

Volume 9, Issue 1 (1-2024)
CJHR 2024, 9(1): 21-32 |
Back to browse issues page


Ethics code: IR.IAU.TABRIZ.REC.1400.02
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rabipour F, Hosseininasab S D, Salari A. Effectiveness of Mindfulness-Based Stress Reduction on Executive Functions in Patients with Hypertension: A Randomized Clinical Trial. CJHR 2024; 9 (1) :21-32
URL: http://cjhr.gums.ac.ir/article-1-349-en.html
URL: http://cjhr.gums.ac.ir/article-1-349-en.html



1- Department of Psychology, Tabriz Branch, Islamic Azad University, Tabriz, Iran.
2- Department of Psychology, Tabriz Branch, Islamic Azad University, Tabriz, Iran. , d.hosseininasab@iaut.ac.ir
3- Cardiovascular Diseases Research Center, Department of Cardiology, Guilan University of Medical Sciences, Rasht, Iran.
2- Department of Psychology, Tabriz Branch, Islamic Azad University, Tabriz, Iran. , d.hosseininasab@iaut.ac.ir
3- Cardiovascular Diseases Research Center, Department of Cardiology, Guilan University of Medical Sciences, Rasht, Iran.
Full-Text [PDF 956 kb]
(81 Downloads)
| Abstract (HTML) (202 Views)

Full-Text: (81 Views)
Introduction
Hypertension is a serious medical condition and the primary cause of cardiovascular diseases and early death around the world [1]. The global burden of disease study showed that hypertension was responsible for the highest years of life lost due to premature death [2]. Extensive use of antihypertensive medications helped the global average blood pressure to remain constant or slightly decrease [3]; on the other hand, the frequency of hypertension in low to middle-income countries has increased [1]. According to various reports, the frequency of hypertension in different locations of the world ranged between 4 to 78 percent. The mean frequencies in the Eastern Mediterranean region and Iran were 29.5% and 22%, respectively [4].
Epidemiological evidence shows that hypertension is a risk factor for dementia onset and cognitive impairment [5, 6, 7, 8, 9]. Also, research backgrounds indicated different executive functions and weaker cognitive functions of patients with hypertension compared with individuals without the disease [10, 11, 12, 13]. Executive function, also known as executive control or cognitive control, refers to a family of top-down mental processes that individuals require when they must focus and when autonomy or relying on instinct or intuition is insufficient or impossible [14]. These processes are thought to be supported (at least to some extent) by structure within the brain’s frontal lobes. There is also a general agreement on the existence of three primary executive functions: Inhibitory control, working memory, and cognitive flexibility, from which prime executive functions, such as logic, problem-solving, and planning, form [14].
Findings of the Honolulu-Asia aging study previously indicated that the relationship between increased blood pressure in middle age and dementia only existed in patients never treated with antihypertensive medication [15]. A recent study, on the other hand, reported that besides the individuals never treated with antihypertensive drugs, patients with treat-resistant hypertension and those whose systolic blood pressure failed to reach the standard value were also exposed to the risk of severe cognitive problems, such as disordered executive functions [16]. Furthermore, antihypertensive drug use, in the long run, considerably exposes individuals to the risk of losing cognitive abilities and mild cognitive impairment compared with individuals with normal blood pressure. However, patients not adhering to treatment face more cognitive issues [11, 16].
Mindfulness-based stress reduction (MBSR) is among the interventions recently applied to a wide range of medical issues to help the condition of patients of different ages [17]. Mindfulness is rooted in Eastern meditative traditions and is often accompanied by formal meditation practice. Mindfulness is called the heart of Buddhist meditation. Nevertheless, mindfulness is more than meditation. It is a state of awareness in nature, which includes conscious attention to one’s moment-by-moment experience. In other words, mindfulness is defined as intentional attention to the experiences of the current moment in an acceptable manner and far from judgment [18]. Various studies indicated mindfulness-based interventions (MBIs) as an effective treatment for enhancing executive functions and reducing cognitive and behavioral problems in different patients. MBI also provided potential confidence as a suitable and effective method for medical care [17, 19-21]. According to estimates, MBIs support participants in mindfulness skills (such as self-awareness, attention control, and emotion regulation) and cause them to act more consistently and correctly regarding other determining factors of the disease, including adherence to antihypertensive drugs, diets, exercise, and stress response [22].
Literature reviews indicated cognitive issues and executive function weaknesses in some patients [11]. Meanwhile, most studies focus on the correlations and etiology, or variables related to hypertension and cardiovascular problems of the patients, and ignore the effectiveness of treatments affecting the cognitive features of hypertension patients. Furthermore, even though MBSR is among the well-received treatments for improving cognitive functions in various sample groups, its effect on the executive and cognitive functions of patients with hypertension has not been investigated, and the number of available studies is limited. On the other hand, inconsistent results of studies, including Askari et al. (2023) [23], and Marciniak et al. (2020) [24], who didn’t confirm the efficiency of MBIs on the executive and cognitive functions of the patients, add to the necessity of this study. Considering the mentioned discussions, the present study aimed to investigate the efficacy of mindfulness-based stress reduction on the executive functions of patients with hypertension.
Materials and Methods
Study type and population
The current research was conducted as a double-blind randomized clinical trial with a control group based on a pre-test, post-test and two-month follow-up design. The study population was all patients with hypertension referred to Heshmat Heart Hospital in Rasht City in 2021. Forthy qualified volunteers of this population were included in the study by the purposive sampling method. The sample size was 40 people according to previous similar studies [25-27], and anticipating 30% dropout due to the conditions of the COVID-19 pandemic. Finally, six subjects dropped out during the study. The inclusion criteria were as follows: Primary (essential) hypertension according to the medical record and under routine medical treatment for at least 6 months since the diagnosis, obtaining a score of less than 3, for the component of completed categories in the Wisconsin test, age range of 30-60 years, ability to speak, read and write, informed consent and willing to participate in the research; and exclusion criteria were: Absence of more than two sessions, inability or unwillingness to use computer or internet; unwilling to continue training, participation in courses at the same time or in the last two months, drug and alcohol abuse, severe personality and clinical disorders or suicidal ideation (according to the Minnesota personality inventory (MMPI scale scores from 71 items) and a clinical interview session by a clinical psychologist), recent head trauma and brain injuries or receiving electric shock or special treatment in the last six months (self report).
Study procedure
After receiving the code of ethics and the clinical trial code, it was coordinated with the Heshmat Heart Research Center in Rasht City; the patients were first visited by a cardiologist at the Heshmat Heart Research Center, then they were referred to the researcher, in the same hospital. In the first meeting, for each patient, the purpose and method of conducting the research were explained, and the demographic characteristics and ethical consent forms were completed. The selected people were assigned to two intervention and control groups using the internet randomization method and the allocation concealment was done by using Sequentially numbered, opaque, sealed envelope (SNOSE) by creating a random sequence. Based on the research sample’ size, several aluminium envelopes were prepared and each of the created random sequence was recorded on a card and the cards were respectively placed inside the envelope. Also, in order to maintain the random sequence, the outer surface of the envelopes was numbered in the same order. Finally, the envelopes were glued, closed and placed in a box. Starting the work, the envelopes were opened in order and the allocated group of the participants was revealed. Both group completed pre-test for measuring executive functions with the Wisconsin test, then the experimental group went under intervention by a psychologist proficient in MBI. After the completion of the intervention, a post-test was taken, and a follow-up was conducted two months later.
