively, which show the validity of the desired content of the DASS-42. Also, internal consistency was strong, with Cronbach’s α coefficients of 0.89 for existential health and 0.84 for religious health.
Statistical analyses
To analyze the research data, descriptive statistics including Mean±SD and covariance analysis were used based on their assumptions with the help of SPSS software, version 24. The significance level of these tests was considered 0.05. The Shapiro-Wilk test results were reported to check the normality of the distribution of variables in the two groups. According to the results, normal distribution was met for all variables. The study used multivariate analysis of covariance to assess the effectiveness of ACT on psychological distress, alexithymia, and spiritual health in women with CVD. The researchers tested various assumptions about the equality of variance, covariance matrix, and regression coefficients. The results indicated that these assumptions were valid.
Results
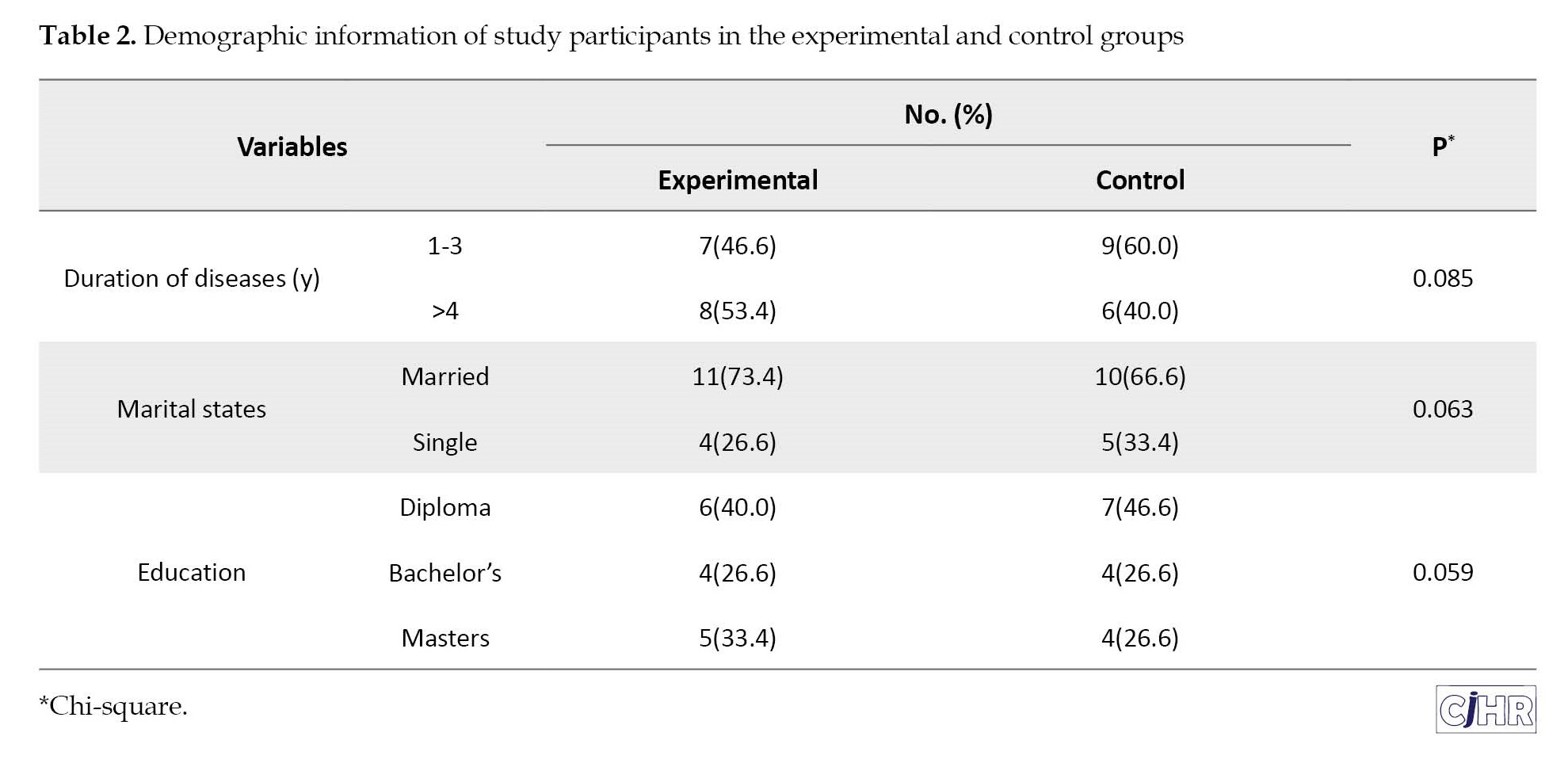
The Mean±SD of the age of the experimental and control groups were 49.12±5.27 and 48.74±4.86, respectively. As displayed in Table 2, highlights no statistically significant differences between the two groups in terms of demographic variables.
The Mean±SD of pre-test-post-test scores of psychological distress, alexithymia, and spiritual health in patients with CVD in the experimental and control groups are presented in Table 3.
