

Volume 9, Issue 2 (4-2024)
CJHR 2024, 9(2): 105-114 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Madani S F, Farrokhzad P. Acceptance and Commitment Therapy on Caregiving Burden and Psychological Flexibility in Caregivers of Elderly With Alzheimer's Disease. CJHR 2024; 9 (2) :105-114
URL: http://cjhr.gums.ac.ir/article-1-351-en.html
URL: http://cjhr.gums.ac.ir/article-1-351-en.html



1- Department of Psychology, Faculty of Psychology and Educational Sciences, Roudehen Branch, Islamic Azad University, Tehran, Iran
2- Department of Psychology, Faculty of Psychology and Educational Sciences, Roudehen Branch, Islamic Azad University, Tehran, Iran ,dr.peahfarokhzad@gmail.com
2- Department of Psychology, Faculty of Psychology and Educational Sciences, Roudehen Branch, Islamic Azad University, Tehran, Iran ,
Keywords: Acceptance and Commitment Therapy, Caregiver burden, Psychological flexibility, caregivers, Aged patients with Alzheimer', s disease Alzheimer Disease
Full-Text [PDF 600 kb]
(651 Downloads)
| Abstract (HTML) (1587 Views)
Full-Text: (777 Views)
Introduction
Population aging is a progressive phenomenon in the 21st century. In 2020, the global population of individuals aged 65 and above was 727 million, predicted to double over the next 30 years. This growth in the number of older population is likely to increase age-related diseases, such as Alzheimer's. Alzheimer’s disease is a prevalent mental disorder among the aged [1]. Currently, there is no specific drug available for Alzheimer’s disease as it is irreversible. Its imaging manifestations include brain atrophy and shrinkage of the brain’s parenchyma, and its symptoms include memory loss, significant personality changes, and even severe conditions like mental decline and facial paralysis [2 ]. Previous studies have reported that family members are the primary caregivers for Alzheimer’s patients. As a result, these caregivers often face daily stresses that are either overlooked or dealt with through various coping techniques. However, coping mechanisms vary among individuals due to governmental resources, economic status, and cultural differences [3]. Caring for an Alzheimer’s patient is highly challenging, and a caregiver often needs to be available around the clock. Caregiver burden is one of the issues present in the care of Alzheimer’s patients [4]. Family caregivers often dedicate their time and efforts to meeting all the health and personal needs of Alzheimer’s patients. However, they often neglect their own physical and mental health, resulting in reporting high levels of stress that may lead to various illnesses and issues. Coping techniques assist caregivers in adapting and meeting care needs [5].
Psychological flexibility is a dynamic process that help individuals to be stay focused on their long-term goals and values even through tough times or facing unexpected challenges. It is associated with various mental health outcomes among patients, such as depression, anxiety, psychosis, epilepsy, and pain [6]. The families of Alzheimer’s patients face significant psychological and economic burdens as the quality of life of patients is severely threatened [7]. According to Jansen et al. caregivers with a higher level of psychological flexibility experience less distress [8]. Tan et al. found that psychological flexibility has a strong relationship with mindfulness, lower levels of caregiver burden, depressive and anxiety symptoms [6]. Psychological inflexibility remains a significant predictor of these outcomes. Therefore, intervention programs that increase caregiver awareness of their psychological state would be beneficial [7]. Lappalainen et al. suggest that psychological inflexibility is a common factor contributing to mental health problems among caregivers, even when considering other relevant variables [9]. Lappalainen et al.’s study also indicated that thought suppression and psychological inflexibility significantly explain symptoms of depression and anxiety among family caregivers and are closely related to quality of life [9]. These findings emphasize the importance of implementing acceptance-based strategies to address thought suppression and psychological inflexibility [6, 8, 9].
One of the central points of acceptance and commitment therapy (ACT) is the idea of psychological flexibility, which is the ability to be fully present in the moment and to feel the emotions one is experiencing [10]. For example, when caring for an aged Alzheimer’s patient who is highly sensitive to their surroundings, it is essential to validate any distressing feelings the caregiver might experience using ACT approach [11]. The primary goal of ACT is to foster psychological flexibility. This involves being fully present and taking action toward valued goals to increase psychological flexibility and reduce burden [10-12]. In a study conducted by Zhang et al. (2022), an online experimental ACT program was examined for family caregivers of dementia patients. They found a decrease in depressive symptoms, burden, and stress reactions to behavioral symptoms. Additionally, there was an increase in positive caregiving aspects and life quality. Specific interventions in ACT reduced cognitive fusion and psychological inflexibility, leading to improved quality of life based on personal values [10]. In a study conducted by Montaner et al. in 2022, they aimed to implement and evaluate the effectiveness of a 6-week ACT intervention. The intervention was aimed at reducing anxiety and job burnout in healthcare professionals who work with dementia patients. The study found significant reductions in emotional exhaustion and anxiety levels and increases in life satisfaction and personal success in the intervention group. These results were sustained in the 3-month and 12-month follow-up periods [12]. Another study by Mosher et al. (2022) found that ACT significantly reduced fatigue and caregiver burden in patients who have advanced gastrointestinal cancer [13].
According to the literature review conducted by the authors, there have been only a few studies examining the efficacy of acceptance and commitment-based treatment on care pressure. Conversely, psychological flexibility has captured the interest of numerous researchers. But the caregiver stress has been relatively overlooked in research, particularly in the context of Iran. Therefore, this study was aimed to investigate the effect of ACT on psychological flexibility and caregiver burden in caregivers of Alzheimer’s patients.
Materials and Methods
The current research was quasi-experimental, and the design was pre-test, post-test with a control group, and a 3-month follow-up). The statistical population consisted of caregivers of aged patients with Alzheimer’s at Dr. Vajieh Aghamolaei’s Neurology Clinic in the spring of 2023. In this study, 30 individuals were selected with the purposive sampling method according to the inclusion criteria.
To determine the sample size based on previous studies [14-16], 15 individuals per group were considered for efficacy studies. In the current study, 30 individuals were assigned to the experimental and control groups (n=15, for each group). The inclusion criteria for the study were an age range of 30 to 45 years, being married, having at least a high school diploma, scoring above average on the AAQ-2 questionnaire, scoring above average on the caregiver burden inventory (CBI) questionnaire, and individuals’ willingness to participate in the study. Exclusion criteria were unwillingness to participate at any treatment stage and absence from more than two intervention sessions.
