

Volume 9, Issue 2 (4-2024)
CJHR 2024, 9(2): 95-104 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
joukar F, Asgharnezhad M, Maroufizadeh S, Yeganeh S, Aghajani Nargessi D, Zohrehvand B, et al . Treatment Seeking Behavior for COVID-19 Symptoms Among Northern Iranian Population: A Cross-sectional Study. CJHR 2024; 9 (2) :95-104
URL: http://cjhr.gums.ac.ir/article-1-357-en.html
URL: http://cjhr.gums.ac.ir/article-1-357-en.html
Farahnaz Joukar1 

 , Mehrnaz Asgharnezhad1 , Saman Maroufizadeh2 , Sara Yeganeh1 , Dorrin Aghajani Nargessi3 , Behzad Zohrehvand4 , Mahsa Safizadeh1 , Alireza Gholizadeh5 , Zahra Rajabian Moghaddam6 , Fariborz Mansour-Ghanaei1 , Mohammadreza Naghipour *7
, Mehrnaz Asgharnezhad1 , Saman Maroufizadeh2 , Sara Yeganeh1 , Dorrin Aghajani Nargessi3 , Behzad Zohrehvand4 , Mahsa Safizadeh1 , Alireza Gholizadeh5 , Zahra Rajabian Moghaddam6 , Fariborz Mansour-Ghanaei1 , Mohammadreza Naghipour *7
, Mehrnaz Asgharnezhad1 , Saman Maroufizadeh2 , Sara Yeganeh1 , Dorrin Aghajani Nargessi3 , Behzad Zohrehvand4 , Mahsa Safizadeh1 , Alireza Gholizadeh5 , Zahra Rajabian Moghaddam6 , Fariborz Mansour-Ghanaei1 , Mohammadreza Naghipour *7
1- Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran
2- Department of Biostatistics, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran
3- Department of Emergency Medicine, School of Medicine Razi Hospital, Guilan University of Medical Sciences, Rasht, Iran.
4- Department of Emergency Medicine, School of Medicine Razi Hospital, Guilan University of Medical Sciences, Rasht, Iran
5- School of Medicine Heshmat Hospital, Guilan University of Medical Sciences, Rasht, Iran
6- School of Medicine Razi Hospital, Guilan University of Medical Sciences, Rasht, Iran
7- Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran ,naghi@gums.ac.ir
2- Department of Biostatistics, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran
3- Department of Emergency Medicine, School of Medicine Razi Hospital, Guilan University of Medical Sciences, Rasht, Iran.
4- Department of Emergency Medicine, School of Medicine Razi Hospital, Guilan University of Medical Sciences, Rasht, Iran
5- School of Medicine Heshmat Hospital, Guilan University of Medical Sciences, Rasht, Iran
6- School of Medicine Razi Hospital, Guilan University of Medical Sciences, Rasht, Iran
7- Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran ,
Full-Text [PDF 609 kb]
(337 Downloads)
| Abstract (HTML) (1245 Views)
Full-Text: (342 Views)
Introduction
In December 2019, a new virus called corona virus disease 2019 (COVID-19), as an acute respiratory syndrome disease, emerged in Wuhan, Hubei Province, China [1]. The corona virus 2019 spread rapidly to other countries, despite China’s extensive efforts to control it and in 2 months infected 25 countries worldwide [2] and on March 11, 2020, World Health Organization (WHO) declared the global pandemic of corona virus as a public health emergency of international concern [3]. As of July 16, 2020, there are roughly 13.700.000 COVID-19 cases and 586.000 deaths worldwide [3].
Following its global outbreak, on February 19, Iranian officials announced the outbreak of corona virus 2019 in the country and Qom and Guilan (northern provinces of Iran) was the first provinces infected [4]. The virus spread rapidly in Iran and by March 5, 2020, all 31 provinces were infected through person-to-person transmission. The total number of confirmed cases by July 16 was 264561, with 13410 deaths and 227561 recoveries reported in Iran [3].
Average of incubation period of this virus varies between 5-7 days, so the suspected contacts are recommended to quarantine for 14 days [5]. The most common clinical manifestation at the disease onset includes sore throat, fever, myalgia and cough [6]. Severe illness occurs in about 15% of patients, leading to hospitalization [7].