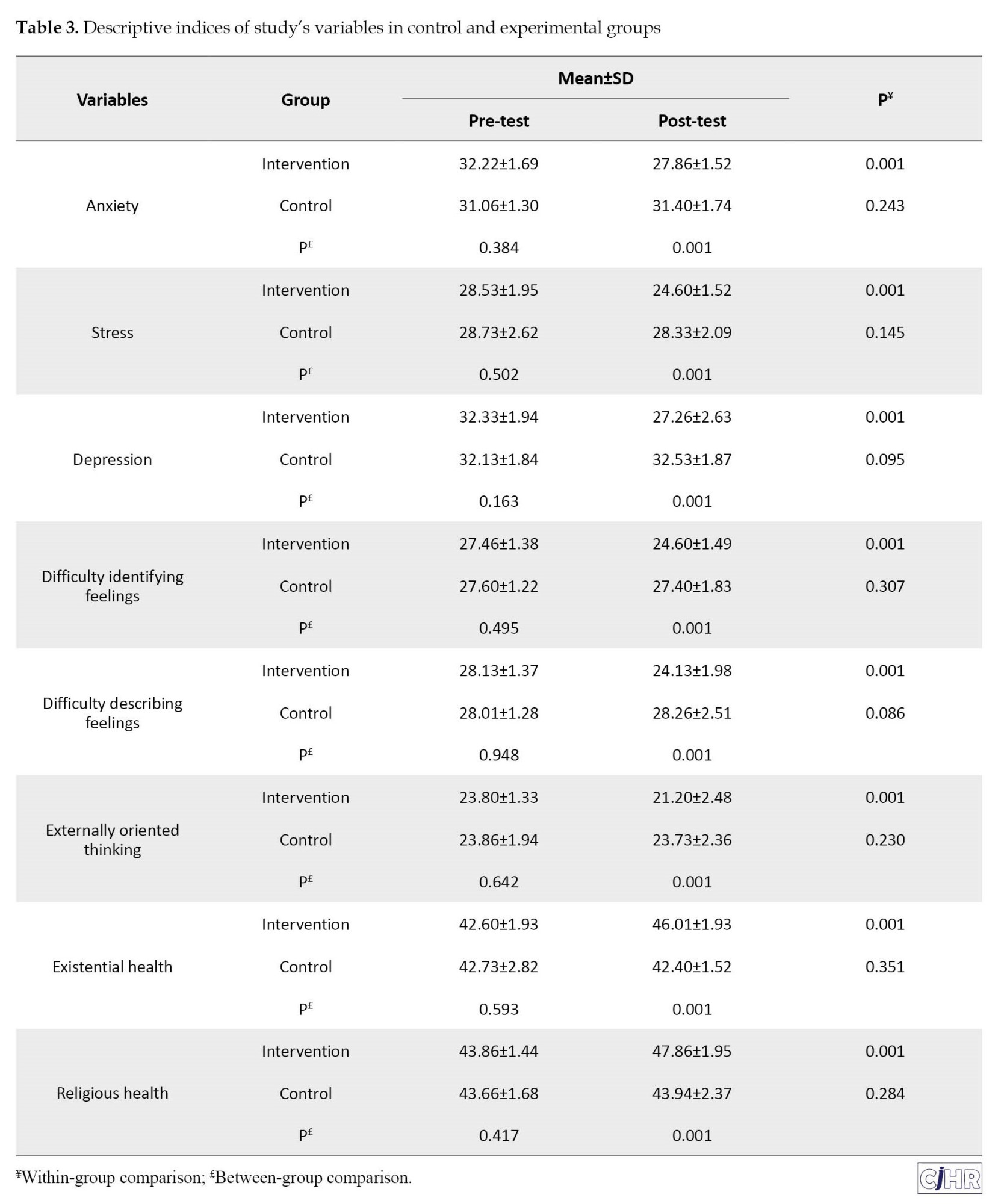
According to Table 3, there was a significant difference in the pre-test scores of the two experimental and control groups.
The results of the Levin test to examine the homogeneity of variance of dependent variables in groups showed that the variance of psychological distress (F=2.615, P=0.117), alexithymia (F=1.50, P=0.231), and spiritual health (F=1.37, P=0.251) were equal in the groups. The results of the Box test to evaluate the equality of the covariance matrix of dependent variables between the experimental and control groups also showed that the covariance matrix of the dependent variables is equal (box M=55.43, F=1.06, P=0.377). Also, the results of the chi-square-Bartlett test to examine the sphericity or significance of the relationship between psychological distress, alexithymia, and spiritual health showed that the relationship between them is significant (χ2=140.88, df=35, P<0.05). The homogeneity of regression coefficients was examined through the interaction of dependent variables and independent variables (intervention method) in the pre-test and post-test. The interaction of these pre-tests and post-tests with the independent variable was not significant and indicated the homogeneity of the regression slope. Therefore, all assumptions of multivariate analysis of covariance were met. Table 4 shows the results of multivariate analysis of covariance for comparison between the two groups.
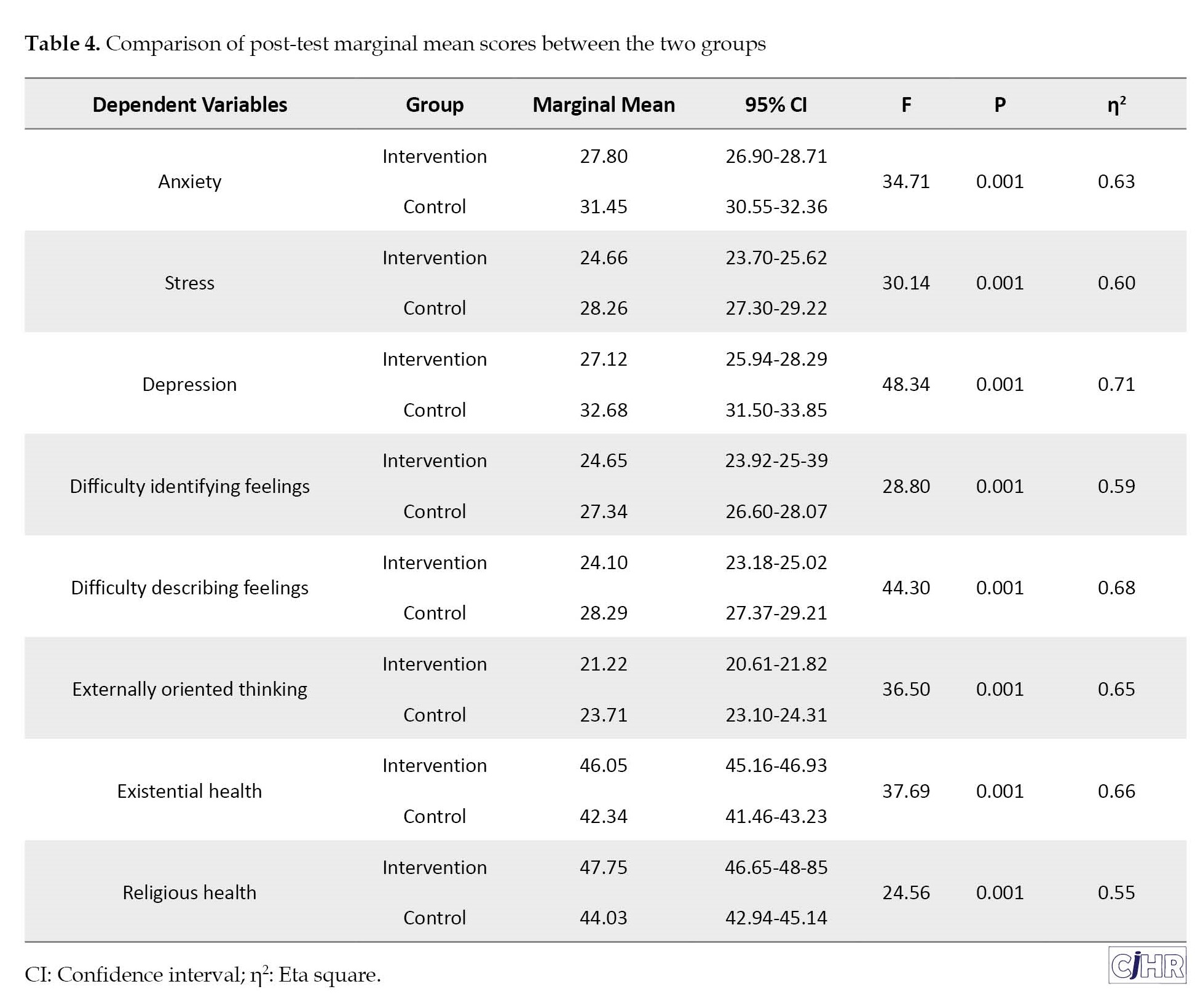
The marginal post-test score adjusted for baseline covariate showed that there was a significant difference between the two groups in terms of anxiety (F=34.71), stress (F=30.14), depression (F=48.34), difficulty identifying feelings (F=28.80), difficulty describing feelings (F=44.30), externally oriented thinking (F=36.50), existential health (F=37.69), and religious health (F=24.56) at the level of 0.001. These findings indicate that there is a significant difference between the groups in these variables.
