

Volume 9, Issue 1 (1-2024)
CJHR 2024, 9(1): 43-50 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghanbari R, Mojtahedi K, joukar F, Maroufizadeh S, Hassanipour S, Naghipour M, et al . Association between hypothyroidism and constipation: A cross- sectional study from the PERSIAN Guilan cohort study. CJHR 2024; 9 (1) :43-50
URL: http://cjhr.gums.ac.ir/article-1-350-en.html
URL: http://cjhr.gums.ac.ir/article-1-350-en.html
Reyhaneh Ghanbari1 
 , Kourosh Mojtahedi1 , Farahnaz Joukar1 , Saman Maroufizadeh2 , Soheil Hassanipour1 , Mohammadreza Naghipour1 , Sara Yeganeh1 , Fariborz Mansour-Ghanaei * 3
, Kourosh Mojtahedi1 , Farahnaz Joukar1 , Saman Maroufizadeh2 , Soheil Hassanipour1 , Mohammadreza Naghipour1 , Sara Yeganeh1 , Fariborz Mansour-Ghanaei * 3
, Kourosh Mojtahedi1 , Farahnaz Joukar1 , Saman Maroufizadeh2 , Soheil Hassanipour1 , Mohammadreza Naghipour1 , Sara Yeganeh1 , Fariborz Mansour-Ghanaei * 3
1- Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran.
2- Department of Biostatistics, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
3- Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran. , fmansourghanaei@gmail.com
2- Department of Biostatistics, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
3- Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran. , fmansourghanaei@gmail.com
Full-Text [PDF 520 kb]
(114 Downloads)
| Abstract (HTML) (208 Views)
Full-Text: (73 Views)
Introduction
Constipation is characterized by infrequent bowel movements, difficulty passing stools, firmness of stools, or incomplete and irregular bowel movements. It can occur idiopathically or as a secondary condition to other diseases, and is a common digestive disorder [1, 2].The Rome IV criteria are used to diagnose functional constipation [3, 4]. In Iran, the prevalence of constipation ranges from 1.4% to 37% in various studies [5]. Various factors are known to increase the risk of chronic constipation, including demographic and socio-economic factors, behavioral and lifestyle factors, as well as factors related to health status or underlying diseases [6, 7].
Among the demographic and socio-economic factors associated with constipation, we may list age, gender, income, level of education, residential status (urban or rural), and marital status, among which the most robust correlation with constipation is reported for the female gender. Regarding the relationship of other factors with constipation, various findings have been reported in different studies [6, 8]. Lifestyle factors that may potentially contribute to constipation include the level of physical activity, dietary habits (fiber and water intake), smoking, alcohol consumption, and medication use [9, 10]. Digestive diseases, endocrine disorders, neurological diseases, and medications can also be as risk factors [6, 7, 11]. Thyroid disorders, particularly hypothyroidism, can affect the movement of the digestive system [12, 13]. Studies comparing bowel movements or other bowel symptoms in euthyroid, hypothyroid, and hyperthyroid adult patients have produced varying results [14]. Physiological studies show changes in anorectal function in adult patients with hypothyroidism and hyperthyroidism, but findings regarding intestinal transit times or constipation symptoms are ambiguous [15-19].
Accoring to the literature reviewed by the authors, there are no studies on hypothyroidism status of individuals with constipation in Iran. Therefore, this study aimed to determine the relationship between constipation and hypothyroidism in the PERSIAN Guilan cohort study (PGCS).
Materials and Methods
Participants and study design
In this analytical cross-sectional study conducted in the PGCS, a subset of the PERSIAN cohort studies between the ages of 35 and 70 years, irrespective of gender, were included. The PGCS profile and PERSIAN protocol were previously published in detail [20, 21]. The process of inviting eligible families involved a two-stage approach. Firstly, a public invitation was extended to all individuals residing within the covered area, followed by a targeted visit to eligible households. Those who presented themselves at the Cohort Center of the Monastery were registered and their details were recorded in the admissions form. Subsequently, written informed consent was obtained from the referents. Exclusion criteria included inability to go to the clinic for a physical examination, mental retardation, and unwillingness to participate in the study. Individuals were divided into two groups based on their constipation status and compared with respect to the desired variables.
Study variables and data collection
Data were obtained by a questionnaire by a face-to-face interview with trained interviewers. Interviewers were proficient in the native language of the region, which facilitated communication with participants. The questionnaires were completed using dedicated online software that included demographic and clinical data: Age (year), gender (male, female), marital status (single, married, divorced, and widow), place of residence (rural, urban), education (years), employment status (employed or unemployed), wealth score index (WSI) was reported using the principal component analysis (PCA) [20]. In this study WSI categorized into three tertiles from poorest (1st tertile) to richest (3th tertile). Detailed explanation of the WSI calculation for participants were provided in previous studies from PERSIAN cohort [22, 23].
Life style data including body mass index (BMI), smoking and opium consumption (yes, no), alcohol user (yes, no), hookah (yes, no), non-steroidal anti-inflammatory drugs (NSAIDs) or antidepressants use (yes, no), Tea and coffee consumption (yes, no), fruit and vegetable consumption based on a daily intake. BMI was measured using weight in kilogram divided by height in square of meter and then categorized into normal weight, underweight, overweight, and obese for BMI levels of 18.5–24.9 kg/m2, <18.5 kg/m2, 25–29.9 kg/m2 and 30 kg/m2, respectively [24]. The measurement of physical activity was previously described in detail in previous studies from PERSIAN cohort [22, 25]. It was measured using metabolic equivalent rates (METs) which is a self-report instrument for measuring the activities of daily living [26] of participants of PERSIAN cohort using the questionnaire. Hypothyroidism was defined based on self-report of taking levothyroxine by individuals. The diagnosis of chronic constipation was based on the patient’s self-report. Constipation was defined as having fewer than three bowel movements per week based on the definition of the Mayo Clinic [27].