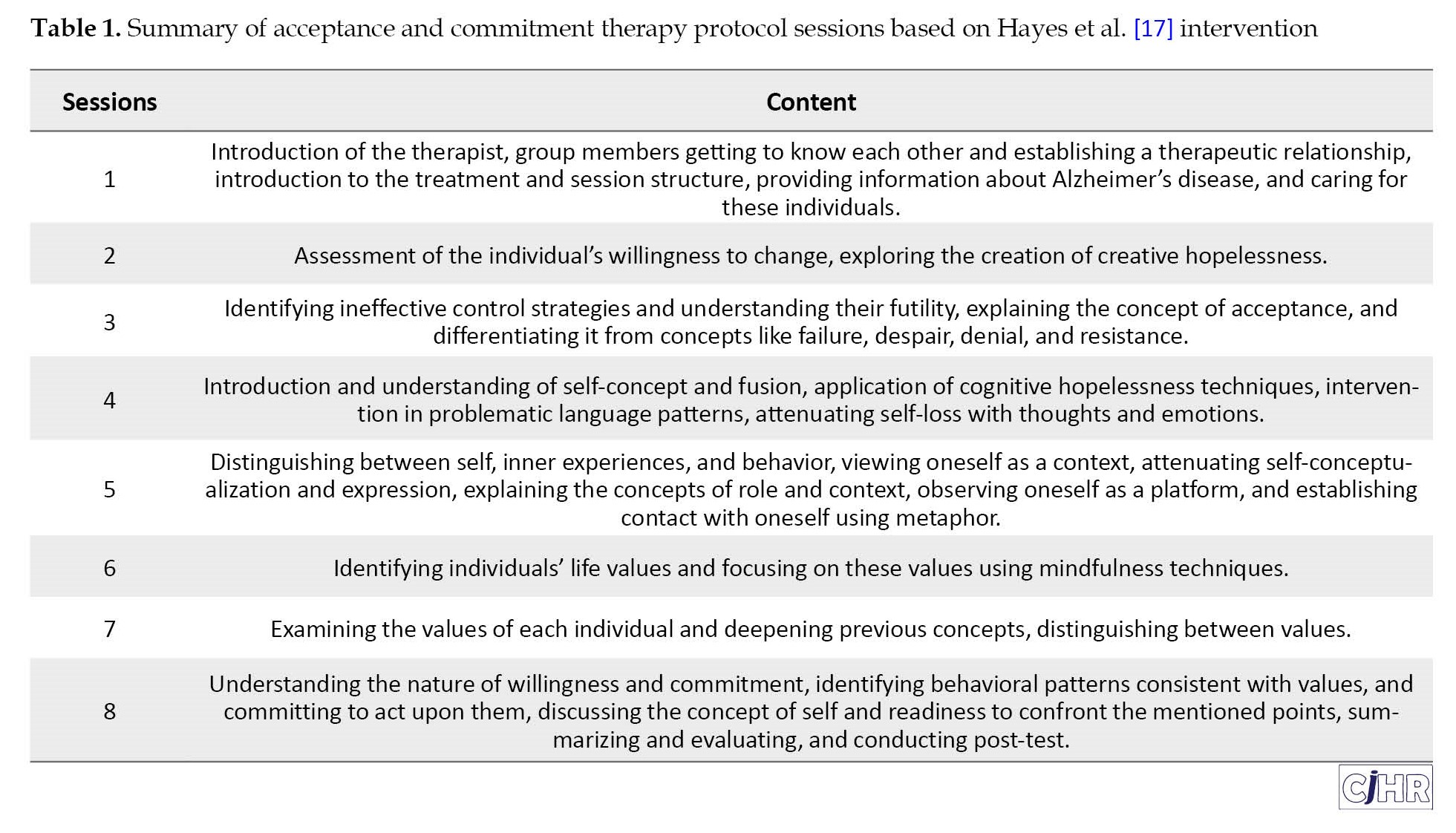
The process of collecting the study participants was carried out with permission from Dr. Aghamolaei’s Neurology Clinic. The ACT intervention [17] was implemented for the experimental group over eight sessions, each lasting 90 minutes, spanning eight consecutive weeks. The procedures and the required time were fully explained to the participants. Participants provided written informed consent to participate in the study. To maintain the privacy of individuals, the names of the participants were not mentioned in the questionnaires and reports, and the principle of confidentiality was observed. Participants were free to withdraw from the study at any time. Participants were informed that participation in the research would not impose any financial burden on them. They were also informed that the control group could benefit from the effective intervention at the end of the study. The summary of treatment sessions based on ACT is presented in Table 1.
Questionnaires
Acceptance and action questionnaire-II (AAQ-II)
The initial version of the AAQ-I was developed by Hayes et al. [17] was a 10-item scale that following psychometric evolution it was reduced to a 7-item scale with a 7-point Likert scale (1=never to 7=always). Items 2, 3, 4, 5, 7, 8, and 9 were reverse scored (1=always to 7=never), [17]. The items reflected either the likely dominance or non-dominance of private events (thoughts, feelings, and physiological sensations) in determining values-directed action [18]. This questionnaire measures psychological inflexibility, experiential avoidance, and acceptance. Higher total scores on the AAQ-II indicate higher psychological inflexibility, experiential avoidance, and more potential psychological distress. Lower total scores mean more psychological flexibility. A normative percentile is also presented, comparing the respondent’s score against a sample of normative undergraduates and adults [19]. A percentile of 50 indicates that the client has average (and healthy) levels of psychological flexibility and experiential avoidance. If the client scores 25 or above (percentile of approximately 86) then this is an indication that the client’s psychological inflexibility may impact their overall wellbeing. Cronbach’s α for various clinical and non-clinical groups has been reported to be between 0.78 and 0.88. The questionnaire has an internal consistency of 0.87 and a test re-test reliability of 0.80. Research findings have reported this tool’s reliability, validity, and satisfaction structure. The average alpha coefficient is 0.84, and the test re-test reliability is 0.80 for AAQ-II or the Persian version. Internal consistency ranged from 0.71 to 0.84 across four groups, with a total score of 0.89 [20].
Caregiver burden inventory (CBI)
The CBI was developed by Novak et al. to assess caregivers’ perceived objective and mental stress [21]. This test consists of 24 statements, and participants must indicate on a five-point Likert scale to what extent they experience each situation. The inventory measures caregiver burden across five dimensions: Time dependence burden (items 1 to 5), developmental burden (items 6 to 10), physical burden (items 11 to 14), social burden (items 15 to 19), and emotional burden (items 20 to 24). The total score ranges from 0 to 120, with higher scores indicating a more significant negative impact of caregiving on various aspects of the caregiver’s life. Cronbach’s α coefficients for the subscales ranged from 0.69 to 0.78; the entire inventory was reported as 0.87 [21]. Shafiezadeh et al. (2020) examined the validity and reliability of the Persian version of the CBI in 150 caregivers of Alzheimer’s patients. They obtained an internal consistency (Cronbach’s α) of 0.93 for the subscales. Additionally, the test re-test reliability coefficient using the intra-cluster correlation was 0.96 over a two-week interval [22].
Statistical analysis
In this research, descriptive criteria such as Mean±SD and confidence interval (CI) were used for descriptive statistics and covariance analysis for inferential statistics. The collected data were analyzed with chi-square test, repeated measures analysis of covariance at a significance level of 0.05 and SPSS software, version 27 was used for all statistical analyses. Kolmogorov-Smirnov test was used to evaluate normal distribution and Levene’s test was used to evaluate homogeneity of variances. Bonferroni’s post hoc test was also used to compare the means.
Results
The Mean±SD of the age of participants in the intervention group (20.35±1.90) were found to be significantly lower compared to the control group (36.40±3.62). Sixty percent vs 53% of the participants were female in the experimental and control groups, respectively. The majority of caregivers in both groups had a bachelor’s degree. There was no significant difference in terms of sex and educational level of the participants in the two groups. Table 2 shows demographic characteristics of the participants according to the two groups.