Course description
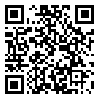
The first and perhaps the most well-known empirically supported MBI in the treatment of psychological symptoms, used in this study, is MBSR, developed by Kabat-Zinn in the early 1980s. MBSR is an 8-week structured training program, taught in a group way [18, 28]. We used a psychologist expert in mindfulness to teach this course to the participants and the control group did not receive any type of training at the same time. To prevent withdrawal and to ensure that homework was completed, the participants were contacted regularly (once a week) and one day before each session, and the possible benefits of the study were discussed with them and they were encouraged to continue the study. During the 8-week online course synchronous (one 120-minute session each week), a variety of MBSR techniques including awareness of breathing, eating meditation, body scan, and a number of other techniques were taught and practiced. During the sessions, the experiences of the participants were shared in the form of a group discussion about the benefits of mindfulness in lifestyle behaviors related to hypertension. Also, exercises in the format of voice and video were presented to each participant so that they can use them in their daily homework. The adapted summary of MBSR sessions [29, 30] is presented in Table 1.

Measurement tools
In order to collect information, in the first session (screening), the form of demographic characteristics, including gender, age, education level, marital status, employment status, exercise and smoking was completed by the participants as a self-report. Duration of illness, medication status and substance abuse and other physical was checked through clinical interviews and medical record. Also, mental diseases were checked through clinical interviews and MMPI scale scores from 71 items by a clinical psychologist). In addition, height and weight (body mass index) were measured with a digital scale and measuring tape by the first author of the study.
In order to measure the research variable, the computerized standard Wisconsin test was implemented individually in face-to-face sessions.
Wisconsin card sorting test (computer version)
Grant and Berg (1948) introduced the Wisconsin card sorting test [31], and then Heaton et al. developed the computer version in 1993 [32]. This test is among the primary indicators for determining the function of the brain’s frontal lobes and the most common test for evaluating executive functions [33]. This tool includes four primary cards (including a triangle, star, cross, and circle), constantly displayed on top of the monitor display until the end of the test. Sixty other cards in random order appear at the bottom of the display, one after another. When a card is displayed on the monitor, the participant must decide that considering the three parameters (i.e. color, shape, number), this card must be placed under which of the primary cards. The display monitor instantly shows the correct or wrong feedback after the participant’s response. The intended pattern changes after ten successive correct answers by the participant [33]. The Wisconsin exam has several outputs and scoring methods. The most common grading method is to record the number of completed categories and perseverative errors. The number of completed categories which range from 0 to 6, refer to the number of correct courses or in other words ten consecutive correct answers. A Perseverative Error is recorded when one continues to categorize according to a previously successful principle (regardless of incorrect feedback) and also when, in the first series, they persist in categorizing based on an initial incorrect guess. The range of perseverative errors’ score can be between 0 and 60. Obtaining a higher score in the completed categories, as well as a lower score in the Perseverative Errors, indicates a person’s better executive functions [33]. In the present study, two outputs of completed categories and perseverative errors were reported. The validity and reliability of this test, has been confirmed in many studies around the world. Kopp et al. (2021) reported the reliability of this tool using Cronbach’s α method as 0.95 [34]. In Iran, Shahgholian et al. (2012) designed and assessed the psychometric properties of the computer version of the Wisconsin card sorting test. Differential validity was investigated using two groups of low anxiety and high anxiety, and the result of the test was 2.56 for the completed categories component, and 1.99 for the perseverative errors component, which distinguished the two groups well. The reliability coefficient using Cronbach’s α method for completed categories and perseverative errors were 0.73 and 0.74, respectively, and the reliability coefficient using the split-half method was 0.83 and 0.87, respectively [33].
Statistical analysis
Mean±SD were used to describe data. To determine the normality assumption of dependent variables distribution, skewness and kurtosis were investigated. Chi-square and t-test were used to compare variables between the two groups. Mauchly’s test was used to check the sphericity or equality of variance of the differences among the research variables levels; also, the M-box test was used to check the assumption of homogeneity of the covariance matrices; and the Leven’s test was used to check the equality of variances. To check the hypotheses, repeated measures analysis of variance (ANOVA) and Bonferroni post-hoc test were used. Data were analyzed in SPSS software version 26 at a significance level of 0.05.
Results
Out of 40 eligible patients, 17 were completed the study and were analysed. The Flow diagram of the study is shown in Figure 1.
Hypertension is a serious medical condition and the primary cause of cardiovascular diseases and early death around the world [1]. The global burden of disease study showed that hypertension was responsible for the highest years of life lost due to premature death [2]. Extensive use of antihypertensive medications helped the global average blood pressure to remain constant or slightly decrease [3]; on the other hand, the frequency of hypertension in low to middle-income countries has increased [1]. According to various reports, the frequency of hypertension in different locations of the world ranged between 4 to 78 percent. The mean frequencies in the Eastern Mediterranean region and Iran were 29.5% and 22%, respectively [4].
Epidemiological evidence shows that hypertension is a risk factor for dementia onset and cognitive impairment [5, 6, 7, 8, 9]. Also, research backgrounds indicated different executive functions and weaker cognitive functions of patients with hypertension compared with individuals without the disease [10, 11, 12, 13]. Executive function, also known as executive control or cognitive control, refers to a family of top-down mental processes that individuals require when they must focus and when autonomy or relying on instinct or intuition is insufficient or impossible [14]. These processes are thought to be supported (at least to some extent) by structure within the brain’s frontal lobes. There is also a general agreement on the existence of three primary executive functions: Inhibitory control, working memory, and cognitive flexibility, from which prime executive functions, such as logic, problem-solving, and planning, form [14].
Findings of the Honolulu-Asia aging study previously indicated that the relationship between increased blood pressure in middle age and dementia only existed in patients never treated with antihypertensive medication [15]. A recent study, on the other hand, reported that besides the individuals never treated with antihypertensive drugs, patients with treat-resistant hypertension and those whose systolic blood pressure failed to reach the standard value were also exposed to the risk of severe cognitive problems, such as disordered executive functions [16]. Furthermore, antihypertensive drug use, in the long run, considerably exposes individuals to the risk of losing cognitive abilities and mild cognitive impairment compared with individuals with normal blood pressure. However, patients not adhering to treatment face more cognitive issues [11, 16].
Mindfulness-based stress reduction (MBSR) is among the interventions recently applied to a wide range of medical issues to help the condition of patients of different ages [17]. Mindfulness is rooted in Eastern meditative traditions and is often accompanied by formal meditation practice. Mindfulness is called the heart of Buddhist meditation. Nevertheless, mindfulness is more than meditation. It is a state of awareness in nature, which includes conscious attention to one’s moment-by-moment experience. In other words, mindfulness is defined as intentional attention to the experiences of the current moment in an acceptable manner and far from judgment [18]. Various studies indicated mindfulness-based interventions (MBIs) as an effective treatment for enhancing executive functions and reducing cognitive and behavioral problems in different patients. MBI also provided potential confidence as a suitable and effective method for medical care [17, 19-21]. According to estimates, MBIs support participants in mindfulness skills (such as self-awareness, attention control, and emotion regulation) and cause them to act more consistently and correctly regarding other determining factors of the disease, including adherence to antihypertensive drugs, diets, exercise, and stress response [22].
Literature reviews indicated cognitive issues and executive function weaknesses in some patients [11]. Meanwhile, most studies focus on the correlations and etiology, or variables related to hypertension and cardiovascular problems of the patients, and ignore the effectiveness of treatments affecting the cognitive features of hypertension patients. Furthermore, even though MBSR is among the well-received treatments for improving cognitive functions in various sample groups, its effect on the executive and cognitive functions of patients with hypertension has not been investigated, and the number of available studies is limited. On the other hand, inconsistent results of studies, including Askari et al. (2023) [23], and Marciniak et al. (2020) [24], who didn’t confirm the efficiency of MBIs on the executive and cognitive functions of the patients, add to the necessity of this study. Considering the mentioned discussions, the present study aimed to investigate the efficacy of mindfulness-based stress reduction on the executive functions of patients with hypertension.