Discussion
The present study was conducted with the aim of the effectiveness of ACT on psychological distress, alexithymia, and spiritual health of women with CVD. The results of the present study showed that women with CVD had less anxiety, depression, and stress after receiving treatment based on ACT. These findings are in line with the research of Dar et al. [8]; Osborne et al. [9]; Pimple et al. [10] and Bouchard et al. [11].
ACT can be beneficial in improving psychological well-being and reducing symptoms of anxiety, depression, and stress in various populations, including those with chronic health conditions [30]. In the case of women with CVD, ACT might have been used as an adjunct to traditional medical treatment to address their mental health concerns. The stress and emotional burden associated with a CVD diagnosis can significantly impact a person’s overall well-being [24]. By promoting acceptance, mindfulness, and value-driven actions, ACT equips women with the necessary tools to enhance their emotional well-being and overall quality of life. While medical interventions remain crucial, addressing the psychological aspects of CVD is equally vital for providing comprehensive care to women facing this challenging health condition [31]. The results of Dar et al. [8] determined that people who have high levels of psychological distress are at risk of CVD. On the other hand, the findings of a review study by Osborne et al. [9] showed that stress, anxiety, and depression are among the aggravating factors in the onset and increase of CVD levels.
The findings of the present study showed that women with CVD had less difficulty identifying feelings, difficulty describing feelings, and externally oriented thinking after receiving ACT. These findings are in line with studies by Maqbool et al. [14]; Lazarević et al. [15]; Aluja et al. [16] and Wiernik et al. [17].
ACT can be a useful therapeutic approach for individuals struggling with alexithymia. By promoting acceptance of emotions and thoughts without judgment, individuals with alexithymia can begin to develop a greater understanding and awareness of their emotions [14]. Mindfulness practices in ACT can help individuals become more attuned to their bodily sensations and emotional experiences, which can be beneficial for those with alexithymia, as they might find it challenging to identify emotions based solely on cognitive appraisal [26]. The values clarification and committed action aspects of ACT can help individuals with alexithymia align their behaviors with their deeper values, even if they struggle to connect with their emotions directly [30]. The study’s findings underscore the significant impact of ACT in reducing alexithymia among women with CVD. By addressing this often-overlooked emotional factor, healthcare providers can contribute to improved patient outcomes, enhanced emotional well-being, and better quality of life for women living with cardiovascular conditions [25]. The results of Maqbool et al. [14] revealed that a significant number of patients with CVD have high levels of alexithymia, which causes them to not pursue treatment. On the other hand, the findings of Lazarević et al. [15] study indicated a significant positive correlation between alexithymia and CVD. In the meantime, people who had problems recognizing their emotions were indifferent to their illness and did not make efforts to increase their quality of life and mental health.
The results of the present study showed that women with CVD had higher existential and religious health after receiving ACT. These findings are in line with the research of Aryafard et al. [20]; Heshmati et al. [21]; Brewer et al. [22] and von Flach et al. [23].
The journey with CVD can evoke existential questions and prompt a search for meaning and purpose, making spiritual health vital for overall well-being. ACT’s emphasis on values and committed action aligns with many spiritual principles, encouraging women to connect with their spiritual beliefs and integrate them into their lives [24]. As women identify and live in alignment with their spiritual values, they may experience greater spiritual growth and a deeper sense of purpose [31]. Spirituality is a deeply personal and transformative aspect of human existence, encompassing the search for meaning, purpose, and connection to something greater than oneself. Many individuals find solace, guidance, and a sense of fulfillment in their spiritual beliefs and practices [27]. In recent years, mental health professionals have recognized the significance of integrating spirituality into therapy to support individuals on their journey toward holistic well-being [29]. Both ACT and spirituality recognize the impermanent and uncertain nature of life. Through ACT’s focus on values and mindfulness, individuals can develop resilience and cope with difficult emotions and challenging life circumstances. This can lead to a more profound acceptance of uncertainty, fostering a sense of surrender and trust in one’s spiritual journey [28]. The results of a review study by Aryafard et al. [20] determined that the spiritual health of Iranian patients with CVD is average, which requires further improvement. On the other hand, the findings of Heshmati et al. [21] indicated a significant correlation between hope, optimism, and spiritual well-being. Patients with high levels of spirituality were less likely to have severe vascular disease.
The impossibility of controlling the social, educational, and economic status of the research participants was one of the limitations of the research. Therefore, it is suggested that in future research, efforts should be made to control these components. Also, due to the conditions of the COVID-19 epidemic, a small sample size was selected, and it is suggested that more patients be investigated in future studies. The impossibility of long-term follow-up of the impact of the program using a follow-up test was another limitation. Based on this, it is suggested that this issue be taken into consideration in future research so that it is possible to examine the long-term impact of ACT.