Table 3 shows that the average caregiving burden and its components and psychological flexibility have decreased in the ACT group in the post-test and follow-up stages compared to the pre-test.

Meanwhile, the control group’s average caregiving burden and psychological flexibility have remained relatively stable, with slight changes across the pre-test, post-test, and follow-up stages. Between-group difference of caregiving burden, time dependence burden, and physical burden was significant in all stages of the research (P<0.05). However, between-groups difference in developmental burden, social burden, emotional burden, and psychological flexibility was significant only in the post-test and follow-up stages of the research (P<0.001) while, there were no difference between the groups in the pre-test stages. Before running the statistical test, the researcher checked the research assumptions. The assumption of normality was not violated according to the Kolmogorov-Smirnov test. The homogeneity of variance assumption was also met according to the Levene’s test. In Table 3, the researcher examined the results of the analysis of the covariance test.
The group by time interaction tests are showing in Table 4.
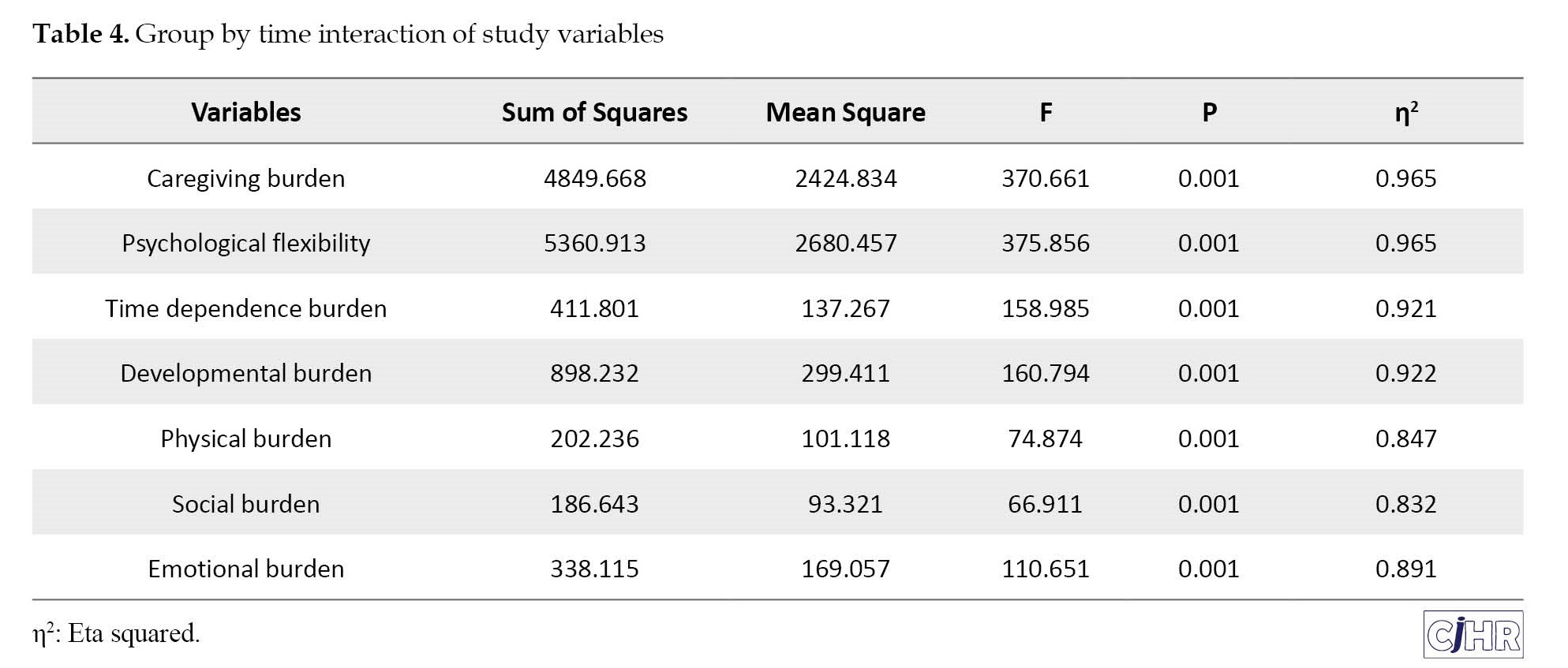
The interaction was significant for all variables. Therefore, the analysis was separately performed for each time point and the result are showing in Table 5.
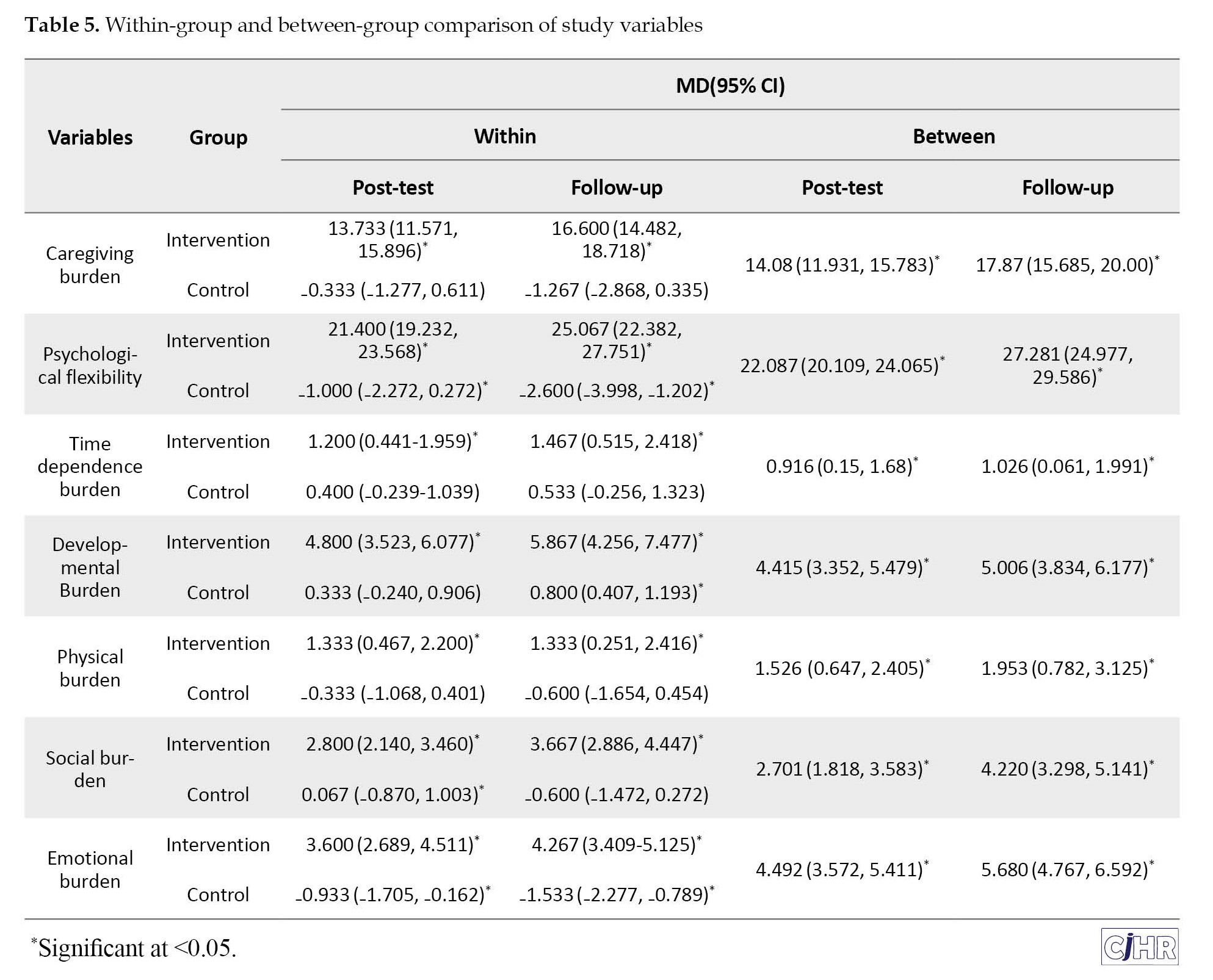
The within group difference of all variables from baseline to post-test and to follow-up was significant in the intervention group indicating an increase in scores of all variable over time. While, there was slight and non-significance changes over time in the control group. The between-group comparison also showed a significant difference between the two groups indicating improvement in the scores of study variables in the intervention compared to the control group. For example, the mean difference of caregiving burden from baseline to post-test in the intervention compared to the control group was 14.08 (95% CI, 11.93%-15.78%). The between-group difference was significant for all study variables.