Materials and Methods
Study type and population
The current research was conducted as a double-blind randomized clinical trial with a control group based on a pre-test, post-test and two-month follow-up design. The study population was all patients with hypertension referred to Heshmat Heart Hospital in Rasht City in 2021. Forthy qualified volunteers of this population were included in the study by the purposive sampling method. The sample size was 40 people according to previous similar studies [25-27], and anticipating 30% dropout due to the conditions of the COVID-19 pandemic. Finally, six subjects dropped out during the study. The inclusion criteria were as follows: Primary (essential) hypertension according to the medical record and under routine medical treatment for at least 6 months since the diagnosis, obtaining a score of less than 3, for the component of completed categories in the Wisconsin test, age range of 30-60 years, ability to speak, read and write, informed consent and willing to participate in the research; and exclusion criteria were: Absence of more than two sessions, inability or unwillingness to use computer or internet; unwilling to continue training, participation in courses at the same time or in the last two months, drug and alcohol abuse, severe personality and clinical disorders or suicidal ideation (according to the Minnesota personality inventory (MMPI scale scores from 71 items) and a clinical interview session by a clinical psychologist), recent head trauma and brain injuries or receiving electric shock or special treatment in the last six months (self report).
Study procedure
After receiving the code of ethics and the clinical trial code, it was coordinated with the Heshmat Heart Research Center in Rasht City; the patients were first visited by a cardiologist at the Heshmat Heart Research Center, then they were referred to the researcher, in the same hospital. In the first meeting, for each patient, the purpose and method of conducting the research were explained, and the demographic characteristics and ethical consent forms were completed. The selected people were assigned to two intervention and control groups using the internet randomization method and the allocation concealment was done by using Sequentially numbered, opaque, sealed envelope (SNOSE) by creating a random sequence. Based on the research sample’ size, several aluminium envelopes were prepared and each of the created random sequence was recorded on a card and the cards were respectively placed inside the envelope. Also, in order to maintain the random sequence, the outer surface of the envelopes was numbered in the same order. Finally, the envelopes were glued, closed and placed in a box. Starting the work, the envelopes were opened in order and the allocated group of the participants was revealed. Both group completed pre-test for measuring executive functions with the Wisconsin test, then the experimental group went under intervention by a psychologist proficient in MBI. After the completion of the intervention, a post-test was taken, and a follow-up was conducted two months later.
Course description
The first and perhaps the most well-known empirically supported MBI in the treatment of psychological symptoms, used in this study, is MBSR, developed by Kabat-Zinn in the early 1980s. MBSR is an 8-week structured training program, taught in a group way [18, 28]. We used a psychologist expert in mindfulness to teach this course to the participants and the control group did not receive any type of training at the same time. To prevent withdrawal and to ensure that homework was completed, the participants were contacted regularly (once a week) and one day before each session, and the possible benefits of the study were discussed with them and they were encouraged to continue the study. During the 8-week online course synchronous (one 120-minute session each week), a variety of MBSR techniques including awareness of breathing, eating meditation, body scan, and a number of other techniques were taught and practiced. During the sessions, the experiences of the participants were shared in the form of a group discussion about the benefits of mindfulness in lifestyle behaviors related to hypertension. Also, exercises in the format of voice and video were presented to each participant so that they can use them in their daily homework. The adapted summary of MBSR sessions [29, 30] is presented in Table 1.
Measurement tools
In order to collect information, in the first session (screening), the form of demographic characteristics, including gender, age, education level, marital status, employment status, exercise and smoking was completed by the participants as a self-report. Duration of illness, medication status and substance abuse and other physical was checked through clinical interviews and medical record. Also, mental diseases were checked through clinical interviews and MMPI scale scores from 71 items by a clinical psychologist). In addition, height and weight (body mass index) were measured with a digital scale and measuring tape by the first author of the study.
In order to measure the research variable, the computerized standard Wisconsin test was implemented individually in face-to-face sessions.
Wisconsin card sorting test (computer version)
Grant and Berg (1948) introduced the Wisconsin card sorting test [31], and then Heaton et al. developed the computer version in 1993 [32]. This test is among the primary indicators for determining the function of the brain’s frontal lobes and the most common test for evaluating executive functions [33]. This tool includes four primary cards (including a triangle, star, cross, and circle), constantly displayed on top of the monitor display until the end of the test. Sixty other cards in random order appear at the bottom of the display, one after another. When a card is displayed on the monitor, the participant must decide that considering the three parameters (i.e. color, shape, number), this card must be placed under which of the primary cards. The display monitor instantly shows the correct or wrong feedback after the participant’s response. The intended pattern changes after ten successive correct answers by the participant [33]. The Wisconsin exam has several outputs and scoring methods. The most common grading method is to record the number of completed categories and perseverative errors. The number of completed categories which range from 0 to 6, refer to the number of correct courses or in other words ten consecutive correct answers. A Perseverative Error is recorded when one continues to categorize according to a previously successful principle (regardless of incorrect feedback) and also when, in the first series, they persist in categorizing based on an initial incorrect guess. The range of perseverative errors’ score can be between 0 and 60. Obtaining a higher score in the completed categories, as well as a lower score in the Perseverative Errors, indicates a person’s better executive functions [33]. In the present study, two outputs of completed categories and perseverative errors were reported. The validity and reliability of this test, has been confirmed in many studies around the world. Kopp et al. (2021) reported the reliability of this tool using Cronbach’s α method as 0.95 [34]. In Iran, Shahgholian et al. (2012) designed and assessed the psychometric properties of the computer version of the Wisconsin card sorting test. Differential validity was investigated using two groups of low anxiety and high anxiety, and the result of the test was 2.56 for the completed categories component, and 1.99 for the perseverative errors component, which distinguished the two groups well. The reliability coefficient using Cronbach’s α method for completed categories and perseverative errors were 0.73 and 0.74, respectively, and the reliability coefficient using the split-half method was 0.83 and 0.87, respectively [33].
Statistical analysis
Mean±SD were used to describe data. To determine the normality assumption of dependent variables distribution, skewness and kurtosis were investigated. Chi-square and t-test were used to compare variables between the two groups. Mauchly’s test was used to check the sphericity or equality of variance of the differences among the research variables levels; also, the M-box test was used to check the assumption of homogeneity of the covariance matrices; and the Leven’s test was used to check the equality of variances. To check the hypotheses, repeated measures analysis of variance (ANOVA) and Bonferroni post-hoc test were used. Data were analyzed in SPSS software version 26 at a significance level of 0.05.
Results
Out of 40 eligible patients, 17 were completed the study and were analysed. The Flow diagram of the study is shown in Figure 1.