Statistical analysis
In this study, continuous variables were presented as Mean±SD and categorical variables as number (percentage). To determine whether those with and without constipation differ on demographic and clinical variables, χ2 test (or Cochran–Armitage test for trend) were conducted for categorical variables, and independent t-tests were used for continuous variables. The association of constipation with hypothyroidism was examined using logistic regression analysis. Odds ratio (OR) and 95% confidence interval (CI) were calculated. OR was also adjusted for demographic and clinical variables. In total, three models were run. Model 1 was unadjusted; model 2 was adjusted for age and sex; and model 3 was adjusted for variables in Model 2 plus marital status, years of education, occupation, place of residency, wealth score index (WSI), body mass index (BMI), physical activity, smoking, hookah smoking, drug consumption, alcohol consumption, tea and coffee consumption, NSAIDs and antidepressant drugs. Data analysis was performed using SPSS software, version 16 (SPSS Inc., Chicago, IL, USA), and a P<0.05 was considered statistically significant.
Results
Characteristics of the participants
Demographic and clinical characteristics of the participants are outlined in Table 1.
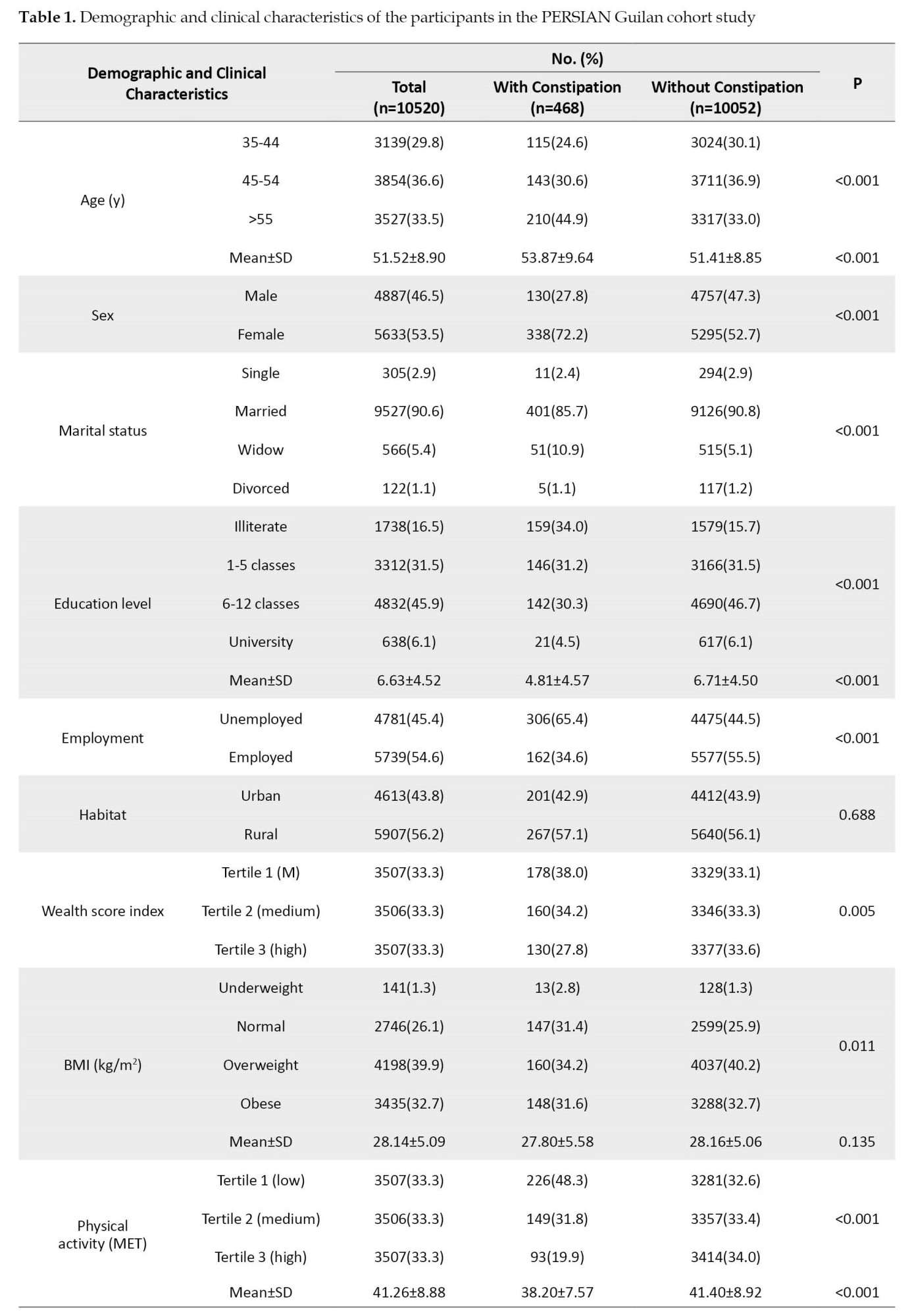
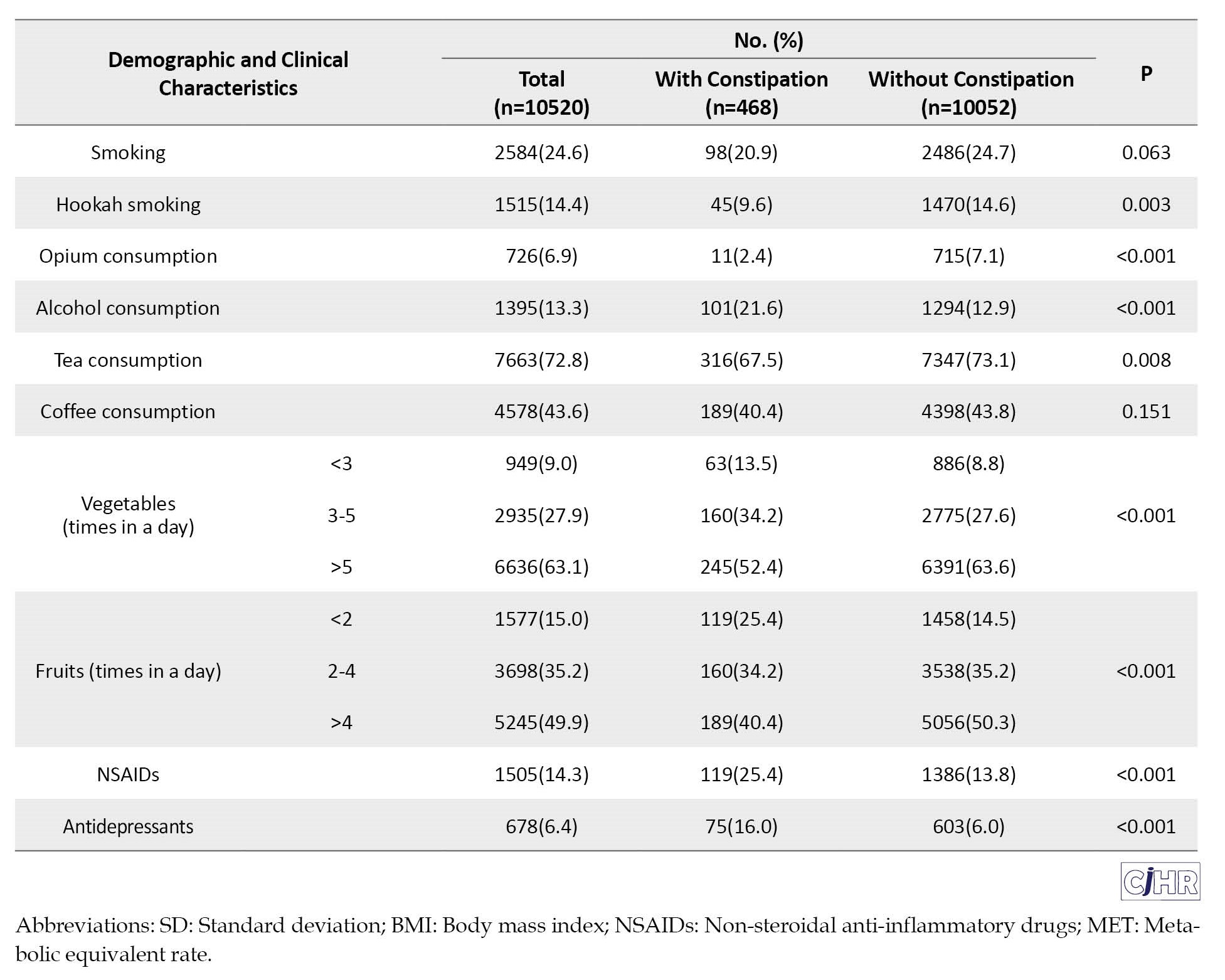
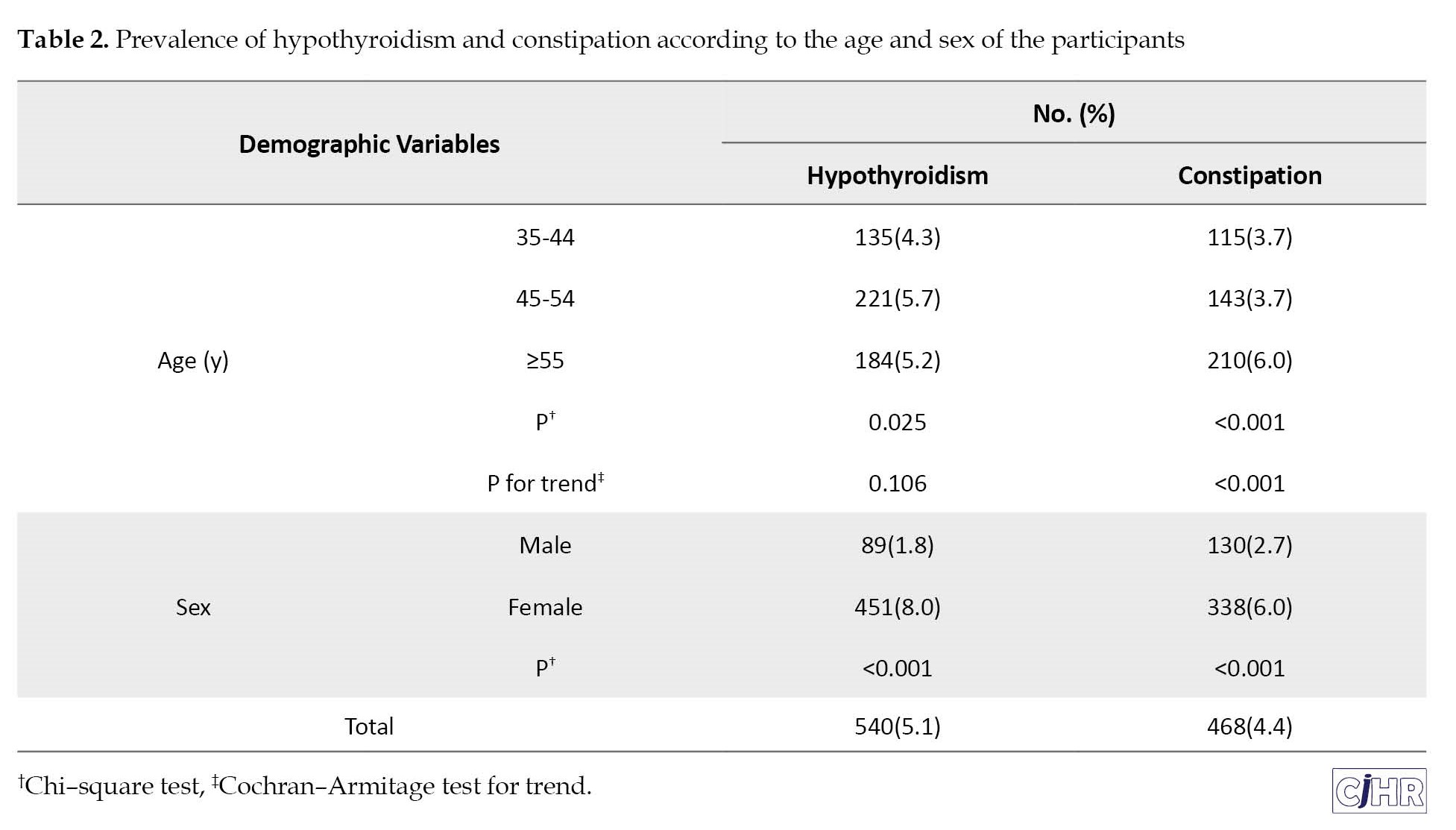
The mean age of the participants was 51.52±8.90 years. Of the participants, 53.5% were female, 90.6% were married, 6.1% had university education, 45.4% were unemployed, 56.2% wee resident in rural area, 32.7% had obese-BMI, 24.6% were smokers, and 13.3% consumed alcohol. Compared to participants without constipation, participants with constipation were older, more likely to be female, more widowed, more unemployed, had low WSI and low psychical activity and reported less consumption of hookah smoking and drug, more consumption of alcohol, low consumption of fruits and vegetables and more taking of NSAIDs and antidepressant drugs. The prevalence of hypothyroidism was 5.1% in the present study and was more prevalent in women than in men (8.0% vs 1.8%, P<0.001). The prevalence of hypothyroidism among participants aged 35-44 years was lower than those aged 45 or more years (P=0.025). The prevalence of constipation was 4.4% in the present study and was more common in women than in men (6.0% vs 2.7%, P<0.001). The prevalence of constipation increased with age: The highest was 6.0% in those aged 55 or more years (P for trend <0.001) (Table 2).