According to the Centers for Disease Control and Prevention (CDC) recommendation, home management may be appropriate for patients who have a mild infection or who can be treated outpatient and isolated in appropriate conditions [8]. The management of such patients should focus on preventing the virus transmission and monitoring the clinical condition to hospitalize immediately if needed [8].
Despite extreme precautions to seek medical attention in case of cough, fever and difficulty breathing, in many cases people with symptoms avoid contacting health care provider. A recent Gallup study shows that in the United States, 14% of adults do not seek treatment for corona virus for themselves or a household member [9]. There have also been frequent reports of patient avoiding professional medical care in low- and middle-income countries [10]. About two-thirds of corona victims in Russia first decided to self-care and then found themselves in critical condition in hospitals [11].
Early detection of individual suspected to COVID-19 and contact tracing is necessary for infection control [12]. Identifying and limiting obstacles to appropriate treatment seeking for symptomatic patient improves disease management and control [13].
COVID-19 will not be the last pandemic in our deeply interconnected world, and sadly it won’t be the worst. With all preventive measures in the face of COVID-19, we will certainly face pandemics in the future. However, the world must obviously prepare for future pandemics in light of the lessons learnt from the Coronavirus disease 2019 (COVID-19) pandemic [14]. Availability of health care providers, perceived susceptibility and severity of disease, social and demographic characteristics of individuals may be affected treatment-seeking behaviors [15]. Since the patients’ treatment-seeking behavior can change in different cultures and time periods [16], and considering the importance of the early detection of individual suspected to COVID-19, Therefore, this study was conducted to investigate the treatment seeking behavior of suspected to COVID-19 infections among northern Iranian population and its related factors.
Materials and Methods
Study design
This hospital-based cross-sectional study was conducted for a period of 2 months between March and May 2020 in Guilan (northern provinces of Iran) at the onset of the corona epidemic in Iran.
Study participants were selected by a convenient sampling method from the only referral hospital in the province. The sample size was estimated to be 606 participants, based on the main outcome, namely, treatment seeking behavior and the number of related factors, with confidence level of 95% and test power of 80%. The inclusion criteria were patients who were hospitalized with a confirmed COVID-19 diagnosis. Confirmed case of COVID-19 was defined as positive real-time fluorescent quantitative polymerase chain reaction (RT-PCR) and/or chest CT manifestations including sub pleural ground glass shadows, with or without pulmonary interstitial thickening [17]. If the participant’s skipping a question led to missing data, they were excluded from study.
Data collection
In this study, relevant information was collected using a questionnaire containing five areas.
Section 1 collected data on sociodemographic characteristics of patient, including age, education, gender, occupation, residency, marital status and health insurance. Section 2 collected data on symptom of COVID-19 infection including fever, cough, sore throat, breathing difficulties, coryza, weakness, muscular pain, confusion, headache, chest pain, diarrhea, nausea and vomiting, anorexia, anosmia and chills. Section 3 collected data on past medical history including diabetes mellitus, hypertension, respiratory diseases and obesity (body mass index (BMI) ≥30). Section 4 collected data on self-reported first action with onset of COVID-19 symptoms as treatment seeking behavior. Treatment-seeking was classified as following: a) Seeking care from professionals including all private or public hospitals, health centers or private doctors. b) Self-medication. c) Traditional care or home remedy.
Data analyses
Data analyses were performed by SPSS software, version 17.0. Frequency distribution of the first treatment-seeking behaviors according to characteristics of patient, symptoms of patients and past medical history were compared with chi-square test. Univariate and multivariate logistic regression analysis were performed to identify significant predictors of professional treatment-seeking. Factors with a P<0.05 on a univariate model were entered into a multivariate logistic regression model. Unadjusted and adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated.
Result
Characteristics of patient
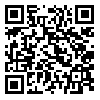
Of the total 602 subjects who participated in the study (two patients excluded due to incomplete data), 54.7% were men. The age of patient ranged from 19 to 99 years old, with an average age of 54.6±13.9 years. Half of patients (50%) were between the ages of 46–64. The majority of the patients were urban residents (80.0%), were married (82.1%), had diploma or less level of education (72.9%), covered by health insurance (85.9%), and 43.3% of them were employed (Table 1).