Discussion
This study aimed to investigate the effectiveness of ACT on caregiver burden and psychological flexibility in caregivers of Alzheimer’s patients. The findings indicated that the ACT intervention (and its components) is effective for caregivers of Alzheimer’s patients. This finding is consistent with the research results of Lappalainen et al. [11], Zhang et al. [10], Montaner et al. [12], and Mosher et al. [13]. According to the current findings, Zhang et al. (2022) concluded that an online ACT program for family caregivers of dementia patients reduces depressive symptoms, burden, and stress reactions to behavioral symptoms while increasing positive caregiving aspects and quality of life [10]. Mosher et al. (2022) showed that ACT reduced fatigue in caregivers of advanced gastrointestinal cancer patients [13]. Montaner et al. (2022) explored the implementation and effectiveness of a 6-week ACT intervention for healthcare professionals who work with dementia patients. The aim was to reduce anxiety and burnout, as well as enhance psychological flexibility and life satisfaction. The researchers found that the intervention group showed significant decreases in emotional exhaustion and anxiety levels, along with an increase in life satisfaction and personal success. In addition, the intervention yielded reductions in job exhaustion and improvements in psychological flexibility. These results were maintained at the three and 12-month follow-up periods [23]. Fauth et al. (2022) carried out a research project to investigate the effectiveness of an online pilot program in utilizing ACT for family caregivers of individuals with dementia. The results showed that participants experienced reduced depressive symptoms, burden, and stress reactions to symptoms, along with increased positive aspects of care and quality of life, as measured through pre-test, post-test, and 4-week follow-up assessments. Specifically, participants showed improvements in cognitive dissonance, psychological inflexibility, and living according to personal values. All of these outcomes were statistically significant and sustained during the 4-week follow-up period [24].
It can be said that the evaluation of stressors determines their positive or negative outcomes [23, 24]. Identifying how maladaptive evaluations form, modifying them for compatibility, managing negative evaluations, and creating self-efficacy in managing complex thoughts are key intervention points for caregivers [25]. ACT is a valuable tool, facilitating the processing of complex thoughts (like negative stress evaluation) differently than many other psychosocial approaches. ACT helps caregivers overcome difficult emotions by teaching them to identify what is meaningful and align with their values. Clarifying values in areas such as mental health and interpersonal relationships, through acceptance and diffusion processes in ACT, enhances the social health dimensions of caregivers. Studies have also shown that ACT-based therapy is effective in reducing psychological disturbances (stress, depression and anxiety) and enhancing the physical and socio-psychological dimensions of patients, thus potentially impacting caregiver burden [26].
The research findings indicated that ACT intervention is effective in enhancing psychological flexibility in caregivers of Alzheimer’s patients. This finding is consistent with the results of Herbert & Forman [26], Aliakbari Dehkordi et al. [27], Zolfaghari et al. [28] and Fallah & Ghodsi [29]. According to the findings of Garivani and colleagues (2021) [30], commitment and acceptance-based therapy effectively increase psychological flexibility in mothers of children with tic disorders. Fallah & Ghodsi [29], in a sample study of 30 patients, demonstrated the effectiveness of ACT in increasing psychological flexibility in coronary artery disease patients [29]. Herbert and Forman’s study [26] indicated the effectiveness of ACT in enhancing psychological flexibility [26]. Feros and colleagues [31] showed that commitment and acceptance-based training improved psychological flexibility and acceptance of unpleasant thoughts in cancer patients [29]. Similarly, Wersebe and colleagues [32] showed with a sample of 91 individuals experiencing high work stress that ACT can increase psychological flexibility and reduce distress [32]. Psychological flexibility acts as a guiding force regulating emotional, cognitive, and behavioral domains. This primary indicator of emotional health positively influences emotional regulation, cognitive flexibility, behavioral adaptation, and the ability to change one’s mindset, enabling individuals to modify their behavior and reconcile with others [33].
Bennett-Levy et al. [34] stated that psychological flexibility can alter mindsets or behavioral sets when strategies threaten individual or social performance [34]. Psychological flexibility maintains a balance between essential life domains and the ability to be mindful, accepting, and committed to behaviors that deeply align with values. Therefore, as an educational approach, acceptance and commitment-based interventions focus on creating psychological flexibility through meaningful cognitive roles, valuable language, and structured timing [34]. This intervention and approach do not examine thoughts and feelings from a cognitive-behavioral perspective but delve into strategies for processing personal experiences. During the ACT process, caregivers learn to enjoy life despite its challenges and find meaning while being satisfied with themselves [36]. This approach emphasizes that challenges and engagement with beliefs should be reduced since the struggle with thoughts or emotions exacerbates problems [17].
The limitations of the current study that need to be mentioned are: Non-random sampling, the measurement tool for the study’s dependent variables was a questionnaire, which may introduce response bias. The sample of this study was limited to individuals aged 30 to 45 in Tehran, making it challenging to generalize the results. The role of caregivers in the patient’s life was not addressed, and the severity levels of Alzheimer’s disease among the participants were not considered. Consequently, the caregiving burden experienced by informal caregivers might differ.
To address these research limitations and obtain more accurate results, it is recommended to utilize other methods, such as clinical interviews, to gather more accurate information and reduce measurement error of dependent variables. Conduct similar studies on other age groups and compare their results with this study. Given the limited sample size of this study, it should be replicated with larger sample sizes to ensure the results’ generalizability. Similar studies should be conducted on caregivers of other chronic illnesses, and their results should be compared with this study. The role of caregivers in the patient’s life should be considered in future research, and the severity levels of Alzheimer’s disease among the participants should be evaluated and distinguished.