Conclusion
ACT offers promising prospects in improving the psychological, emotional, and spiritual health of women living with CVD. By promoting acceptance, emotional awareness, and committed action, ACT empowers women to cope effectively with psychological distress, address alexithymia, and nurture their spiritual well-being. As a holistic therapeutic approach, ACT acknowledges the interconnectedness of these dimensions, allowing women to find strength, purpose, and resilience as they navigate the challenges of living with CVD. As further research unfolds, the potential of ACT in enhancing the overall well-being of women with CVD remains an essential focus for clinicians and researchers alike.
Ethical Considerations
Compliance with ethical guidelines
The present study was approved by Ethics Committee of Baqiyatallah University of Medical Sciences (Code: IR.BMSU.BAQ.REC.1399.011).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Farzin Bagheri Sheykhangafshe and Vahid Savabi Niri; Methodology: Maryam Zolfagharnia, Zeynab Bourbour and Forough Esrfilian; Investigation: Farzin Bagheri Sheykhangafshe and Vahid Savabi Niri; Writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank all the participants in this research.
References
Cardiovascular disease (CVD) is a notable health concern for women, often underestimated and historically believed to be associated with male gender [1]. However, it’s important to recognize that CVD affects women significantly, sometimes even more, and can exhibit distinct manifestations in females [2]. The prevalence of CVD varies by region and is influenced by factors like lifestyle choices, healthcare access, genetics, and socioeconomic status [3]. A study by Townsend et al. [4] highlighted a considerable occurrence of CVD in Europe, emerging as the primary cause of death for individuals under 70. In Iran, a review by Sarrafzadegan et al. [5] found that CVD was responsible for 46% of deaths and 23% of disease burden in the past four decades.
In CVD, anxiety, depression, and stress are among the psychological factors that may play a role in the occurrence or exacerbation of the disease. Psychological factors like anxiety, depression, and stress play a role in CVD, potentially triggering or exacerbating the condition [3]. Psychological distress encompasses negative emotions such as anxiety, depression, chronic stress, and mental suffering [6]. This distress can impact CVD development and progression, while CVD can reciprocally lead to psychological issues [7]. Unhealthy coping mechanisms, like overeating, smoking, sedentary behavior, and excessive alcohol consumption, can arise from psychological distress [8]. These behaviors contribute to CVD risk factors such as obesity, hypertension, and high cholesterol [9]. Research by Pimple et al. [10] revealed a strong link between psychological distress and CVD in women. Another study by Bouchard et al. [11] found that psychological distress and limited social support exacerbate CVD symptoms.
Emotions can have a significant impact on CVD, both in terms of its development and management. Suppressing and ignoring the emotions that exist in alexithymia can cause a late diagnosis of CVD. Alexithymia involves difficulties in recognizing, articulating, and managing one’s emotions [12]. Individuals with alexithymia struggle to understand and express feelings, having limited emotional awareness [13]. Research suggests a link between alexithymia and CVD, implying its role in heart-related conditions [14]. Alexithymia may hinder recognizing physical CVD symptoms like chest pain [15]. Aluja et al.’s study [16] highlighted a strong correlation between alexithymia and CVD, leading to poor treatment adherence. Similarly, Wiernik et al. [17] found elevated alexithymia linked to lower quality of life and mental well-being, increasing susceptibility to CVD risk.
Having meaning in life can reduce the symptoms of illness and pain. The relationship between CVD and spiritual health is intricate and captivating. Spiritual health encompasses a sense of connection to something beyond oneself, finding purpose and meaning in life [18]. This multifaceted concept includes religious beliefs, practices, and a broader sense of spirituality apart from organized religion [19]. Spirituality and religion offer coping mechanisms to handle stress and challenges [20]. Religious activities like prayer or meditation can lower stress, a significant CVD risk factor, thereby promoting better heart health [21]. Brewer et al. [22] found that high spiritual levels correlate with healthier lifestyles, reduced fast-food and cigarette consumption, and fewer CVD instances. Similarly, von Flach et al. [23] discovered that spiritual health mitigates psychological issues and CVD risk. It’s important to note that the impact of spiritual health on CVD can vary greatly from person to person. Not everyone is religious or spiritual, and individuals may have different belief systems. The key is that spiritual health, in whatever form it takes, can be a source of strength and support for individuals facing CVD. Healthcare providers should be sensitive to their patients’ spiritual beliefs and consider the role of spirituality in their overall well-being and health management [19].
Pharmaceutical and medical treatments can be effective to some extent, but after some time having mental health and accepting the disease is of great importance. Recent research has started examining the role of acceptance and commitment therapy (ACT) for women with CVD [24], recognizing their unique challenges influenced by physical and psychosocial factors [25]. ACT is a psychotherapy approach that promotes psychological flexibility by helping individuals accept difficult emotions and thoughts and aligning actions with values and goals [26]. Utilizing mindfulness, acceptance strategies, and behavioral changes [27], ACT’s emphasis on acceptance and mindfulness makes it suitable for addressing psychological factors in women with CVD [28]. ACT interventions have shown promise in reducing psychological distress among women with CVD, enabling them to better manage emotional burdens [29]. Rashidi et al. [30], Sheibani et al. [31], and Zhang et al. [32] collectively highlight ACT’s efficacy in improving psychological and spiritual well-being among individuals with CVD.
The importance of mental health in women with CVD is multifaceted. It encompasses risk reduction, early intervention, treatment adherence, improved quality of life, and overall better cardiovascular outcomes. A holistic approach to women’s cardiovascular care should include a focus on mental health, emphasizing the need for screening, assessment, and intervention for mental health concerns alongside traditional medical management. This integrated approach can lead to more effective care and a higher quality of life for women living with CVD. Psychological treatments are an integral part of the comprehensive care provided to patients with CVD. They can help manage stress, anxiety, depression, and other emotional factors, facilitate behavior change, and improve overall well-being, all of which can contribute to better cardiovascular outcomes and a higher quality of life for these patients. Healthcare providers must consider the psychological aspects of CVD and integrate psychological interventions into the overall treatment plan for these patients. The present study was conducted with the aim of the effectiveness of ACT on psychological distress, alexithymia, and spiritual health of women with CVD.