The prevalence of constipation was higher among participants with hypothyroidism than those without hypothyroidism, although this difference was not statistically significant (5.6% vs 4.4%, P=0.200). In unadjusted model (model 1), the presence of hypothyroidism increased the odds of constipation by 1.28-fold (95% CI, 0.88%, 1.87%), although this relationship was not statistically significant (P=0.201) (Table 3).
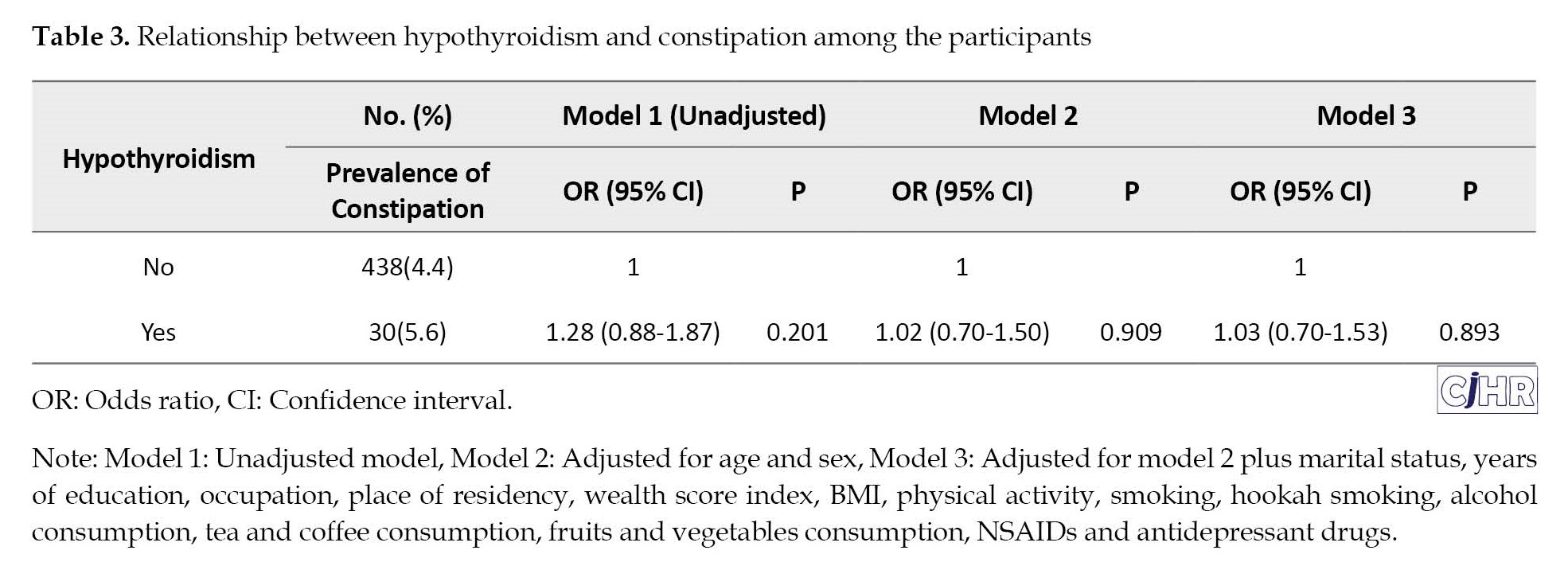
This association remained non-significant after adjusting for age and sex (OR=1.02, 95% CI, 0.70%, 1.50%). Similar result was obtained in fully adjusted model (Model 3) (OR=1.03, 95% CI, 0.70%, 1.53%) (Table 3).
Discussion
Constipation is a prevalent gastrointestinal ailment in the general population. Research comparing the frequency of bowel movements or other gastrointestinal symptoms in euthyroid, hypothyroid, and hyperthyroid adult patients has produced conflicting results. Physiological studies have demonstrated modified anorectal function in adult patients with hypothyroidism and hyperthyroidism, yet findings regarding intestinal transit times or constipation symptoms have been ambiguous. Hence, this study was carried out with the objective of ascertaining the correlation between constipation and hypothyroidism within the PGCS.