Conclusion
Given that the effectiveness of ACT on caregiving burden and psychological flexibility in caregivers of aged Alzheimer’s patients has been confirmed in the present study, and since many family caregivers report that available resources do not sufficiently meet their wishes or needs, clinical psychologists and health professionals are recommended to support caregivers in their roles better and enhance their mental well-being through intervention programs focused on compassion so that they can be more effective in accompanying the treatment process of Alzheimer’s patients.
Ethical Considerations
Compliance with ethical guidelines
The present study was approved by Ethics Committee of Islamic Azad University, Roudehen Branch (Code: IR.IAU.R.REC.1402.019).
Funding
The paper was extracted from the master's thesis of Seyed Farzan Madani, approved by Islamic Azad University, Roudehen Branch.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The completion of this study would not have been possible without the dedication and hard work of numerous individuals. Their contributions and support have been invaluable.
References
Population aging is a progressive phenomenon in the 21st century. In 2020, the global population of individuals aged 65 and above was 727 million, predicted to double over the next 30 years. This growth in the number of older population is likely to increase age-related diseases, such as Alzheimer's. Alzheimer’s disease is a prevalent mental disorder among the aged [1]. Currently, there is no specific drug available for Alzheimer’s disease as it is irreversible. Its imaging manifestations include brain atrophy and shrinkage of the brain’s parenchyma, and its symptoms include memory loss, significant personality changes, and even severe conditions like mental decline and facial paralysis [2 ]. Previous studies have reported that family members are the primary caregivers for Alzheimer’s patients. As a result, these caregivers often face daily stresses that are either overlooked or dealt with through various coping techniques. However, coping mechanisms vary among individuals due to governmental resources, economic status, and cultural differences [3]. Caring for an Alzheimer’s patient is highly challenging, and a caregiver often needs to be available around the clock. Caregiver burden is one of the issues present in the care of Alzheimer’s patients [4]. Family caregivers often dedicate their time and efforts to meeting all the health and personal needs of Alzheimer’s patients. However, they often neglect their own physical and mental health, resulting in reporting high levels of stress that may lead to various illnesses and issues. Coping techniques assist caregivers in adapting and meeting care needs [5].
Psychological flexibility is a dynamic process that help individuals to be stay focused on their long-term goals and values even through tough times or facing unexpected challenges. It is associated with various mental health outcomes among patients, such as depression, anxiety, psychosis, epilepsy, and pain [6]. The families of Alzheimer’s patients face significant psychological and economic burdens as the quality of life of patients is severely threatened [7]. According to Jansen et al. caregivers with a higher level of psychological flexibility experience less distress [8]. Tan et al. found that psychological flexibility has a strong relationship with mindfulness, lower levels of caregiver burden, depressive and anxiety symptoms [6]. Psychological inflexibility remains a significant predictor of these outcomes. Therefore, intervention programs that increase caregiver awareness of their psychological state would be beneficial [7]. Lappalainen et al. suggest that psychological inflexibility is a common factor contributing to mental health problems among caregivers, even when considering other relevant variables [9]. Lappalainen et al.’s study also indicated that thought suppression and psychological inflexibility significantly explain symptoms of depression and anxiety among family caregivers and are closely related to quality of life [9]. These findings emphasize the importance of implementing acceptance-based strategies to address thought suppression and psychological inflexibility [6, 8, 9].
One of the central points of acceptance and commitment therapy (ACT) is the idea of psychological flexibility, which is the ability to be fully present in the moment and to feel the emotions one is experiencing [10]. For example, when caring for an aged Alzheimer’s patient who is highly sensitive to their surroundings, it is essential to validate any distressing feelings the caregiver might experience using ACT approach [11]. The primary goal of ACT is to foster psychological flexibility. This involves being fully present and taking action toward valued goals to increase psychological flexibility and reduce burden [10-12]. In a study conducted by Zhang et al. (2022), an online experimental ACT program was examined for family caregivers of dementia patients. They found a decrease in depressive symptoms, burden, and stress reactions to behavioral symptoms. Additionally, there was an increase in positive caregiving aspects and life quality. Specific interventions in ACT reduced cognitive fusion and psychological inflexibility, leading to improved quality of life based on personal values [10]. In a study conducted by Montaner et al. in 2022, they aimed to implement and evaluate the effectiveness of a 6-week ACT intervention. The intervention was aimed at reducing anxiety and job burnout in healthcare professionals who work with dementia patients. The study found significant reductions in emotional exhaustion and anxiety levels and increases in life satisfaction and personal success in the intervention group. These results were sustained in the 3-month and 12-month follow-up periods [12]. Another study by Mosher et al. (2022) found that ACT significantly reduced fatigue and caregiver burden in patients who have advanced gastrointestinal cancer [13].
According to the literature review conducted by the authors, there have been only a few studies examining the efficacy of acceptance and commitment-based treatment on care pressure. Conversely, psychological flexibility has captured the interest of numerous researchers. But the caregiver stress has been relatively overlooked in research, particularly in the context of Iran. Therefore, this study was aimed to investigate the effect of ACT on psychological flexibility and caregiver burden in caregivers of Alzheimer’s patients.
Materials and Methods
The current research was quasi-experimental, and the design was pre-test, post-test with a control group, and a 3-month follow-up). The statistical population consisted of caregivers of aged patients with Alzheimer’s at Dr. Vajieh Aghamolaei’s Neurology Clinic in the spring of 2023. In this study, 30 individuals were selected with the purposive sampling method according to the inclusion criteria.
To determine the sample size based on previous studies [14-16], 15 individuals per group were considered for efficacy studies. In the current study, 30 individuals were assigned to the experimental and control groups (n=15, for each group). The inclusion criteria for the study were an age range of 30 to 45 years, being married, having at least a high school diploma, scoring above average on the AAQ-2 questionnaire, scoring above average on the caregiver burden inventory (CBI) questionnaire, and individuals’ willingness to participate in the study. Exclusion criteria were unwillingness to participate at any treatment stage and absence from more than two intervention sessions.
The process of collecting the study participants was carried out with permission from Dr. Aghamolaei’s Neurology Clinic. The ACT intervention [17] was implemented for the experimental group over eight sessions, each lasting 90 minutes, spanning eight consecutive weeks. The procedures and the required time were fully explained to the participants. Participants provided written informed consent to participate in the study. To maintain the privacy of individuals, the names of the participants were not mentioned in the questionnaires and reports, and the principle of confidentiality was observed. Participants were free to withdraw from the study at any time. Participants were informed that participation in the research would not impose any financial burden on them. They were also informed that the control group could benefit from the effective intervention at the end of the study. The summary of treatment sessions based on ACT is presented in Table 1.