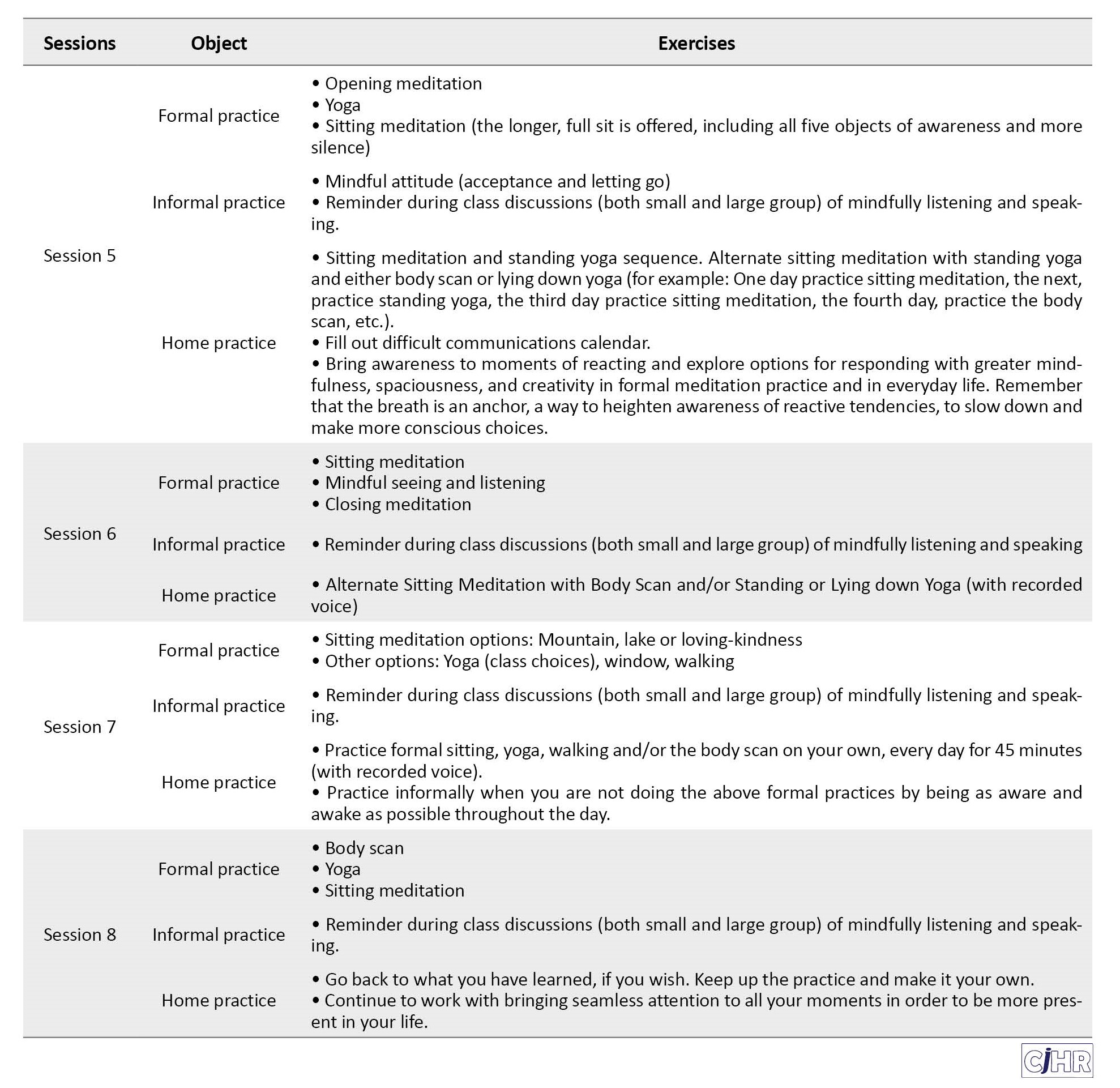
No significant difference was observed between the groups in terms of age (t=0.493, P=0.921), Gender (χ2=0.119, P=0.730), and body mass index (t=0.772, P=0.595). There was also no significant difference between the groups in terms of education level, marital status, employment status, smoking, exercise, duration of the disease and disease’ family history. Table 2, shows demographic variables of the study and Table 3 shows the descriptive information of the research variables.
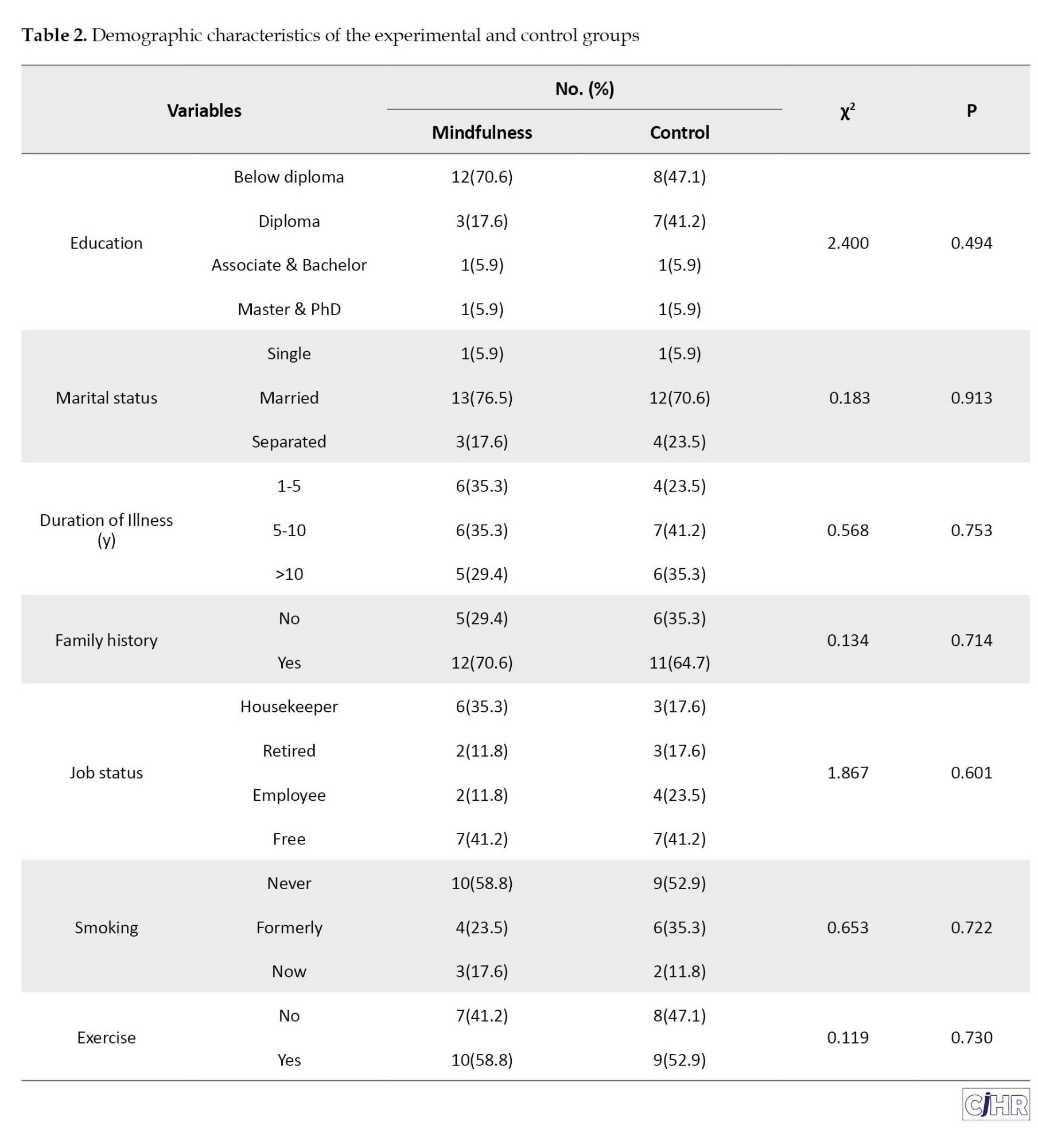
The findings showed that in the pre-test, there wasn’t a difference in the completed categories, between the MBSR group (2±0.485) and the control group (2.06±0.659). In the post-test, a significant difference in the completed categories was found between the MBSR (3.29±0.848) and the control group (2.18±0.636); which implies the MBSR group outperformed the control group in increasing completed categories. Finally, at the follow-up, all changes were still stable in the MBSR group (3.12±0.485) and the control group (2.12±0.600). In the pre-test, there wasn’t difference in the Perseverative errors, between the MBSR (30.06±6.60) and the control group (29.88±9.41); In the post-test, a significant difference in the Perseverative errors was found between the MBSR (20.94±5.71) and the control group (29.94±8.70); which implies the MBSR group outperformed the control group in decreasing Perseverative errors. Finally, at the follow-up design, all changes were still stable in the MBSR group (20.88±5.48) and the control group (29.41±8.08).
The degree of skewness and kurtosis of the research variables was in the range of 2 and -2, which indicates the normal distribution of the mentioned variables scores. The assumption of homogeneity of variance was met using Leven’s test in the post-test and follow-up phase (P>0.05). Considering the significance of the Mauchly’s test result, which indicates the heterogeneity of covariance matrix between the groups, the Greenhouse-Geisser correction was used. The observed interaction effect of group and time was significant for both components of completed categories (F=39.35, P=0.001) and perseverative errors (F=149.97, P=0.001) indicating a significant difference between the groups in terms of the mentioned variables at different times. Therefore, the results of each group was separately assessed over time. The results of pairwise comparison is shown in Table 4.