Materials and Methods
The research design employed in this study was a randomized controlled clinical trial, utilizing a pre-test-post-test design supplemented with a control group. The statistical population under study consisted of women with CVD residing in the 6th district of Tehran during August and September the year 2021. After preparing a list of 30 patients (who had been diagnosed with CVD by a cardiologist), the researchers assigned 15 patients to the experimental and control groups by lottery. The determination of the sample size for this study was predicated upon earlier research and aligned with the parameters set forth by the G*Power software, version 3.1.9.7 (effect size=1.53, 1−β=0.97, and α=0.05) [33]. The inclusion criteria for participation in the study encompassed factors such as personal contentment, age range between 25 and 50 years (the disease is not due to old age), literacy for reading and writing, and the absence of psychiatric medication usage. Conversely, participants were excluded from the study if they failed to respond to questionnaire items, experienced an escalation in pain intensity, or missed more than two therapy sessions.
ACT
To select patients with CVD, two hospitals were referred. These individuals sought medical treatment for their condition at hospitals within the 6th district of Tehran (Gandhi and Mustafa Khomeini). Following the acquisition of consent from clinic authorities and patients, a total of 30 women diagnosed with CVD by their cardiologists were assigned to the intervention and control groups. The research questionnaires were completed by members of both groups in the form of a pre-test. Due to the unfavorable conditions of the disease, it was tried to collect the pre-test scores in person and online (questionnaire link in Google form). ACT sessions by a therapist specializing in chronic diseases in the psychology clinic were then performed in eight 90-minute weekly group sessions for the experimental group, while the control group did not receive any intervention. To prevent the exchange of information between the members of the groups, they were asked not to discuss the content of the meetings with each other. For this reason, there was no dropout in the groups. ACT was designed based on the ACT programs proposed by Hayes et al. [34] and also taking into account the key characteristics in the design of ACT programs (Table 1).
To comply with ethical principles, after collecting the post-test, treatment sessions were also held for the control group.
Measurement tools
Psychological distress scale (DASS-42)
The concise version of the DASS-42, grouped into three subscales: Depression, anxiety, and stress [35]. Each subscale has 14 questions, rated on a Likert scale of zero to three. Participants assess the extent of their experience of each condition over the past week, using a 4-point intensity/frequency scale. Scores for each subscale range from 0 to 42, where higher scores indicate greater psychological distress [34]. In the Iranian context, Cronbach’s α coefficients for anxiety, depression, and stress are 0.85, 0.90, and 0.82, respectively [36]. In the present study, the content validity index (CVI) and content validity ratio index (CVR) were used to measure the content validity of the questionnaire. The CVI and CVR of the questionnaire were 0.83 and 0.87, respectively, which show the validity of the desired content of the DASS-42. Also, Cronbach’s α coefficients for anxiety (0.86), depression (0.84), and stress (0.81) subscales showed reliable consistency.
Toronto alexithymia scale (TAS-20)
The 20-item alexithymia scale, developed by Bagby et al. [37] includes three subscales: Difficulty identifying feelings, difficulty describing feelings, and externally oriented thinking. Responses are assessed on a five-point Likert scale, ranging from 1 (completely disagree) to 5 (completely agree). Scores range from 20 to 100. Bagby et al. [37] established reliability with Cronbach’s α of 0.81 and test re-test reliability of 0.77. In Iran, Cronbach’s α ranged from 0.71 to 0.83, and test re-test reliability from 0.61 to 0.69 [38]. In the present study, the CVI and CVR were used to measure the content validity of the questionnaire. The CVI and CVR of the questionnaire were 0.89 and 0.81, respectively, which show the validity of the desired content of the DASS-42. Also, Cronbach’s α for subscales were 0.81, 0.86, and 0.84, indicating good internal consistency.
Spiritual health questionnaire (SHQ)
The SHQ was developed by Bufford et al. [39] and comprises 10 items with even numbers assessing existential health, and 10 items with odd numbers evaluating religious health. The combined spiritual health score, ranging from 20 to 120, results from both subsets’ cumulative scores. Respondents’ answers follow a six-point Likert scale. Bufford et al. [39] established the scale’s validity and reliability at 0.86 and 0.91, respectively, among students. In Iran, the questionnaire exhibited a Cronbach’s α coefficient of 0.85 [40]. In the present study, the CVI and CVR were used to measure the content validity of the questionnaire. The CVI and CVR of the questionnaire were 0.84 and 0.83, respectively, which show the validity of the desired content of the DASS-42. Also, internal consistency was strong, with Cronbach’s α coefficients of 0.89 for existential health and 0.84 for religious health.
Statistical analyses
To analyze the research data, descriptive statistics including Mean±SD and covariance analysis were used based on their assumptions with the help of SPSS software, version 24. The significance level of these tests was considered 0.05. The Shapiro-Wilk test results were reported to check the normality of the distribution of variables in the two groups. According to the results, normal distribution was met for all variables. The study used multivariate analysis of covariance to assess the effectiveness of ACT on psychological distress, alexithymia, and spiritual health in women with CVD. The researchers tested various assumptions about the equality of variance, covariance matrix, and regression coefficients. The results indicated that these assumptions were valid.
Results
The Mean±SD of the age of the experimental and control groups were 49.12±5.27 and 48.74±4.86, respectively. As displayed in Table 2, highlights no statistically significant differences between the two groups in terms of demographic variables.
The Mean±SD of pre-test-post-test scores of psychological distress, alexithymia, and spiritual health in patients with CVD in the experimental and control groups are presented in Table 3.
According to Table 3, there was a significant difference in the pre-test scores of the two experimental and control groups.
The results of the Levin test to examine the homogeneity of variance of dependent variables in groups showed that the variance of psychological distress (F=2.615, P=0.117), alexithymia (F=1.50, P=0.231), and spiritual health (F=1.37, P=0.251) were equal in the groups. The results of the Box test to evaluate the equality of the covariance matrix of dependent variables between the experimental and control groups also showed that the covariance matrix of the dependent variables is equal (box M=55.43, F=1.06, P=0.377). Also, the results of the chi-square-Bartlett test to examine the sphericity or significance of the relationship between psychological distress, alexithymia, and spiritual health showed that the relationship between them is significant (χ2=140.88, df=35, P<0.05). The homogeneity of regression coefficients was examined through the interaction of dependent variables and independent variables (intervention method) in the pre-test and post-test. The interaction of these pre-tests and post-tests with the independent variable was not significant and indicated the homogeneity of the regression slope. Therefore, all assumptions of multivariate analysis of covariance were met. Table 4 shows the results of multivariate analysis of covariance for comparison between the two groups.