Questionnaires
Acceptance and action questionnaire-II (AAQ-II)
The initial version of the AAQ-I was developed by Hayes et al. [17] was a 10-item scale that following psychometric evolution it was reduced to a 7-item scale with a 7-point Likert scale (1=never to 7=always). Items 2, 3, 4, 5, 7, 8, and 9 were reverse scored (1=always to 7=never), [17]. The items reflected either the likely dominance or non-dominance of private events (thoughts, feelings, and physiological sensations) in determining values-directed action [18]. This questionnaire measures psychological inflexibility, experiential avoidance, and acceptance. Higher total scores on the AAQ-II indicate higher psychological inflexibility, experiential avoidance, and more potential psychological distress. Lower total scores mean more psychological flexibility. A normative percentile is also presented, comparing the respondent’s score against a sample of normative undergraduates and adults [19]. A percentile of 50 indicates that the client has average (and healthy) levels of psychological flexibility and experiential avoidance. If the client scores 25 or above (percentile of approximately 86) then this is an indication that the client’s psychological inflexibility may impact their overall wellbeing. Cronbach’s α for various clinical and non-clinical groups has been reported to be between 0.78 and 0.88. The questionnaire has an internal consistency of 0.87 and a test re-test reliability of 0.80. Research findings have reported this tool’s reliability, validity, and satisfaction structure. The average alpha coefficient is 0.84, and the test re-test reliability is 0.80 for AAQ-II or the Persian version. Internal consistency ranged from 0.71 to 0.84 across four groups, with a total score of 0.89 [20].
Caregiver burden inventory (CBI)
The CBI was developed by Novak et al. to assess caregivers’ perceived objective and mental stress [21]. This test consists of 24 statements, and participants must indicate on a five-point Likert scale to what extent they experience each situation. The inventory measures caregiver burden across five dimensions: Time dependence burden (items 1 to 5), developmental burden (items 6 to 10), physical burden (items 11 to 14), social burden (items 15 to 19), and emotional burden (items 20 to 24). The total score ranges from 0 to 120, with higher scores indicating a more significant negative impact of caregiving on various aspects of the caregiver’s life. Cronbach’s α coefficients for the subscales ranged from 0.69 to 0.78; the entire inventory was reported as 0.87 [21]. Shafiezadeh et al. (2020) examined the validity and reliability of the Persian version of the CBI in 150 caregivers of Alzheimer’s patients. They obtained an internal consistency (Cronbach’s α) of 0.93 for the subscales. Additionally, the test re-test reliability coefficient using the intra-cluster correlation was 0.96 over a two-week interval [22].
Statistical analysis
In this research, descriptive criteria such as Mean±SD and confidence interval (CI) were used for descriptive statistics and covariance analysis for inferential statistics. The collected data were analyzed with chi-square test, repeated measures analysis of covariance at a significance level of 0.05 and SPSS software, version 27 was used for all statistical analyses. Kolmogorov-Smirnov test was used to evaluate normal distribution and Levene’s test was used to evaluate homogeneity of variances. Bonferroni’s post hoc test was also used to compare the means.
Results
The Mean±SD of the age of participants in the intervention group (20.35±1.90) were found to be significantly lower compared to the control group (36.40±3.62). Sixty percent vs 53% of the participants were female in the experimental and control groups, respectively. The majority of caregivers in both groups had a bachelor’s degree. There was no significant difference in terms of sex and educational level of the participants in the two groups. Table 2 shows demographic characteristics of the participants according to the two groups.
Table 3 shows that the average caregiving burden and its components and psychological flexibility have decreased in the ACT group in the post-test and follow-up stages compared to the pre-test.
Meanwhile, the control group’s average caregiving burden and psychological flexibility have remained relatively stable, with slight changes across the pre-test, post-test, and follow-up stages. Between-group difference of caregiving burden, time dependence burden, and physical burden was significant in all stages of the research (P<0.05). However, between-groups difference in developmental burden, social burden, emotional burden, and psychological flexibility was significant only in the post-test and follow-up stages of the research (P<0.001) while, there were no difference between the groups in the pre-test stages. Before running the statistical test, the researcher checked the research assumptions. The assumption of normality was not violated according to the Kolmogorov-Smirnov test. The homogeneity of variance assumption was also met according to the Levene’s test. In Table 3, the researcher examined the results of the analysis of the covariance test.
The group by time interaction tests are showing in Table 4.
The interaction was significant for all variables. Therefore, the analysis was separately performed for each time point and the result are showing in Table 5.
The within group difference of all variables from baseline to post-test and to follow-up was significant in the intervention group indicating an increase in scores of all variable over time. While, there was slight and non-significance changes over time in the control group. The between-group comparison also showed a significant difference between the two groups indicating improvement in the scores of study variables in the intervention compared to the control group. For example, the mean difference of caregiving burden from baseline to post-test in the intervention compared to the control group was 14.08 (95% CI, 11.93%-15.78%). The between-group difference was significant for all study variables.
Discussion
This study aimed to investigate the effectiveness of ACT on caregiver burden and psychological flexibility in caregivers of Alzheimer’s patients. The findings indicated that the ACT intervention (and its components) is effective for caregivers of Alzheimer’s patients. This finding is consistent with the research results of Lappalainen et al. [11], Zhang et al. [10], Montaner et al. [12], and Mosher et al. [13]. According to the current findings, Zhang et al. (2022) concluded that an online ACT program for family caregivers of dementia patients reduces depressive symptoms, burden, and stress reactions to behavioral symptoms while increasing positive caregiving aspects and quality of life [10]. Mosher et al. (2022) showed that ACT reduced fatigue in caregivers of advanced gastrointestinal cancer patients [13]. Montaner et al. (2022) explored the implementation and effectiveness of a 6-week ACT intervention for healthcare professionals who work with dementia patients. The aim was to reduce anxiety and burnout, as well as enhance psychological flexibility and life satisfaction. The researchers found that the intervention group showed significant decreases in emotional exhaustion and anxiety levels, along with an increase in life satisfaction and personal success. In addition, the intervention yielded reductions in job exhaustion and improvements in psychological flexibility. These results were maintained at the three and 12-month follow-up periods [23]. Fauth et al. (2022) carried out a research project to investigate the effectiveness of an online pilot program in utilizing ACT for family caregivers of individuals with dementia. The results showed that participants experienced reduced depressive symptoms, burden, and stress reactions to symptoms, along with increased positive aspects of care and quality of life, as measured through pre-test, post-test, and 4-week follow-up assessments. Specifically, participants showed improvements in cognitive dissonance, psychological inflexibility, and living according to personal values. All of these outcomes were statistically significant and sustained during the 4-week follow-up period [24].
It can be said that the evaluation of stressors determines their positive or negative outcomes [23, 24]. Identifying how maladaptive evaluations form, modifying them for compatibility, managing negative evaluations, and creating self-efficacy in managing complex thoughts are key intervention points for caregivers [25]. ACT is a valuable tool, facilitating the processing of complex thoughts (like negative stress evaluation) differently than many other psychosocial approaches. ACT helps caregivers overcome difficult emotions by teaching them to identify what is meaningful and align with their values. Clarifying values in areas such as mental health and interpersonal relationships, through acceptance and diffusion processes in ACT, enhances the social health dimensions of caregivers. Studies have also shown that ACT-based therapy is effective in reducing psychological disturbances (stress, depression and anxiety) and enhancing the physical and socio-psychological dimensions of patients, thus potentially impacting caregiver burden [26].