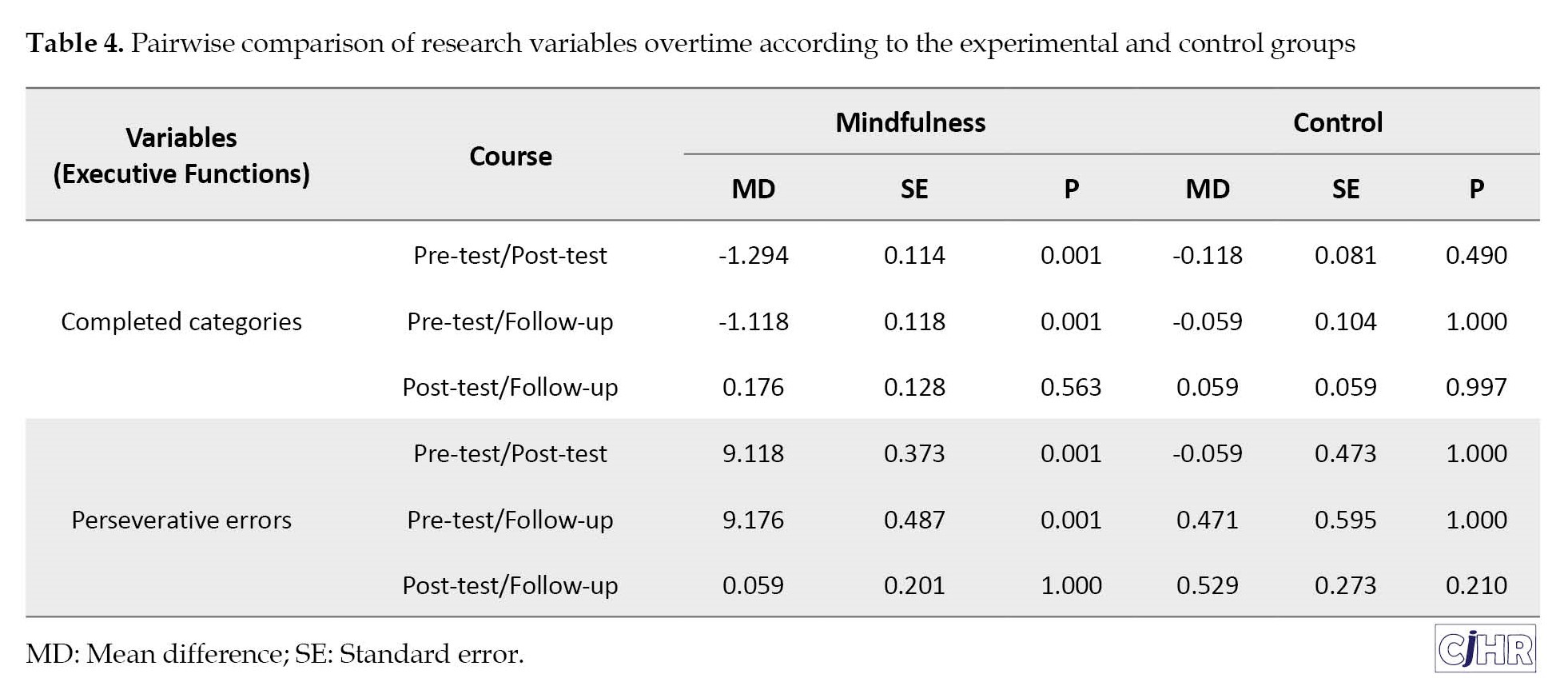
In the experimental group, the mean difference between pre-test and post-test, and between the pre-test and the follow-up for the completed categories’ component, has been reported as negative, which indicates a significant increase in the score of the completed categories of executive functions in the post-test and follow-up stages compared to the pre-test in the experimental group (P<0.001). Also, the average difference between pre-test and post-test, and between the pre-test and the follow-up, has been reported as positive for the perseverative errors’ component, which indicates a significant decrease in the score of perseverative errors of executive functions in the post-test and follow-up phases compared to the pre-test in the experimental group (P<0.001); while none of the mean differences in the control group were reported to be significant. Therefore, the research hypothesis was confirmed and MBSR was effective in improving executive functions in patients with hypertension.
Discussion
The purpose of this study was to investigate the effectiveness of mindfulness-based stress reduction (MBSR) on executive functions in patients with hypertension. Results indicated that MBSR significantly improved executive functions in patients with hypertension. In other words, MBSR increased the score of the completed categories, and decreased the score of perseverative errors of the participants in the experimental group. These results are consistent with the results of studies by Eskandari et al. (2022) [35], Shakib et al. (2021) [36], Dong et al. (2023) [19], Yousefi et al. (2023) [21], Ahmed Aboalola (2023) [20], and Zainal & Newman (2023) [17], which showed interventions based on mindfulness led to increasing and improving the executive functions in patients. Ahmed Aboalola’s (2023) study showed that it is possible to enhance executive function skills using mindfulness-based intervention in young with attention-deficit/ hyperactivity-disorder (ADHD) [20]. This result was confirmed in the study of Shakib et al. (2021) with the group of children with ADHD [36]. Also, Yousefi et al. (2023) [21] reported that MBSR was effective in promoting executive function in patients with rheumatoid arthritis; and Eskandari et al. (2022) showed the effectiveness of MBI on the executive functions of patients with multiple sclerosis [35]. Askari et al. (2023) [23], and Marciniak et al. (2020) [24], conveying inconsistent results with the present hypothesis, showed that MBSR had a minimal impact on cognition and reported no statistically significant difference. However, when describing their results, they mentioned the low adherence of their participants to home exercises.
In the explanation of the present hypothesis, the neurological mechanisms of the effect of MBIs are first discussed. For instance, Fornix, located at the mesial aspect of the cerebral hemispheres, connects several knots of the Limbic system and plays critical roles in cognition and episodic memory recall [37]. Polcari et al. (2022) reported that individuals under MBIs indicated increased axial diffusivity in the fornix-stria terminalis tract at the right side compared with the control group, which showed increased structural connectivity. Brain imaging also revealed a thicker corpus callosum in meditators, indicating greater structural connectivity [38]. Also, Sperduti et al. (2012) presented a meta-analysis study on brain regions activated during mindfulness training. They found that the basal ganglia, entorhinal cortex, and medial prefrontal cortex are important brain regions activated during mindfulness. These three regions are critical to the cognitive and emotional processes involved in mindfulness training. They found that when people are in a state of mindfulness, the basal ganglia can help inhibit irrelevant thoughts, the entorhinal cortex helps control mental state, and the medial prefrontal cortex helps increase emotional awareness [39]. All the mentioned cases such as memory, inhibitory control and self-awareness are dimensions of executive functions on which the effectiveness of mindfulness therapy was also shown in the present study.
According to a study by Laneri et al., (2016) MBI was related to structural changes in the cingulate because changes in white matter structure in the posterior cingulate cortex were observed in experienced meditators [40]; also, Tang et al. (2012) reported changes in white matter in the anterior cingulate cortex of experienced meditators, smokers, and healthy individuals who participated in MBIs [41]. Furthermore, studies on the electroencephalography of experienced meditators highlighted the creation of certain brain rhythms involved in consciousness and metacognitive perception, including changes in gamma waves, whose range primarily depends on the number of exercise hours [42].