The marginal post-test score adjusted for baseline covariate showed that there was a significant difference between the two groups in terms of anxiety (F=34.71), stress (F=30.14), depression (F=48.34), difficulty identifying feelings (F=28.80), difficulty describing feelings (F=44.30), externally oriented thinking (F=36.50), existential health (F=37.69), and religious health (F=24.56) at the level of 0.001. These findings indicate that there is a significant difference between the groups in these variables.
Discussion
The present study was conducted with the aim of the effectiveness of ACT on psychological distress, alexithymia, and spiritual health of women with CVD. The results of the present study showed that women with CVD had less anxiety, depression, and stress after receiving treatment based on ACT. These findings are in line with the research of Dar et al. [8]; Osborne et al. [9]; Pimple et al. [10] and Bouchard et al. [11].
ACT can be beneficial in improving psychological well-being and reducing symptoms of anxiety, depression, and stress in various populations, including those with chronic health conditions [30]. In the case of women with CVD, ACT might have been used as an adjunct to traditional medical treatment to address their mental health concerns. The stress and emotional burden associated with a CVD diagnosis can significantly impact a person’s overall well-being [24]. By promoting acceptance, mindfulness, and value-driven actions, ACT equips women with the necessary tools to enhance their emotional well-being and overall quality of life. While medical interventions remain crucial, addressing the psychological aspects of CVD is equally vital for providing comprehensive care to women facing this challenging health condition [31]. The results of Dar et al. [8] determined that people who have high levels of psychological distress are at risk of CVD. On the other hand, the findings of a review study by Osborne et al. [9] showed that stress, anxiety, and depression are among the aggravating factors in the onset and increase of CVD levels.
The findings of the present study showed that women with CVD had less difficulty identifying feelings, difficulty describing feelings, and externally oriented thinking after receiving ACT. These findings are in line with studies by Maqbool et al. [14]; Lazarević et al. [15]; Aluja et al. [16] and Wiernik et al. [17].
ACT can be a useful therapeutic approach for individuals struggling with alexithymia. By promoting acceptance of emotions and thoughts without judgment, individuals with alexithymia can begin to develop a greater understanding and awareness of their emotions [14]. Mindfulness practices in ACT can help individuals become more attuned to their bodily sensations and emotional experiences, which can be beneficial for those with alexithymia, as they might find it challenging to identify emotions based solely on cognitive appraisal [26]. The values clarification and committed action aspects of ACT can help individuals with alexithymia align their behaviors with their deeper values, even if they struggle to connect with their emotions directly [30]. The study’s findings underscore the significant impact of ACT in reducing alexithymia among women with CVD. By addressing this often-overlooked emotional factor, healthcare providers can contribute to improved patient outcomes, enhanced emotional well-being, and better quality of life for women living with cardiovascular conditions [25]. The results of Maqbool et al. [14] revealed that a significant number of patients with CVD have high levels of alexithymia, which causes them to not pursue treatment. On the other hand, the findings of Lazarević et al. [15] study indicated a significant positive correlation between alexithymia and CVD. In the meantime, people who had problems recognizing their emotions were indifferent to their illness and did not make efforts to increase their quality of life and mental health.
The results of the present study showed that women with CVD had higher existential and religious health after receiving ACT. These findings are in line with the research of Aryafard et al. [20]; Heshmati et al. [21]; Brewer et al. [22] and von Flach et al. [23].
The journey with CVD can evoke existential questions and prompt a search for meaning and purpose, making spiritual health vital for overall well-being. ACT’s emphasis on values and committed action aligns with many spiritual principles, encouraging women to connect with their spiritual beliefs and integrate them into their lives [24]. As women identify and live in alignment with their spiritual values, they may experience greater spiritual growth and a deeper sense of purpose [31]. Spirituality is a deeply personal and transformative aspect of human existence, encompassing the search for meaning, purpose, and connection to something greater than oneself. Many individuals find solace, guidance, and a sense of fulfillment in their spiritual beliefs and practices [27]. In recent years, mental health professionals have recognized the significance of integrating spirituality into therapy to support individuals on their journey toward holistic well-being [29]. Both ACT and spirituality recognize the impermanent and uncertain nature of life. Through ACT’s focus on values and mindfulness, individuals can develop resilience and cope with difficult emotions and challenging life circumstances. This can lead to a more profound acceptance of uncertainty, fostering a sense of surrender and trust in one’s spiritual journey [28]. The results of a review study by Aryafard et al. [20] determined that the spiritual health of Iranian patients with CVD is average, which requires further improvement. On the other hand, the findings of Heshmati et al. [21] indicated a significant correlation between hope, optimism, and spiritual well-being. Patients with high levels of spirituality were less likely to have severe vascular disease.
The impossibility of controlling the social, educational, and economic status of the research participants was one of the limitations of the research. Therefore, it is suggested that in future research, efforts should be made to control these components. Also, due to the conditions of the COVID-19 epidemic, a small sample size was selected, and it is suggested that more patients be investigated in future studies. The impossibility of long-term follow-up of the impact of the program using a follow-up test was another limitation. Based on this, it is suggested that this issue be taken into consideration in future research so that it is possible to examine the long-term impact of ACT.
Conclusion
ACT offers promising prospects in improving the psychological, emotional, and spiritual health of women living with CVD. By promoting acceptance, emotional awareness, and committed action, ACT empowers women to cope effectively with psychological distress, address alexithymia, and nurture their spiritual well-being. As a holistic therapeutic approach, ACT acknowledges the interconnectedness of these dimensions, allowing women to find strength, purpose, and resilience as they navigate the challenges of living with CVD. As further research unfolds, the potential of ACT in enhancing the overall well-being of women with CVD remains an essential focus for clinicians and researchers alike.