The research findings indicated that ACT intervention is effective in enhancing psychological flexibility in caregivers of Alzheimer’s patients. This finding is consistent with the results of Herbert & Forman [26], Aliakbari Dehkordi et al. [27], Zolfaghari et al. [28] and Fallah & Ghodsi [29]. According to the findings of Garivani and colleagues (2021) [30], commitment and acceptance-based therapy effectively increase psychological flexibility in mothers of children with tic disorders. Fallah & Ghodsi [29], in a sample study of 30 patients, demonstrated the effectiveness of ACT in increasing psychological flexibility in coronary artery disease patients [29]. Herbert and Forman’s study [26] indicated the effectiveness of ACT in enhancing psychological flexibility [26]. Feros and colleagues [31] showed that commitment and acceptance-based training improved psychological flexibility and acceptance of unpleasant thoughts in cancer patients [29]. Similarly, Wersebe and colleagues [32] showed with a sample of 91 individuals experiencing high work stress that ACT can increase psychological flexibility and reduce distress [32]. Psychological flexibility acts as a guiding force regulating emotional, cognitive, and behavioral domains. This primary indicator of emotional health positively influences emotional regulation, cognitive flexibility, behavioral adaptation, and the ability to change one’s mindset, enabling individuals to modify their behavior and reconcile with others [33].
Bennett-Levy et al. [34] stated that psychological flexibility can alter mindsets or behavioral sets when strategies threaten individual or social performance [34]. Psychological flexibility maintains a balance between essential life domains and the ability to be mindful, accepting, and committed to behaviors that deeply align with values. Therefore, as an educational approach, acceptance and commitment-based interventions focus on creating psychological flexibility through meaningful cognitive roles, valuable language, and structured timing [34]. This intervention and approach do not examine thoughts and feelings from a cognitive-behavioral perspective but delve into strategies for processing personal experiences. During the ACT process, caregivers learn to enjoy life despite its challenges and find meaning while being satisfied with themselves [36]. This approach emphasizes that challenges and engagement with beliefs should be reduced since the struggle with thoughts or emotions exacerbates problems [17].
The limitations of the current study that need to be mentioned are: Non-random sampling, the measurement tool for the study’s dependent variables was a questionnaire, which may introduce response bias. The sample of this study was limited to individuals aged 30 to 45 in Tehran, making it challenging to generalize the results. The role of caregivers in the patient’s life was not addressed, and the severity levels of Alzheimer’s disease among the participants were not considered. Consequently, the caregiving burden experienced by informal caregivers might differ.
To address these research limitations and obtain more accurate results, it is recommended to utilize other methods, such as clinical interviews, to gather more accurate information and reduce measurement error of dependent variables. Conduct similar studies on other age groups and compare their results with this study. Given the limited sample size of this study, it should be replicated with larger sample sizes to ensure the results’ generalizability. Similar studies should be conducted on caregivers of other chronic illnesses, and their results should be compared with this study. The role of caregivers in the patient’s life should be considered in future research, and the severity levels of Alzheimer’s disease among the participants should be evaluated and distinguished.
Conclusion
Given that the effectiveness of ACT on caregiving burden and psychological flexibility in caregivers of aged Alzheimer’s patients has been confirmed in the present study, and since many family caregivers report that available resources do not sufficiently meet their wishes or needs, clinical psychologists and health professionals are recommended to support caregivers in their roles better and enhance their mental well-being through intervention programs focused on compassion so that they can be more effective in accompanying the treatment process of Alzheimer’s patients.
Ethical Considerations
Compliance with ethical guidelines
The present study was approved by Ethics Committee of Islamic Azad University, Roudehen Branch (Code: IR.IAU.R.REC.1402.019).
Funding
The paper was extracted from the master's thesis of Seyed Farzan Madani, approved by Islamic Azad University, Roudehen Branch.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The completion of this study would not have been possible without the dedication and hard work of numerous individuals. Their contributions and support have been invaluable.
References
- Pentz R, Iulita MF, Mikutra-Cencora M, Ducatenzeiler A, Bennett DA, Cuello AC. A new role for matrix metalloproteinase-3 in the NGF metabolic pathway: Proteolysis of mature NGF and sex-specific differences in the continuum of Alzheimer's pathology. Neurobiol Dis. 2021; 148:105150. [DOI:10.1016/j.nbd.2020.105150] [PMID] [PMCID]
- Jahn T, Clark C, Kerksiek A, Lewczuk P, Lütjohann D, Popp J. Cholesterol metabolites and plant sterols in cerebrospinal fluid are associated with Alzheimer's cerebral pathology and clinical disease progression. J Steroid Biochem Mol Biol. 2021; 205:105785. [DOI:10.1016/j.jsbmb.2020.105785] [PMID]
- Albugami M, Qadi N, Almugbel F, Mohammed A, Alttas A, Elamin A, et al. The demographic characteristics and the risk factors of dementia in Saudi elderly. Am J Psychiatry Neurosci. 2018; 6(1):1-8. [DOI:10.11648/j.ajpn.20180601.11]
- Bernstein A, Merrilees J, Dulaney S, Harrison KL, Chiong W, Ong P, et al. Using care navigation to address caregiver burden in dementia: A qualitative case study analysis. Alzheimers Dement. 2020; 6(1):e12010. [DOI:10.1002/trc2.12010] [PMID] [PMCID]
- Badawoud AM, AlQadheeb YK, AlZahrani SS, AlGhamdi RA, Alanazi EA, AlFozan SM, et al. The level of burden among caregivers of patients with alzheimer's disease in Saudi Arabia. Int J Environ Res Public Health. 2023; 20(4):2864. [DOI:10.3390/ijerph20042864] [PMID] [PMCID]
- Tan KP, Ang JK, Koh EBY, Pang NTP, Mat Saher Z. Relationship of psychological flexibility and mindfulness to caregiver burden, and depressive and anxiety symptoms in caregivers of people with dementia. Int J Environ Res Public Health. 2023; 20(5):4232. [DOI:10.3390/ijerph20054232] [PMID] [PMCID]
- Kishita N, Contreras ML, West J, Mioshi E. Exploring the impact of carer stressors and psychological inflexibility on depression and anxiety in family carers of people with dementia. J Contextual Behav Sci. 2020; 17:119-25. [DOI:10.1016/j.jcbs.2020.07.005]