In another explanation, MBI is a psychotherapy in which individuals learn the mental representation of issues in life that are beyond immediate human control through breathing, acceptance, and non-judgmental viewing [43]. In other words, response occurs when the mental pathways of response generation are sufficiently stimulated. Accordingly, reinvestment of non-automatic attention and non-habitual response, which can be facilitated by MBSR, is necessary for the improvement of MBSR tasks [36]. Another explanation is that according to the opinion of Muller et al., relaxation exercises improve the function of primary hormones (which play critical roles in the physiology of mood disorders) by improving the circulation in endocrine glands and indirectly affect executive functions by improving the mood [44]. According to the authors of this study, mindfulness exercises have a lot in common with executive functions; that is, in all mindfulness exercises, components of executive functions such as attention and working memory are involved. For example, the basic concepts of mindfulness therapy, i.e. explaining doing mode and being mode, teach the participant how to perform a non-automatic, conscious task; or in a body scan exercise, people pay attention to bodily sensations in different parts of the body, refocusing if they get distracted. Also, in breathing meditation, the focus is on breathing, and participants are encouraged to return to the practice of focusing on breathing with the concentration on the inhalation and exhalation of their breath if their mind distraction. In other exercises such as eating, seeing and hearing meditation, paying attention to experiences in the present moment and focused and expanded awareness is the basis of the work. And this is the skill that involves people’s executive functions when doing things. Therefore, as the muscles of the body gain more strength due to continuous exercises, it is not unlikely that frequent mindfulness exercises improve executive functions. In spite of conflicting findings, most of studies are generally well suggesting that MBSR can improve executive functions and cognitive aspects which have important roles in maintaining self-care and treatment adherence in chronic patients.
Conclusion
According to the results of this research, MBSR was effective on executive functions of patients with hypertension. Therefore, it is suggested that the mentioned intervention be used in medical centers to improve the cognitive activities of patients with hypertension.
The current research faced some limitations. Although we tried to comply with all of the clinical trial requirements, due to the special conditions of COVID-19, we were faced with a sample limitation and we used the Purposive sampling method (although the allocation of groups was random), so the small sample size and the non-random nature of the sampling may make it difficult to generalize the findings. The follow-up period was only two months which does not guarantee long-term sustainability. Another limitation of the present study was the lack of a comprehensive investigation on the type and dosage of the drugs used by the participants, which may cause significant and considerable effects on the executive and cognitive functions of the patients. With regard to the limitations of the current research, it is suggested to consider the mentioned cases in future researches.
Ethical Considerations
Compliance with ethical guidelines
This article was approved by Department of Psychology, Tabriz Branch, Islamic Azad University (Code: IR.IAU.TABRIZ.REC.1400.02) and was registered by the Iranian Clinical Trial System (IRCT) (Code: IRCT20210531051454N1).
Funding
This article was taken from a Phd dissertation of Fatemeh Rabipour, approved by Department of Psychology, Tabriz Branch, Islamic Azad University (Code: 97000615).
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank the participated in this study for their cooperation and the assistance of the members of the cardiovascular research canter and Heshmat Hospital in Rasht City, Iran.
References
The findings showed that in the pre-test, there wasn’t a difference in the completed categories, between the MBSR group (2±0.485) and the control group (2.06±0.659). In the post-test, a significant difference in the completed categories was found between the MBSR (3.29±0.848) and the control group (2.18±0.636); which implies the MBSR group outperformed the control group in increasing completed categories. Finally, at the follow-up, all changes were still stable in the MBSR group (3.12±0.485) and the control group (2.12±0.600). In the pre-test, there wasn’t difference in the Perseverative errors, between the MBSR (30.06±6.60) and the control group (29.88±9.41); In the post-test, a significant difference in the Perseverative errors was found between the MBSR (20.94±5.71) and the control group (29.94±8.70); which implies the MBSR group outperformed the control group in decreasing Perseverative errors. Finally, at the follow-up design, all changes were still stable in the MBSR group (20.88±5.48) and the control group (29.41±8.08).
The degree of skewness and kurtosis of the research variables was in the range of 2 and -2, which indicates the normal distribution of the mentioned variables scores. The assumption of homogeneity of variance was met using Leven’s test in the post-test and follow-up phase (P>0.05). Considering the significance of the Mauchly’s test result, which indicates the heterogeneity of covariance matrix between the groups, the Greenhouse-Geisser correction was used. The observed interaction effect of group and time was significant for both components of completed categories (F=39.35, P=0.001) and perseverative errors (F=149.97, P=0.001) indicating a significant difference between the groups in terms of the mentioned variables at different times. Therefore, the results of each group was separately assessed over time. The results of pairwise comparison is shown in Table 4.
In the experimental group, the mean difference between pre-test and post-test, and between the pre-test and the follow-up for the completed categories’ component, has been reported as negative, which indicates a significant increase in the score of the completed categories of executive functions in the post-test and follow-up stages compared to the pre-test in the experimental group (P<0.001). Also, the average difference between pre-test and post-test, and between the pre-test and the follow-up, has been reported as positive for the perseverative errors’ component, which indicates a significant decrease in the score of perseverative errors of executive functions in the post-test and follow-up phases compared to the pre-test in the experimental group (P<0.001); while none of the mean differences in the control group were reported to be significant. Therefore, the research hypothesis was confirmed and MBSR was effective in improving executive functions in patients with hypertension.
Discussion
The purpose of this study was to investigate the effectiveness of mindfulness-based stress reduction (MBSR) on executive functions in patients with hypertension. Results indicated that MBSR significantly improved executive functions in patients with hypertension. In other words, MBSR increased the score of the completed categories, and decreased the score of perseverative errors of the participants in the experimental group. These results are consistent with the results of studies by Eskandari et al. (2022) [35], Shakib et al. (2021) [36], Dong et al. (2023) [19], Yousefi et al. (2023) [21], Ahmed Aboalola (2023) [20], and Zainal & Newman (2023) [17], which showed interventions based on mindfulness led to increasing and improving the executive functions in patients. Ahmed Aboalola’s (2023) study showed that it is possible to enhance executive function skills using mindfulness-based intervention in young with attention-deficit/ hyperactivity-disorder (ADHD) [20]. This result was confirmed in the study of Shakib et al. (2021) with the group of children with ADHD [36]. Also, Yousefi et al. (2023) [21] reported that MBSR was effective in promoting executive function in patients with rheumatoid arthritis; and Eskandari et al. (2022) showed the effectiveness of MBI on the executive functions of patients with multiple sclerosis [35]. Askari et al. (2023) [23], and Marciniak et al. (2020) [24], conveying inconsistent results with the present hypothesis, showed that MBSR had a minimal impact on cognition and reported no statistically significant difference. However, when describing their results, they mentioned the low adherence of their participants to home exercises.
In the explanation of the present hypothesis, the neurological mechanisms of the effect of MBIs are first discussed. For instance, Fornix, located at the mesial aspect of the cerebral hemispheres, connects several knots of the Limbic system and plays critical roles in cognition and episodic memory recall [37]. Polcari et al. (2022) reported that individuals under MBIs indicated increased axial diffusivity in the fornix-stria terminalis tract at the right side compared with the control group, which showed increased structural connectivity. Brain imaging also revealed a thicker corpus callosum in meditators, indicating greater structural connectivity [38]. Also, Sperduti et al. (2012) presented a meta-analysis study on brain regions activated during mindfulness training. They found that the basal ganglia, entorhinal cortex, and medial prefrontal cortex are important brain regions activated during mindfulness. These three regions are critical to the cognitive and emotional processes involved in mindfulness training. They found that when people are in a state of mindfulness, the basal ganglia can help inhibit irrelevant thoughts, the entorhinal cortex helps control mental state, and the medial prefrontal cortex helps increase emotional awareness [39]. All the mentioned cases such as memory, inhibitory control and self-awareness are dimensions of executive functions on which the effectiveness of mindfulness therapy was also shown in the present study.