Ethical Considerations
Compliance with ethical guidelines
The present study was approved by Ethics Committee of Baqiyatallah University of Medical Sciences (Code: IR.BMSU.BAQ.REC.1399.011).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision: Farzin Bagheri Sheykhangafshe and Vahid Savabi Niri; Methodology: Maryam Zolfagharnia, Zeynab Bourbour and Forough Esrfilian; Investigation: Farzin Bagheri Sheykhangafshe and Vahid Savabi Niri; Writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank all the participants in this research.
References
- Vogel B, Acevedo M, Appelman Y, Bairey Merz CN, Chieffo A, Figtree GA, et al. The Lancet women and cardiovascular disease Commission: Reducing the global burden by 2030. Lancet. 2021; 397(10292):2385-438. [DOI:10.1016/S0140-6736(21)00684-X] [PMID]
- Mehta LS, Velarde GP, Lewey J, Sharma G, Bond RM, Navas-Acien A, et al. Cardiovascular disease risk factors in women: The impact of race and ethnicity: A scientific statement from the american heart association. Circulation. 2023; 147(19):1471-87. [DOI:10.1161/CIR.0000000000001139] [PMID]
- Geraghty L, Figtree GA, Schutte AE, Patel S, Woodward M, Arnott C. Cardiovascular disease in women: From pathophysiology to novel and emerging risk factors. Heart Lung Circ. 2021; 30(1):9-17. [DOI:10.1016/j.hlc.2020.05.108] [PMID]
- Townsend N, Kazakiewicz D, Lucy Wright F, Timmis A, Huculeci R, Torbica A, et al. Epidemiology of cardiovascular disease in Europe. Nat Rev Cardiol. 2022; 19(2):133-43. [DOI:10.1038/s41569-021-00607-3] [PMID]
- Sarrafzadegan N, Mohammmadifard N. Cardiovascular Disease in Iran in the last 40 years: Prevalence, mortality, morbidity, challenges and strategies for cardiovascular prevention. Arch Iran Med. 2019; 22(4):204-10. [PMID]
- Sumner JA, Cleveland S, Chen T, Gradus JL. Psychological and biological mechanisms linking trauma with cardiovascular disease risk. Transl Psychiatry. 2023; 13(1):25.[DOI:10.1038/s41398-023-02330-8] [PMID] [PMCID]
- Vaccarino V, Badimon L, Bremner JD, Cenko E, Cubedo J, Dorobantu M, et al. Depression and coronary heart disease: 2018 position paper of the ESC working group on coronary pathophysiology and microcirculation. Eur Heart J. 2020; 41(17):1687-96. [DOI:10.1093/eurheartj/ehy913] [PMID] [PMCID]
- Dar T, Radfar A, Abohashem S, Pitman RK, Tawakol A, Osborne MT. Psychosocial stress and cardiovascular disease. Curr Treat Options Cardiovasc Med. 2019; 21(5):23. [DOI:10.1007/s11936-019-0724-5] [PMID] [PMCID]
- Osborne MT, Shin LM, Mehta NN, Pitman RK, Fayad ZA, Tawakol A. Disentangling the links between psychosocial stress and cardiovascular disease. Circ Cardiovasc Imaging. 2020; 13(8):e010931. [DOI:10.1161/CIRCIMAGING.120.010931] [PMID] [PMCID]
- Pimple P, Lima BB, Hammadah M, Wilmot K, Ramadan R, Levantsevych O, et al. Psychological distress and subsequent cardiovascular events in individuals with coronary artery disease. J Am Heart Assoc. 2019; 8(9):e011866. [DOI:10.1161/JAHA.118.011866] [PMID] [PMCID]
- Bouchard V, Robitaille A, Perreault S, Cyr MC, Tardif JC, Busseuil D, et al. Psychological distress, social support, and use of outpatient care among adult men and women with coronary artery disease or other non-cardiovascular chronic disease. J Psychosom Res. 2023; 165:111131. [DOI:10.1016/j.jpsychores.2022.111131] [PMID]
- Waldstein SR, Kauhanen J, Neumann SA, Katzel LI. Alexithymia and cardiovascular risk in older adults: Psychosocial, psychophysiological, and biomedical correlates. Psychol Health. 2002; 17(5):597-610. [DOI:10.1080/08870440290025803]
- Sancassiani F, Montisci R, Preti A, Paribello P, Meloni L, Romano F, et al. Surviving to acute myocardial infarction: The role of psychological factors and alexithymia in delayed time to searching care: A systematic review. J Clin Med. 2021; 10(17):3813. [DOI:10.3390/jcm10173813] [PMID] [PMCID]
- Maqbool R, Iqbal MN, Rafiq M, Anjum A, Qamar S, Ahmed MM. Alexithymia, posttraumatic growth, and life contentment among cardiac sufferers. Pak J Med Res. 2022; 61(3):134-8. [Link]
- Lazarević M. Connection between alexithymia and chronic diseases of the heart and lungs. Acta Fac Med Naissensis. 2023; 40(2):171-8. [DOI:10.5937/afmnai40-41356]
- Aluja A, Malas O, Urieta P, Worner F, Balada F. Biological correlates of the Toronto Alexithymia Scale (TAS-20) in cardiovascular disease and healthy community subjects. Physiol Behav. 2020; 227:113151. [DOI:10.1016/j.physbeh.2020.113151] [PMID]
- Wiernik E, Lemogne C, Fezeu L, Arnault N, Hercberg S, Kesse-Guyot E, et al. Association between alexithymia and risk of incident cardiovascular diseases in the supplémentation en vitamines et minéraux antioxydants (SU.VI.MAX) cohort. Psychosom Med. 2018; 80(5):460-7. [DOI:10.1097/PSY.0000000000000592] [PMID]
- Janssen-Niemeijer AJ, Visse M, Van Leeuwen R, Leget C, Cusveller BS. The role of spirituality in lifestyle changing among patients with chronic cardiovascular diseases: A literature review of qualitative studies. J Relig Health. 2017; 56(4):1460-77. [DOI:10.1007/s10943-017-0384-2] [PMID]
- Bagheri Sheykhangafshe F, Shabahang R. [Prediction of Psychological wellbeing of elderly people based on spirituality, social support, and optimism (Persian)]. J Relig Health. 2020; 7(2):22-32. [Link]
- Aryafard H, Dehvan F, Albatineh AN, Dalvand S, Gheshlagh RG. Spiritual health in Iranian patients with cardiovascular diseases: A systematic review and meta-analysis. Omega. 2022; 302228221108293. [DOI:10.1177/00302228221108293] [PMID]