- Jansen JE, Haahr UH, Lyse HG, Pedersen MB, Trauelsen AM, Simonsen E. Psychological flexibility as a buffer against caregiver distress in families with psychosis. Front Psychol. 2017; 8:1625. [DOI:10.3389/fpsyg.2017.01625] [PMID] [PMCID]
- Lappalainen P, Keinonen K, Pakkala I, Lappalainen R, Nikander R. The role of thought suppression and psychological inflexibility in older family caregivers’ psychological symptoms and quality of life. J Contextual Behav Sci. 2021; 20:129-36. [DOI:10.1016/j.jcbs.2021.04.005]
- Zhang CQ, Leeming E, Smith P, Chung PK, Hagger MS, Hayes SC. Acceptance and commitment therapy for health behavior change: A contextually-driven approach. Front Psychol. 2018; 8:2350. [PMID]
- Lappalainen P, Pakkala I, Lappalainen R, Nikander R. Supported web-based acceptance and commitment therapy for older family caregivers (CareACT) compared to usual care. Clin Gerontol. 2022; 45(4):939-55. [DOI:10.1080/07317115.2021.1912239] [PMID]
- Montaner X, Tárrega S, Pulgarin M, Moix J. Effectiveness of acceptance and commitment therapy (ACT) in professional dementia caregivers burnout. Clin Gerontol. 2022; 45(4):915-26. [DOI:10.1080/07317115.2021.1920530] [PMID]
- Mosher CE, Secinti E, Wu W, Kashy DA, Kroenke K, Bricker JB, et al. Acceptance and commitment therapy for patient fatigue interference and caregiver burden in advanced gastrointestinal cancer: Results of a pilot randomized trial. Palliat Med. 2022; 36(7):1104-17. [DOI:10.1177/02692163221099610] [PMID] [PMCID]
- Shabani M, Jarareh J. [The effectiveness of mindfulness-based stress reduction on caregiver burden and mental fatigue of autistic children’s mothers (Persian)]. Soc Work Mag. 2020; 9(1):5-12. [Link]
- Kazemi A, Ahadi H, Nejat H. [Effectiveness of compassion focused therapy on loneliness, self-care behaviors and blood sugar in diabetes patients (Persian)]. Iran J Rehabil Res Nurs. 2020; 6(3):42-9. [Link]
- Hoseinpoor M, Nourozi K, Rahgoi A, Ghasemi S, Noroozi M, Babaie M. [The relationship between care burden, care preparedness and the quality of life in the home caregivers of the aged with the alzheimer’s disease in Iran Alzheimer’s association (Persian)]. J Gerontol. 2021; 6(2):10-8. [Link]
- Hayes SC, Strosahl KD, Wilson KG. Acceptance and commitment therapy: The process and practice of mindful change. New York: Guilford Press; 2012. [Link]
- Hayes SC, Strosahl K, Wilson KG, Bissett RT, Pistorello J, Toarmino D, et al. Measuring experiential avoidance: A preliminary test of a working model. Psychol Rec. 2004; 54:553-78. [DOI:10.1007/BF03395492]
- Bond FW, Hayes SC, Baer RA, Carpenter KM, Guenole N, Orcutt HK, et al. Preliminary psychometric properties of the acceptance and action questionnaire-II: A revised measure of psychological inflexibility and experiential avoidance. Behav Ther. 2011; 42(4):676-88. [DOI:10.1016/j.beth.2011.03.007] [PMID]
- Abasi E, Fti L, Molodi R, Zarabi H. [Psychometric properties of Persian version of acceptance and action questionnaire-II (Persian)]. Psychol Methods Models. 2012; 3(10):65-80. [Link]
- Novak M, Guest C. Application of a multidimensional caregiver burden inventory. Gerontologist. 1989; 29(6):798-803. [DOI:10.1093/geront/29.6.798] [PMID]
- Shafiezadeh A, Heravi-Karimooi M, Mirzaee A, Rejeh N, Sharif Nia H, Montazeri A. Psychometric characteristics of the iranian caregiver burden inventory (CBI) in caregivers of elderly patients with Alzheimer. Health Qual Life Outcomes. 2020; 18(1):255. [DOI:10.1186/s12955-020-01509-7] [PMID] [PMCID]
- Justice NJ. The relationship between stress and Alzheimer's disease. Neurobiol Stress. 2018; 8:127-33. [PMID]
- Fauth EB, Novak JR, Levin ME. Outcomes from a pilot online Acceptance and Commitment Therapy program for dementia family caregivers. Aging Ment Health. 2022; 26(8):1620-9. [DOI:10.1080/13607863.2021.1942432] [PMID]
- Cheng ST, Fung HH, Chan WC, Lam LC. Short-term effects of a gain-focused reappraisal intervention for dementia caregivers: A double-blind cluster-randomized controlled trial. Am J Geriatr Psychiatry. 2016; 24(9):740-50. [DOI:10.1016/j.jagp.2016.04.012] [PMID]
- Forman EM, Herbert JD. Acceptance and mindfulness in cognitive behavior therapy: Understanding and applying the new therapies. Hoboken: Wiley; 2011. [Link]
- Aliakbari Dehkordi M, Ghafoori S, Jaffary F, Mohtashami T. [The effect of acceptance and commitment therapy (ACT) on physical symptoms, psychosocial flexibility and social health of patients with psoriasis (Persian)]. Knowl Res Appl Psychol. 2021; 21(4):118-32. [DOI:10.30486/jsrp.2019.580247.1584]
- Zolfaghari M, Nikooei F, Shahbazi Seyed Ahmadiyani A, Kohanroozamiri S. [The effectiveness of acceptance and commitment-based therapy on psychological flexibility and quality of life of divorced women (Persian)]. Middle East J Disabil Stud. 2021; 11:208. [Link]
- Fallah K, Ghodsi M. [The effectiveness of acceptance and commitment therapy on the psychological flexibility of patients with coronary heart disease (Persian)]. J Psychol New Ideas. 2022; 13(17):1-14. [Link]
- Garivani G, Booyeh MA, Taheri E. The effectiveness of treatment based on acceptance and commitment to psychological flexibility and perfectionism in mothers of children with tic disorders. J Fundam Ment Health. 2020; 22(6): 349-55. [DOI: 10.22038/JFMH.2020.17597]
- Feros DL, Lane L, Ciarrochi J, Blackledge JT. Acceptance and commitment therapy (ACT) for improving the lives of cancer patients: A preliminary study. Psychooncology. 2013 Feb;22(2):459-64. [DOI:10.1002/pon.2083] [PMID]
- Wersebe H, Lieb R, Meyer AH, Hofer P, Gloster AT. The link between stress, well-being, and psychological flexibility during an acceptance and commitment therapy self-help intervention. Int J Clin Health Psychol. 2018 18(1):60-8. [DOI:10.1016/j.ijchp.2017.09.002] [PMID] [PMCID]
- Kashdan TB, Rottenberg J. Psychological flexibility as a fundamental aspect of health. Clin Psychol Rev. 2010; 30(7):865-78. [DOI:10.1016/j.cpr.2010.03.001] [PMID] [PMCID]
- Bennett-Levy J, Lee NK. Self-practice and self-reflection in cognitive behaviour therapy training: What factors influence trainees' engagement and experience of benefit? Behav Cogn Psychother. 2014; 42(1):48-64. [DOI:10.1017/S1352465812000781] [PMID]
- Hayes-Skelton SA, Roemer L, Orsillo SM. A randomized clinical trial comparing an acceptance-based behavior therapy to applied relaxation for generalized anxiety disorder. J Consult Clin Psychol. 2013; 81(5):761-73. [DOI:10.1037/a0032871] [PMID] [PMCID]
- Köhle N, Drossaert CHC, Jaran J, Schreurs KMG, Verdonck-de Leeuw IM, Bohlmeijer ET. User-experiences with a web-based self-help intervention for partners of cancer patients based on acceptance and commitment therapy and self-compassion: A qualitative study. BMC Public Health. 2017; 17(1):225. [DOI:10.1186/s12889-017-4121-2] [PMID] [PMCID]
Article Type: Original Contributions |
Subject:
Health Management
Received: 2023/12/15 | Accepted: 2024/02/20 | Published: 2024/04/1
Received: 2023/12/15 | Accepted: 2024/02/20 | Published: 2024/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