According to a study by Laneri et al., (2016) MBI was related to structural changes in the cingulate because changes in white matter structure in the posterior cingulate cortex were observed in experienced meditators [40]; also, Tang et al. (2012) reported changes in white matter in the anterior cingulate cortex of experienced meditators, smokers, and healthy individuals who participated in MBIs [41]. Furthermore, studies on the electroencephalography of experienced meditators highlighted the creation of certain brain rhythms involved in consciousness and metacognitive perception, including changes in gamma waves, whose range primarily depends on the number of exercise hours [42].
In another explanation, MBI is a psychotherapy in which individuals learn the mental representation of issues in life that are beyond immediate human control through breathing, acceptance, and non-judgmental viewing [43]. In other words, response occurs when the mental pathways of response generation are sufficiently stimulated. Accordingly, reinvestment of non-automatic attention and non-habitual response, which can be facilitated by MBSR, is necessary for the improvement of MBSR tasks [36]. Another explanation is that according to the opinion of Muller et al., relaxation exercises improve the function of primary hormones (which play critical roles in the physiology of mood disorders) by improving the circulation in endocrine glands and indirectly affect executive functions by improving the mood [44]. According to the authors of this study, mindfulness exercises have a lot in common with executive functions; that is, in all mindfulness exercises, components of executive functions such as attention and working memory are involved. For example, the basic concepts of mindfulness therapy, i.e. explaining doing mode and being mode, teach the participant how to perform a non-automatic, conscious task; or in a body scan exercise, people pay attention to bodily sensations in different parts of the body, refocusing if they get distracted. Also, in breathing meditation, the focus is on breathing, and participants are encouraged to return to the practice of focusing on breathing with the concentration on the inhalation and exhalation of their breath if their mind distraction. In other exercises such as eating, seeing and hearing meditation, paying attention to experiences in the present moment and focused and expanded awareness is the basis of the work. And this is the skill that involves people’s executive functions when doing things. Therefore, as the muscles of the body gain more strength due to continuous exercises, it is not unlikely that frequent mindfulness exercises improve executive functions. In spite of conflicting findings, most of studies are generally well suggesting that MBSR can improve executive functions and cognitive aspects which have important roles in maintaining self-care and treatment adherence in chronic patients.
Conclusion
According to the results of this research, MBSR was effective on executive functions of patients with hypertension. Therefore, it is suggested that the mentioned intervention be used in medical centers to improve the cognitive activities of patients with hypertension.
The current research faced some limitations. Although we tried to comply with all of the clinical trial requirements, due to the special conditions of COVID-19, we were faced with a sample limitation and we used the Purposive sampling method (although the allocation of groups was random), so the small sample size and the non-random nature of the sampling may make it difficult to generalize the findings. The follow-up period was only two months which does not guarantee long-term sustainability. Another limitation of the present study was the lack of a comprehensive investigation on the type and dosage of the drugs used by the participants, which may cause significant and considerable effects on the executive and cognitive functions of the patients. With regard to the limitations of the current research, it is suggested to consider the mentioned cases in future researches.
Ethical Considerations
Compliance with ethical guidelines
This article was approved by Department of Psychology, Tabriz Branch, Islamic Azad University (Code: IR.IAU.TABRIZ.REC.1400.02) and was registered by the Iranian Clinical Trial System (IRCT) (Code: IRCT20210531051454N1).
Funding
This article was taken from a Phd dissertation of Fatemeh Rabipour, approved by Department of Psychology, Tabriz Branch, Islamic Azad University (Code: 97000615).
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank the participated in this study for their cooperation and the assistance of the members of the cardiovascular research canter and Heshmat Hospital in Rasht City, Iran.
References
- Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020; 16(4):223-37. [DOI:10.1038/s41581-019-0244-2] [PMID]
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016; 388(10053):1659-724. [DOI:10.1016/S0140-6736(16)31679-8] [PMID]
- Rouhi Balasi L, Salari A, Emami Sigaroudi A, Ashouri A, Moaddab F, Zaer Sabet F, et al. The effects of illness perception on diet adherence in patients with hypertension. Caspian J Health Res. 2021; 6(2):65-72. [DOI:10.32598/cjhr.6.2.3]
- Mirzaei M, Mirzaei M, Bagheri B, Dehghani A. Awareness, treatment, and control of hypertension and related factors in adult Iranian population. BMC Public Health. 2020; 20(1):667. [DOI:10.1186/s12889-020-08831-1] [PMID]
- de Heus RAA, Tzourio C, Lee EJL, Opozda M, Vincent AD, Anstey KJ, et al. Association between blood pressure variability with dementia and cognitive impairment: A systematic review and meta-analysis. Hypertension. 2021; 78(5):1478-89. [DOI:10.1161/HYPERTENSIONAHA.121.17797] [PMID]
- Gutteridge DS, Tully PJ, Ghezzi ES, Jamadar S, Smith AE, Commerford T, et al. Blood pressure variability and structural brain changes: A systematic review. J Hypertens. 2022; 40(6):1060-70. [DOI:10.1097/HJH.0000000000003133] [PMID]
- Heizhati M, Wang L, Li N, Li M, Pan F, Yang Z, et al. Prevalence of mild cognitive impairment is higher in hypertensive population: A cross-sectional study in less developed northwest China. Medicine. 2020; 99(19):e19891. [DOI:10.1097/MD.0000000000019891] [PMID]
- Walker KA, Power MC, Gottesman RF. Defining the relationship between hypertension, cognitive decline, and dementia: A review. Curr Hypertens Rep. 2017; ;19(3):24. [DOI:10.1007/s11906-017-0724-3] [PMID]
- Kim Y, Lim JS, Oh MS, Yu KH, Lee JS, Park JH, et al. Blood pressure variability is related to faster cognitive decline in ischemic stroke patients: PICASSO subanalysis. Sci Rep. 2021; 11(1):5049. [DOI:10.1038/s41598-021-83945-z] [PMID]
- Hannawi Y, Yanek LR, Kral BG, Vaidya D, Becker LC, Becker DM, et al. Hypertension is associated with white matter disruption in apparently healthy middle-aged individuals. AJNR Am J Neuroradiol. 2018; 39(12):2243-8. [DOI:10.3174/ajnr.A5871] [PMID]
- Li C, Zhu Y, Ma Y, Hua R, Zhong B, Xie W. Association of cumulative blood pressure with cognitive decline, dementia, and mortality. J Am Coll Cardiol. 2022; 79(14):1321-35. [DOI:10.1016/j.jacc.2022.01.045] [PMID]
- Muela HC, Costa-Hong VA, Yassuda MS, Moraes NC, Memória CM, Macedo TA, et al. Impact of hypertension on cognitive performance in individuals with high level of education. Brain Nerves. 2017; 1(2):1-6. [Link]
- Stabouli S, Chrysaidou K, Kotsis V, Chainoglou N, Chatzipapa N, Gidaris D, et al. Central SBP and executive function in children and adolescents with primary and secondary hypertension. J Hypertens. 2020; 38(11):2176-84. [DOI:10.1097/HJH.0000000000002551] [PMID]