In this study, the prevalence of hypothyroidism and constipation was 5.1% and 4.4% respectively. The findings of this investigation revealed that compared to participants without constipation, participants with constipation were older, more likely to be female, more widowed, more unemployed, had low WSI and low psychical activity and reported less consumption of hookah smoking and drug, more consumption of alcohol, low consumption of fruits and vegetables and more use of NSAIDs and antidepressant drugs.
Regarding demographic and socio-economic factors linked to constipation, female gender has been reported to have the strongest correlation with constipation. Other studies have produced varying results regarding the relationship between constipation and these factors [6, 8]. The findings of this study are in line with those of previous research.
Based on the findings of this research, the incidence of constipation was more prevalent among individuals with hypothyroidism as compared to those without it, although this variance did not achieve statistical significance. In accordance with our investigation, Samei et al.’s research, through scrutinizing the incidence of hypothyroidism in children with persistent constipation, evinced that there is a correlation between hypothyroidism and constipation in minors [28]. Additionally, Deen et al.’s study demonstrated that 33% of hypothyroidism patients underwent symptoms of bowel dysfunction [29], which is in harmony with the findings of our investigation.
Kim et al.’s investigation evinced a 0.41% and 1.76% incidence of overt and subclinical hypothyroidism, respectively. The study demonstrated a negligible prevalence of overt and subclinical hypothyroidism in constipated patients. Thyroid function did not impinge upon colon transit time [30]. This contrasts with our research, which may be attributed to differences in the statistical population of the two studies.
In accordance with our findings, Yaylali et al.’s study aimed to scrutinize whether hypothyroidism results in gastrointestinal motor dysfunction. The investigation demonstrated that the average transit time of the esophagus and gastric emptying time in the hypothyroid group had increased by 30±4 minutes compared to the control group [31]. The study indicated that hypothyroidism significantly diminishes the motor activity of the esophagus and stomach, causing disruption in digestive function, sluggish movement, and ultimately leading to constipation. A constraint of this investigation was that the identification of hypothyroidism and constipation was reliant on self-reporting. While interviewer-patient relationships are typically intimate in cohort studies, conducting research based on TSH levels or Rome 4 criteria for constipation could provide a more precise assessment of this correlation. The limitation of this study is that the definition of hypothyroidism was based on taking drugs and the real hypothyroidism status was not detected based on TSH, T3, and T4 tests. Also, constipation was based on self-report.
Conclusion
The fundamental etiology of constipation in hypothyroidism arises from diminished gastrointestinal motility. Ordinarily, the colon’s musculature contracts to propel fecal matter through the intestines and into the rectum. However, in hypothyroidism, the muscles exhibit insufficient frequency and strength of contraction, resulting in sluggish stool transit through the colon. There was no significant statistical association between hypothyroidism and constipation in this study. Since nutrition and the type of fruits and vegetables and the type of substances consumed have an effective role in eliminating constipation, we recommend that these items be considered in future studies.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethical Committee of the Guilan University of Medical Sciences (Code: IR.GUMS.REC.1402.150), and all participants gave informed consent prior to their inclusion in the study.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization and supervision: Fariborz Mansour-Ghanaei and Farahnaz Joukar; Methodology: Mohammadreza Naghipour; Data collection: Fariborz Mansour-Ghanaei, Farahnaz Joukar and Soheil Hassanipour; Data analysis: Saman Maroufizade; Investigation and writing the original draft: Reyhaneh Ghanbari and Sara Yeganeh; Review & editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
We thank all subjects for participating in this study and the personnel of Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Science, for supporting this study.
Constipation is characterized by infrequent bowel movements, difficulty passing stools, firmness of stools, or incomplete and irregular bowel movements. It can occur idiopathically or as a secondary condition to other diseases, and is a common digestive disorder [1, 2].The Rome IV criteria are used to diagnose functional constipation [3, 4]. In Iran, the prevalence of constipation ranges from 1.4% to 37% in various studies [5]. Various factors are known to increase the risk of chronic constipation, including demographic and socio-economic factors, behavioral and lifestyle factors, as well as factors related to health status or underlying diseases [6, 7].
Among the demographic and socio-economic factors associated with constipation, we may list age, gender, income, level of education, residential status (urban or rural), and marital status, among which the most robust correlation with constipation is reported for the female gender. Regarding the relationship of other factors with constipation, various findings have been reported in different studies [6, 8]. Lifestyle factors that may potentially contribute to constipation include the level of physical activity, dietary habits (fiber and water intake), smoking, alcohol consumption, and medication use [9, 10]. Digestive diseases, endocrine disorders, neurological diseases, and medications can also be as risk factors [6, 7, 11]. Thyroid disorders, particularly hypothyroidism, can affect the movement of the digestive system [12, 13]. Studies comparing bowel movements or other bowel symptoms in euthyroid, hypothyroid, and hyperthyroid adult patients have produced varying results [14]. Physiological studies show changes in anorectal function in adult patients with hypothyroidism and hyperthyroidism, but findings regarding intestinal transit times or constipation symptoms are ambiguous [15-19].
Accoring to the literature reviewed by the authors, there are no studies on hypothyroidism status of individuals with constipation in Iran. Therefore, this study aimed to determine the relationship between constipation and hypothyroidism in the PERSIAN Guilan cohort study (PGCS).
Materials and Methods
Participants and study design
In this analytical cross-sectional study conducted in the PGCS, a subset of the PERSIAN cohort studies between the ages of 35 and 70 years, irrespective of gender, were included. The PGCS profile and PERSIAN protocol were previously published in detail [20, 21]. The process of inviting eligible families involved a two-stage approach. Firstly, a public invitation was extended to all individuals residing within the covered area, followed by a targeted visit to eligible households. Those who presented themselves at the Cohort Center of the Monastery were registered and their details were recorded in the admissions form. Subsequently, written informed consent was obtained from the referents. Exclusion criteria included inability to go to the clinic for a physical examination, mental retardation, and unwillingness to participate in the study. Individuals were divided into two groups based on their constipation status and compared with respect to the desired variables.