- Heshmati R, Jafari E, Salimi Kandeh T, Caltabiano ML. Associations of spiritual well-being and hope with health anxiety severity in patients with advanced coronary artery disease. Medicina. 2021; 57(10):1066. [DOI:10.3390/medicina57101066] [PMID] [PMCID]
- Brewer LC, Bowie J, Slusser JP, Scott CG, Cooper LA, Hayes SN, et al. Religiosity/spirituality and cardiovascular health: the american heart association life's simple 7 in african americans of the jackson heart study. J Am Heart Assoc. 2022; 11(17):e024974. [DOI:10.1161/JAHA.121.024974] [PMID] [PMCID]
- von Flach MDRT, Ritt LEF, Santana Junior FG, Correia MVF, Claro TC, Ladeia AM, et al. Spirituality, functional gain, and quality of life in cardiovascular rehabilitation. Arq Bras Cardiol. 2023; 120(3):e20220452. [DOI:10.36660/abc.20220452] [PMID]
- Fiedorowicz JG, Dindo L, Ajibewa T, Persons J, Marchman J, Holwerda SW, et al. One-day acceptance and commitment therapy (ACT) workshop improves anxiety but not vascular function or inflammation in adults with moderate to high anxiety levels in a randomized controlled trial. Gen Hosp Psychiatry. 2021; 73:64-70. [DOI:10.1016/j.genhosppsych.2021.09.009] [PMID] [PMCID]
- Bagheri-Sheykhangafshe F, Kiani A., Savabi-Niri V, Aghdasi N, Bourbour Z. The efficacy of acceptance and commitment therapy on psychological capital and emotion regulation of students with suicidal ideation. Int J Behav Sci. 2022; 16(2):96-102. [DOI:10.30491/IJBS.2022.335463.1779]
- Spatola CA, Manzoni GM, Castelnuovo G, Malfatto G, Facchini M, Goodwin CL, et al. The ACTonHEART study: Rationale and design of a randomized controlled clinical trial comparing a brief intervention based on Acceptance and Commitment Therapy to usual secondary prevention care of coronary heart disease. Health Qual Life Outcomes. 2014; 12:22. [DOI:10.1186/1477-7525-12-22] [PMID] [PMCID]
- Farzaneh A, Marzieh S, Abed M. A comparative study on the effectiveness of acceptance and commitment therapy (ACT) and schema therapy (ST) on problem-solving styles in people with heart diseases. Ann Rom Soc Cell Biol. 2021:21114-26. [DOI:10.53730/ijhs.v6nS6.10302]
- Kheyran-Alnesa M, Mirzaian B, Yar-Ali D. The effectiveness of acceptance and commitment-based therapy on anger, anxiety, and hostility for heart surgery patients. J Biochem Technol. 2018; 9(4):43. [Link]
- Herbert MS, Dochat C, Wooldridge JS, Materna K, Blanco BH, Tynan M, et al. Technology-supported acceptance and commitment therapy for chronic health conditions: A systematic review and meta-analysis. Behav Res Ther. 2022; 148:103995. [DOI:10.1016/j.brat.2021.103995] [PMID] [PMCID]
- Rashidi A, Whitehead L, Newson L, Astin F, Gill P, Lane DA, et al. The role of acceptance and commitment therapy in cardiovascular and diabetes healthcare: A scoping review. Int J Environ Res Public Health. 2021; 18(15):8126.[DOI:10.3390/ijerph18158126] [PMID] [PMCID]
- Sheibani H, Sheibani KA, Amreei NN, Masrour MJ. An investigation of the effects of the acceptance and commitment therapy in groups on the cognitive strategies of emotion regulation and self-control in coronary heart disease patients. J Med Life. 2019; 12(4):361-7. [DOI:10.25122/jml-2019-0035] [PMID] [PMCID]
- Zhang X, Haixia M, Yee LC, Wk HG, Mak YW. Effectiveness of acceptance and commitment therapy on self-care, psychological symptoms, and quality of life in patients with cardiovascular disease: A systematic review and meta-analysis. J Contextual Behav Sci. 2023. [DOI:10.1016/j.jcbs.2023.05.007]
- Faul F, Erdfelder E, Lang AG, & Buchner A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007; 39(2): 175-191. [DOI:10.3758/BF03193146] [PMID]
- Hayes SC, Strosahl KD, Wilson KG. Acceptance and commitment therapy: The process and practice of mindful change. New York: Guilford Press; 2011. [Link]
- Lovibond PF, Lovibond SH. The structure of negative emotional states: Comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behav Res Ther. 1995; 33(3):335-43. [DOI:10.1016/0005-7967(94)00075-U] [PMID]
- Bagheri Sheykhangafshe F, Fathi-Ashtiani A, Savabi Niri V, Sarlak N, Deldari Alamdari M. [Comparison of post-traumatic stress, burnout, and psychological disorders in nurses with and without COVID-19 (Persian)]. Iran J Nurs. 2022; 35(138):346-59. [DOI:10.32598/ijn.35.138.2862.2]
- Bagby RM, Taylor GJ, Parker JD. The twenty-item toronto alexithymia scale--II. Convergent, discriminant, and concurrent validity. J Psychosom Res. 1994; 38(1):33-40. [DOI:10.1016/0022-3999(94)90006-X] [PMID]
- Besharat MA. Psychometric properties of the Farsi version of the emotional intelligence scale-41 (FEIS-41). Pers Individ Differ. 2007; 43(5):991-1000. [DOI:10.1016/j.paid.2007.02.020]
- Bufford RK, Paloutzian RF, Ellison CW. Norms for the spiritual well-being scale. J Psychol Theol. 1991; 19(1):56-70. [DOI:10.1177/009164719101900106]
- Janbabaei G, Esmaeili R, Mosavinasab N, Rajbar M. [A survey of the role of spiritual health and its related factors in the patients with metastatic digestive cancer (Persian)]. J Relig Health. 2014; 2(1):9-14. [Link]
Article Type: Original Contributions |
Subject:
Health Management
Received: 2023/11/6 | Accepted: 2024/03/20 | Published: 2024/04/1
Received: 2023/11/6 | Accepted: 2024/03/20 | Published: 2024/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