- Diamond A. Executive functions. Handb Clin Neurol. 2020; 173:225-40. [DOI:10.1016/B978-0-444-64150-2.00020-4] [PMID]
- Launer LJ, Ross GW, Petrovitch H, Masaki K, Foley D, White LR, et al. Midlife blood pressure and dementia: The Honolulu-Asia aging study. Neurobiol Aging. 2000; 21(1):49-55. [DOI:10.1016/S0197-4580(00)00096-8] [PMID]
- Liu L, Hayden KM, May NS, Haring B, Liu Z, Henderson VW, et al. Association between blood pressure levels and cognitive impairment in older women: A prospective analysis of the Women’s Health Initiative Memory Study. Lancet Healthy Longev. 2022; 3(1):42-53. [DOI:10.1016/S2666-7568(21)00283-X] [PMID]
- Zainal NH, Newman MG. Mindfulness enhances cognitive functioning: A meta-analysis of 111 randomized controlled trials. Health Psychol Rev. 2023; 17(4):1-27. [DOI:10.1080/17437199.2023.2248222] [PMID]
- Kabat-Zinn J. Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. Delta Trade Paperback/Bantam Del; 2005. [Link]
- Dong M, Li Y, Zhang Y. The effect of mindfulness training on executive function in youth with depression. Acta Psychol. 2023; 235:103888. [DOI:10.1016/j.actpsy.2023.103888] [PMID]
- Ahmed Aboalola N. The effectiveness of a mindfulness-based intervention on improving executive functions and reducing the symptoms of attention deficit hyperactivity disorder in young children. Appl Neuropsychol Child. 2023; 12(4):1-9. [DOI:10.1080/21622965.2023.2203321] [PMID]
- Yousefi S, Zanjani Z, Omidi A, Zamani B, Sayyah M. Comparison of mindfulness-based stress reduction therapy and cognitive-behavioral therapy of chronic fatigue, sleep quality, executive function and disease activity in patients with rheumatoid arthritis. J Contem Psychother. 2023; 53(2):173-80. [DOI:10.1007/s10879-022-09558-3]
- Loucks EB, Nardi WR, Gutman R, Kronish IM, Saadeh FB, Li Y, et al. Mindfulness-based blood pressure reduction (MB-BP): Stage 1 single-arm clinical trial. PloS One. 2019; 14(11):e0223095. [DOI:10.1371/journal.pone.0223095] [PMID]
- Askari S, Sotoudeh Asl N, Sabahi P, Ghorbani R. [Comparing the effectiveness of behavioral activation therapy with cognitive-behavioral therapy based on mindfulness on cognitive regulation of emotion and executive functions in people with obsessive-compulsive disorder (Persian)]. J Health Care. 2023; 24(4):342-54. [Link]
- Marciniak R, Šumec R, Vyhnálek M, Bendíčková K, Lázničková P, Forte G, et al. The effect of Mindfulness-Based Stress Reduction (MBSR) on depression, cognition, and immunity in mild cognitive impairment: A pilot feasibility study. Clin Interv Aging. 2020; 15:1365-81. [DOI:10.2147/CIA.S249196] [PMID]
- Valizadeh H, Ahmadi V. [Effectiveness of mindfulness-based therapy on sleep quality and death anxiety in the elderly with hypertension (Persian)]. J Caspian Health Aging. 2021; 6(2):71-84. [DOI:10.22088/cjhaa.6.2.7]
- Ponte Márquez PH, Feliu-Soler A, Solé-Villa MJ, Matas-Pericas L, Filella-Agullo D, Ruiz-Herrerias M, et al. Benefits of mindfulness meditation in reducing blood pressure and stress in patients with arterial hypertension. J Hum Hypertens. 2019; 33(3):237-47. [DOI:10.1038/s41371-018-0130-6] [PMID]
- An E, Irwin MR, Doering LV, Brecht ML, Watson KE, Corwin E, et al. Mindfulness effects on lifestyle behavior and blood pressure: A randomized controlled trial. Health Sci Rep. 2021; 4(2):e296. [DOI:10.1002/hsr2.296] [PMID]
- Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. Gen Hosp Psychiatry. 1982; 4(1):33-47. [DOI:10.1016/0163-8343(82)90026-3] [PMID]
- Santorelli S. Mindfulness-based stress reduction (MBSR): Standards of practice. The Center for Mindfulness in Medicine, Health Care & Society. Massachusetts: University of Massachusetts Medical School; 2014. [Link]
- Santorelli SF, Kabat-Zinn J, Blacker M, Meleo-Meyer F, Koerbel L. Mindfulness-based stress reduction (MBSR) authorized curriculum guide. Massachusetts: University of Massachusetts; 2017. [Link]
- Grant DA, Berg E. Wisconsin card sorting test. J Exp Psychol. 1948; 38(4):404. [DOI:10.1037/h0059831]
- Heaton RK, Staff P. Wisconsin card sorting test: Computer version 4. Odessa: Psychological Assessment Resources. 1993; 4:1-4. [Link]
- Shahgholian M, Azadfallah P, Fathi-Ashtiani A, Khodadadi M. [Design of the Wisconsin Card Sorting Test (WCST) computerized version: Theoretical fundamental, developing and psychometrics characteristics (Persian)]. Clin Psychol Stud. 2012; 1(4):110-34. [Link]
- Kopp B, Lange F, Steinke A. The reliability of the Wisconsin card sorting test in clinical practice. Assessment. 2021; 28(1):248-63. [PMID]
- Eskandari M, Raeisyan Zadeh F, Mehdikhani M. [Comparison of the effectiveness of mindfulness-based stress reduction and relaxation on executive functions in people with Multiple Sclerosis (MS) (Persian)]. Neuropsychology. 2022; 8(29):83-92. [DOI:10.30473/clpsy.2021.57814.1594]
- Shakib Z, Hajabi MZ, Aghayousefi AR. The effect of mindfulness-based intervention on executive functions (sustained attention, processing speed, response inhibition and working memory) in children with attention deficit / hyperactivity disorder. Islam Life Style. 2020; 4(4):125-33. [Link]
- Senova S, Fomenko A, Gondard E, Lozano AM. Anatomy and function of the fornix in the context of its potential as a therapeutic target. J Neurol Neurosurg Psychiatry. 2020; 91(5):547-59. [DOI:10.1136/jnnp-2019-322375] [PMID]
- Polcari JJ, Cali RJ, Nephew BC, Lu S, Rashkovskii M, Wu J, et al. Effects of the mindfulness-based blood pressure reduction (mb-bp) program on depression and neural structural connectivity. J Affect Disord. 2022; 311:31-9. [DOI:10.1016/j.jad.2022.05.059] [PMID]
- Sperduti M, Martinelli P, Piolino P. A neurocognitive model of meditation based on activation likelihood estimation (ALE) meta-analysis. Conscious Cogn. 2012 ; 21(1):269-76. [DOI:10. 1016/j. concog. 2011. 09. 019] [PMID]
- Laneri D, Schuster V, Dietsche B, Jansen A, Ott U, Sommer J. Effects of long-term mindfulness meditation on brain’s white matter microstructure and its aging. Front Aging Neurosci. 2016; 7:254. [DOI:10.3389/fnagi.2015.00254] [PMID]
- Tang YY, Lu Q, Fan M, Yang Y, Posner MI. Mechanisms of white matter changes induced by meditation. Proc Natl Acad Sci U S A. 2012; 109(26):10570-4. [DOI:10.1073/pnas.1207817109] [PMID]
- Ken Tanaka G, Russell TA, Bittencourt J, Marinho V, Teixeira S, Hugo Bastos V, et al. Open monitoring meditation alters the EEG gamma coherence in experts meditators: The expert practice exhibit greater right intra-hemispheric functional coupling. Conscious Cogn. 2022; 102:103354. [DOI:10.1016/j.concog.2022.103354] [PMID]
- Rabipour F, Hosseininasab SD, Salari A. [The effectiveness of mindfulness-based therapy on working memory indices in patients with hypertension: A randomized clinical trial (Persian)]. Feyz Med Sci J. 2023; 27(5):501-11. [Link]
- Müller C, Dubiel D, Kremeti E, Lieb M, Streicher E, Siakir Oglou N, et al. Effects of a single physical or mindfulness intervention on mood, attention, and executive functions: Results from two randomized controlled studies in University Classes. Mindfulness. 2021; 12(5):1282-93. [DOI:10.1007/s12671-021-01601-z]
Article Type: Original Contributions |
Subject:
Health Education and Promotion
Received: 2023/12/20 | Accepted: 2023/12/28 | Published: 2024/01/1
Received: 2023/12/20 | Accepted: 2023/12/28 | Published: 2024/01/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Contact Information
cjhr Office, Guilan University of Medical Sciences
P.O.Box 93345-41938, Rasht, Iran
Journal Tel: +9813 33335820
Publisher Tel: +9821 453 55 000
Email: cjhr.gums@gmail.com