Study variables and data collection
Data were obtained by a questionnaire by a face-to-face interview with trained interviewers. Interviewers were proficient in the native language of the region, which facilitated communication with participants. The questionnaires were completed using dedicated online software that included demographic and clinical data: Age (year), gender (male, female), marital status (single, married, divorced, and widow), place of residence (rural, urban), education (years), employment status (employed or unemployed), wealth score index (WSI) was reported using the principal component analysis (PCA) [20]. In this study WSI categorized into three tertiles from poorest (1st tertile) to richest (3th tertile). Detailed explanation of the WSI calculation for participants were provided in previous studies from PERSIAN cohort [22, 23].
Life style data including body mass index (BMI), smoking and opium consumption (yes, no), alcohol user (yes, no), hookah (yes, no), non-steroidal anti-inflammatory drugs (NSAIDs) or antidepressants use (yes, no), Tea and coffee consumption (yes, no), fruit and vegetable consumption based on a daily intake. BMI was measured using weight in kilogram divided by height in square of meter and then categorized into normal weight, underweight, overweight, and obese for BMI levels of 18.5–24.9 kg/m2, <18.5 kg/m2, 25–29.9 kg/m2 and 30 kg/m2, respectively [24]. The measurement of physical activity was previously described in detail in previous studies from PERSIAN cohort [22, 25]. It was measured using metabolic equivalent rates (METs) which is a self-report instrument for measuring the activities of daily living [26] of participants of PERSIAN cohort using the questionnaire. Hypothyroidism was defined based on self-report of taking levothyroxine by individuals. The diagnosis of chronic constipation was based on the patient’s self-report. Constipation was defined as having fewer than three bowel movements per week based on the definition of the Mayo Clinic [27].
Statistical analysis
In this study, continuous variables were presented as Mean±SD and categorical variables as number (percentage). To determine whether those with and without constipation differ on demographic and clinical variables, χ2 test (or Cochran–Armitage test for trend) were conducted for categorical variables, and independent t-tests were used for continuous variables. The association of constipation with hypothyroidism was examined using logistic regression analysis. Odds ratio (OR) and 95% confidence interval (CI) were calculated. OR was also adjusted for demographic and clinical variables. In total, three models were run. Model 1 was unadjusted; model 2 was adjusted for age and sex; and model 3 was adjusted for variables in Model 2 plus marital status, years of education, occupation, place of residency, wealth score index (WSI), body mass index (BMI), physical activity, smoking, hookah smoking, drug consumption, alcohol consumption, tea and coffee consumption, NSAIDs and antidepressant drugs. Data analysis was performed using SPSS software, version 16 (SPSS Inc., Chicago, IL, USA), and a P<0.05 was considered statistically significant.
Results
Characteristics of the participants
Demographic and clinical characteristics of the participants are outlined in Table 1.
The mean age of the participants was 51.52±8.90 years. Of the participants, 53.5% were female, 90.6% were married, 6.1% had university education, 45.4% were unemployed, 56.2% wee resident in rural area, 32.7% had obese-BMI, 24.6% were smokers, and 13.3% consumed alcohol. Compared to participants without constipation, participants with constipation were older, more likely to be female, more widowed, more unemployed, had low WSI and low psychical activity and reported less consumption of hookah smoking and drug, more consumption of alcohol, low consumption of fruits and vegetables and more taking of NSAIDs and antidepressant drugs. The prevalence of hypothyroidism was 5.1% in the present study and was more prevalent in women than in men (8.0% vs 1.8%, P<0.001). The prevalence of hypothyroidism among participants aged 35-44 years was lower than those aged 45 or more years (P=0.025). The prevalence of constipation was 4.4% in the present study and was more common in women than in men (6.0% vs 2.7%, P<0.001). The prevalence of constipation increased with age: The highest was 6.0% in those aged 55 or more years (P for trend <0.001) (Table 2).
The prevalence of constipation was higher among participants with hypothyroidism than those without hypothyroidism, although this difference was not statistically significant (5.6% vs 4.4%, P=0.200). In unadjusted model (model 1), the presence of hypothyroidism increased the odds of constipation by 1.28-fold (95% CI, 0.88%, 1.87%), although this relationship was not statistically significant (P=0.201) (Table 3).
This association remained non-significant after adjusting for age and sex (OR=1.02, 95% CI, 0.70%, 1.50%). Similar result was obtained in fully adjusted model (Model 3) (OR=1.03, 95% CI, 0.70%, 1.53%) (Table 3).
Discussion
Constipation is a prevalent gastrointestinal ailment in the general population. Research comparing the frequency of bowel movements or other gastrointestinal symptoms in euthyroid, hypothyroid, and hyperthyroid adult patients has produced conflicting results. Physiological studies have demonstrated modified anorectal function in adult patients with hypothyroidism and hyperthyroidism, yet findings regarding intestinal transit times or constipation symptoms have been ambiguous. Hence, this study was carried out with the objective of ascertaining the correlation between constipation and hypothyroidism within the PGCS.
In this study, the prevalence of hypothyroidism and constipation was 5.1% and 4.4% respectively. The findings of this investigation revealed that compared to participants without constipation, participants with constipation were older, more likely to be female, more widowed, more unemployed, had low WSI and low psychical activity and reported less consumption of hookah smoking and drug, more consumption of alcohol, low consumption of fruits and vegetables and more use of NSAIDs and antidepressant drugs.
Regarding demographic and socio-economic factors linked to constipation, female gender has been reported to have the strongest correlation with constipation. Other studies have produced varying results regarding the relationship between constipation and these factors [6, 8]. The findings of this study are in line with those of previous research.
Based on the findings of this research, the incidence of constipation was more prevalent among individuals with hypothyroidism as compared to those without it, although this variance did not achieve statistical significance. In accordance with our investigation, Samei et al.’s research, through scrutinizing the incidence of hypothyroidism in children with persistent constipation, evinced that there is a correlation between hypothyroidism and constipation in minors [28]. Additionally, Deen et al.’s study demonstrated that 33% of hypothyroidism patients underwent symptoms of bowel dysfunction [29], which is in harmony with the findings of our investigation.
Kim et al.’s investigation evinced a 0.41% and 1.76% incidence of overt and subclinical hypothyroidism, respectively. The study demonstrated a negligible prevalence of overt and subclinical hypothyroidism in constipated patients. Thyroid function did not impinge upon colon transit time [30]. This contrasts with our research, which may be attributed to differences in the statistical population of the two studies.
In accordance with our findings, Yaylali et al.’s study aimed to scrutinize whether hypothyroidism results in gastrointestinal motor dysfunction. The investigation demonstrated that the average transit time of the esophagus and gastric emptying time in the hypothyroid group had increased by 30±4 minutes compared to the control group [31]. The study indicated that hypothyroidism significantly diminishes the motor activity of the esophagus and stomach, causing disruption in digestive function, sluggish movement, and ultimately leading to constipation. A constraint of this investigation was that the identification of hypothyroidism and constipation was reliant on self-reporting. While interviewer-patient relationships are typically intimate in cohort studies, conducting research based on TSH levels or Rome 4 criteria for constipation could provide a more precise assessment of this correlation. The limitation of this study is that the definition of hypothyroidism was based on taking drugs and the real hypothyroidism status was not detected based on TSH, T3, and T4 tests. Also, constipation was based on self-report.
Conclusion
The fundamental etiology of constipation in hypothyroidism arises from diminished gastrointestinal motility. Ordinarily, the colon’s musculature contracts to propel fecal matter through the intestines and into the rectum. However, in hypothyroidism, the muscles exhibit insufficient frequency and strength of contraction, resulting in sluggish stool transit through the colon. There was no significant statistical association between hypothyroidism and constipation in this study. Since nutrition and the type of fruits and vegetables and the type of substances consumed have an effective role in eliminating constipation, we recommend that these items be considered in future studies.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethical Committee of the Guilan University of Medical Sciences (Code: IR.GUMS.REC.1402.150), and all participants gave informed consent prior to their inclusion in the study.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization and supervision: Fariborz Mansour-Ghanaei and Farahnaz Joukar; Methodology: Mohammadreza Naghipour; Data collection: Fariborz Mansour-Ghanaei, Farahnaz Joukar and Soheil Hassanipour; Data analysis: Saman Maroufizade; Investigation and writing the original draft: Reyhaneh Ghanbari and Sara Yeganeh; Review & editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
We thank all subjects for participating in this study and the personnel of Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Science, for supporting this study.
References
- Bharucha AE, Pemberton JH, Locke GR. American gastroenterological association technical review on constipation. Gastroenterology. 2013; 144(1):218-38. [DOI:10.1053/j.gastro.2012.10.028]
- Luporini RL, Rizzo AL, Frizol SM, Luporini LD. Diagnosis and treatment of constipation: A clinical update based on the Rome IV criteria. J Coloproctol. 2020; 40(04):425-6. [DOI:10.1016/j.jcol.2020.06.004]
- Bharucha AE, Wald A. Chronic constipation. Mayo Clin Proc. 2019; 94(11):2340-57. [DOI:10.1016/j.mayocp.2019.01.031] [PMID]
- Oka P, Parr H, Barberio B, Black CJ, Savarino EV, Ford AC. Global prevalence of irritable bowel syndrome according to Rome III or IV criteria: A systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2020; 5(10):908-17. [DOI:10.1016/S2468-1253(20)30217-X] [PMID]
- Iraji N, Keshteli AH, Sadeghpour S, Daneshpajouhnejad P, Fazel M, Adibi P. Constipation in Iran: SEPAHAN systematic review No. 5. Int J Prev Med. 2012; 3(Suppl 1):S34-41. [PMID]
- Werth BL, Christopher SA. Potential risk factors for constipation in the community. World J Gastroenterol. 2021; 27(21):2795-817. [DOI:10.3748/wjg.v27.i21.2795] [PMID]
- Chen Z, Peng Y, Shi Q, Chen Y, Cao L, Jia J, et al. Prevalence and risk factors of functional constipation according to the Rome criteria in China: A systematic review and meta-analysis. Front Med (Lausanne). 2022; 9:815156. [DOI:10.3389/fmed.2022.815156] [PMID]
- McCrea GL, Miaskowski C, Stotts NA, Macera L, Varma MG. A review of the literature on gender and age differences in the prevalence and characteristics of constipation in North America. J Pain Symptom Manage. 2009; 37(4):737-45. [DOI:10.1016/j.jpainsymman.2008.04.016] [PMID]
- Anderson JW, Baird P, Davis RH Jr, Ferreri S, Knudtson M, Koraym A, et al. Health benefits of dietary fiber. Nutr Rev. 2009; 67(4):188-205. [DOI:10.1111/j.1753-4887.2009.00189.x] [PMID]
- Booth FW, Roberts CK, Laye MJ. Lack of exercise is a major cause of chronic diseases. Compr Physiol. 2012; 2(2):1143-211. [DOI:10.1002/cphy.c110025] [PMID]
- Talley NJ, Jones M, Nuyts G, Dubois D. Risk factors for chronic constipation based on a general practice sample. The Am J Gastroenterol. 2003; 98(5):1107-11. [DOI:10.1111/j.1572-0241.2003.07465.x] [PMID]
- Yarullina DR, Shafigullin MU, Sakulin KA, Arzamastseva AA, Shaidullov IF, Markelova MI, et al. Characterization of gut contractility and microbiota in patients with severe chronic constipation. PLoS One. 2020; 15(7):e0235985. [DOI:10.1371/journal.pone.0235985] [PMID]
- Zhao Q, Chen YY, Xu DQ, Yue SJ, Fu RJ, Yang J, et al. Action mode of gut motility, fluid and electrolyte transport in chronic constipation. Front Pharmacol. 2021; 12:630249. [DOI:10.3389/fphar.2021.630249] [PMID]
- Bennett WE Jr, Heuckeroth RO. Hypothyroidism is a rare cause of isolated constipationJ Pediatr Gastroenterol Nutr. 2012; 54(2):285-7. [DOI:10.1097/MPG.0b013e318239714f] [PMID]
- Mulhem E, Khondoker F, Kandiah S. Constipation in children and adolescents: Evaluation and treatment. Am Fam Physician. 2022; 105(5):469-78. [PMID]
- Sorouri M, Pourhoseingholi MA, Vahedi M, Safaee A, Moghimi-Dehkordi B, Pourhoseingholi A, et al. Functional bowel disorders in Iranian population using Rome III criteria.Saudi J Gastroenterol. 2010; 16(3):154-60. [DOI:10.4103/1319-3767.65183] [PMID]
- Zahedi MJ, Moghadam SD, Abbasi MH, Mirzaei SM. [The assessment prevalence of functional constipation and associated factors in adults: A community-based study from Kerman, Southeast, Iran (2011-2012) (Persian)]. Govaresh. 2014; 19(2):95-101. [Link]
- Moezi P, Salehi A, Molavi H, Poustchi H, Gandomkar A, Imanieh MH, et al. Prevalence of chronic constipation and its associated factors in pars cohort study: A study of 9000 adults in Southern Iran. Middle East J Dig Dis. 2018; 10(2):75-83.[DOI:10.15171/mejdd.2018.94] [PMID]
- Hassanzadeh-Keshteli A, Hashemi-Jazi MS, Dehestani B, Adibi P. [Epidemiology of constipation and functional constipation and their risk factors in Iranian population (Persian)]. J Isfahan Med School. 2016; 34(404):1282-9. [Link]
- Poustchi H, Eghtesad S, Kamangar F, Etemadi A, Keshtkar AA, Hekmatdoost A, et al. Prospective epidemiological research studies in Iran (the PERSIAN Cohort Study): Rationale, objectives, and design. Am J Epidemiol. 2018; 187(4):647-55. [DOI:10.1093/aje/kwx314] [PMID]
- Mansour-Ghanaei F, Joukar F, Naghipour MR, Sepanlou SG, Poustchi H, Mojtahedi K, et al. The PERSIAN Guilan cohort study (PGCS). Arch Iran Med. 2019; 22(1):39-45. [PMID]
- Kazemi Karyani A, Karmi Matin B, Soltani S, Rezaei S, Soofi M, Salimi Y, et al. Socioeconomic gradient in physical activity: Findings from the PERSIAN cohort study. BMC Public Health. 2019; 19(1):1312. [DOI:10.1186/s12889-019-7715-z] [PMID]
- Najafi F, Rezaei S, Hajizadeh M, Soofi M, Salimi Y, Kazemi Karyani A, et al. Decomposing socioeconomic inequality in dental caries in Iran: Cross-sectional results from the PERSIAN cohort study. Arch Public Health. 2020; 78:75. [DOI:10.1186/s13690-020-00457-4] [PMID]
- WHO. A healthy lifestyle - WHO recommendations. Geneva: World Health Organization; 2020. [Link]
- Najafi A, Safari-Faramani R, Selk-Ghaffari M, Najafi F, Ghafouri M, Darbandi M, et al. Comparison of the physical activity levels between shift workers and non-shift workers in a large-scale cross-sectional study in Iran. BMC Public Health. 2023; 23(1):2034. [DOI:10.1186/s12889-023-16895-y] [PMID]
- Jetté M, Sidney K, Blümchen G. Metabolic equivalents (METS) in exercise testing, exercise prescription, and evaluation of functional capacity. Clin Cardiol. 1990; 13(8):555-65. [DOI:10.1002/clc.4960130809] [PMID]
- No author. Constipation [Internet]. 2023 [Updated 2024 February]. Available from: [Link]
- Samei P, Talakesh H, Salehifard Jouneghani A, Khaledi Sardashti M. The overall prevalence of hypothyroidism in children suffering chronic constipation in Shahrekord in 2019. Int J Epidemiol Res. 2022; 9(3):139-41. [DOI:10.34172/ijer.2022.24]
- Deen KI, Seneviratne SL, de Silva HJ. Anorectal physiology and transit in patients with disorders of thyroid metabolism. J Gastroenterol Hepatol. 1999; 14(4):384-7. [DOI:10.1046/j.1440-1746.1999.01865.x] [PMID]
- Kim J, Myung SJ, Yang DH, Yoon IJ, Seo SY, Ku HS, et al. Clinical characteristics of constipation with Hypothyroidism. Intest Res. 2010; 8(1):48-57. [DOI:10.5217/ir.2010.8.1.48]
- Yaylali O, Kirac S, Yilmaz M, Akin F, Yuksel D, Demirkan N, et al. Does hypothyroidism affect gastrointestinal motility? Gastroenterol Res Pract. 2009; 2009:529802.[DOI:10.1155/2009/529802] [PMID]
Article Type: Original Contributions |
Subject:
Epidemiology
Received: 2023/12/13 | Accepted: 2023/12/20 | Published: 2024/01/1
Received: 2023/12/13 | Accepted: 2023/12/20 | Published: 2024/01/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Contact Information
cjhr Office, Guilan University of Medical Sciences
P.O.Box 93345-41938, Rasht, Iran
Journal Tel: +9813 33335820
Publisher Tel: +9821 453 55 000
Email: cjhr.gums@gmail.com