One-third of patients had positive family history of corona infection and past history of diabetes, hypertension, respiratory disease and obesity was reported in 19.3%, 9.6%, 6.1% and 31.6% of patient respectively (Table 1).
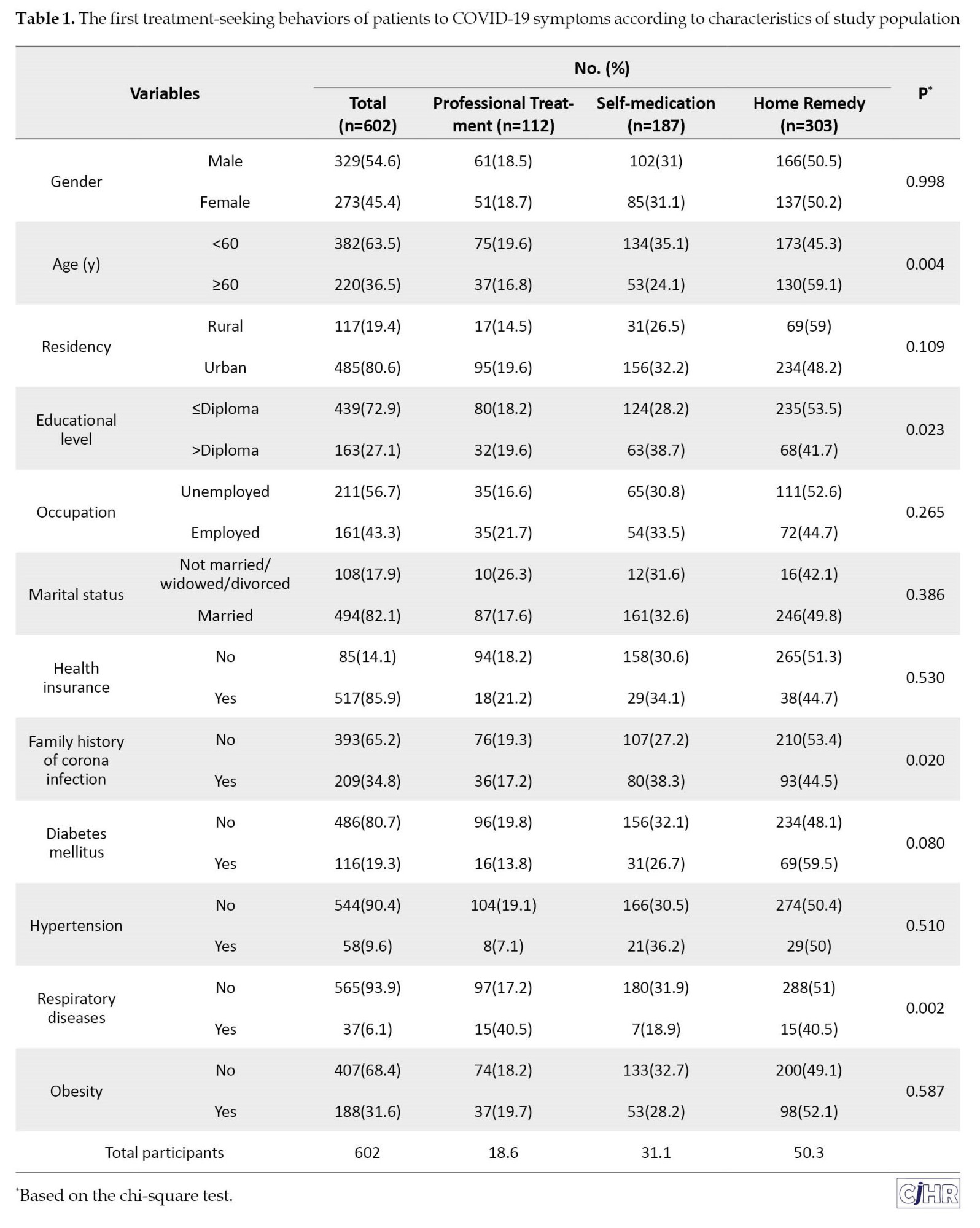
The most prevalent symptoms of COVID-19 in the study population were anosmia (98.3%) and fever (70.1%) (Table 2).
Treatment-seeking behaviors
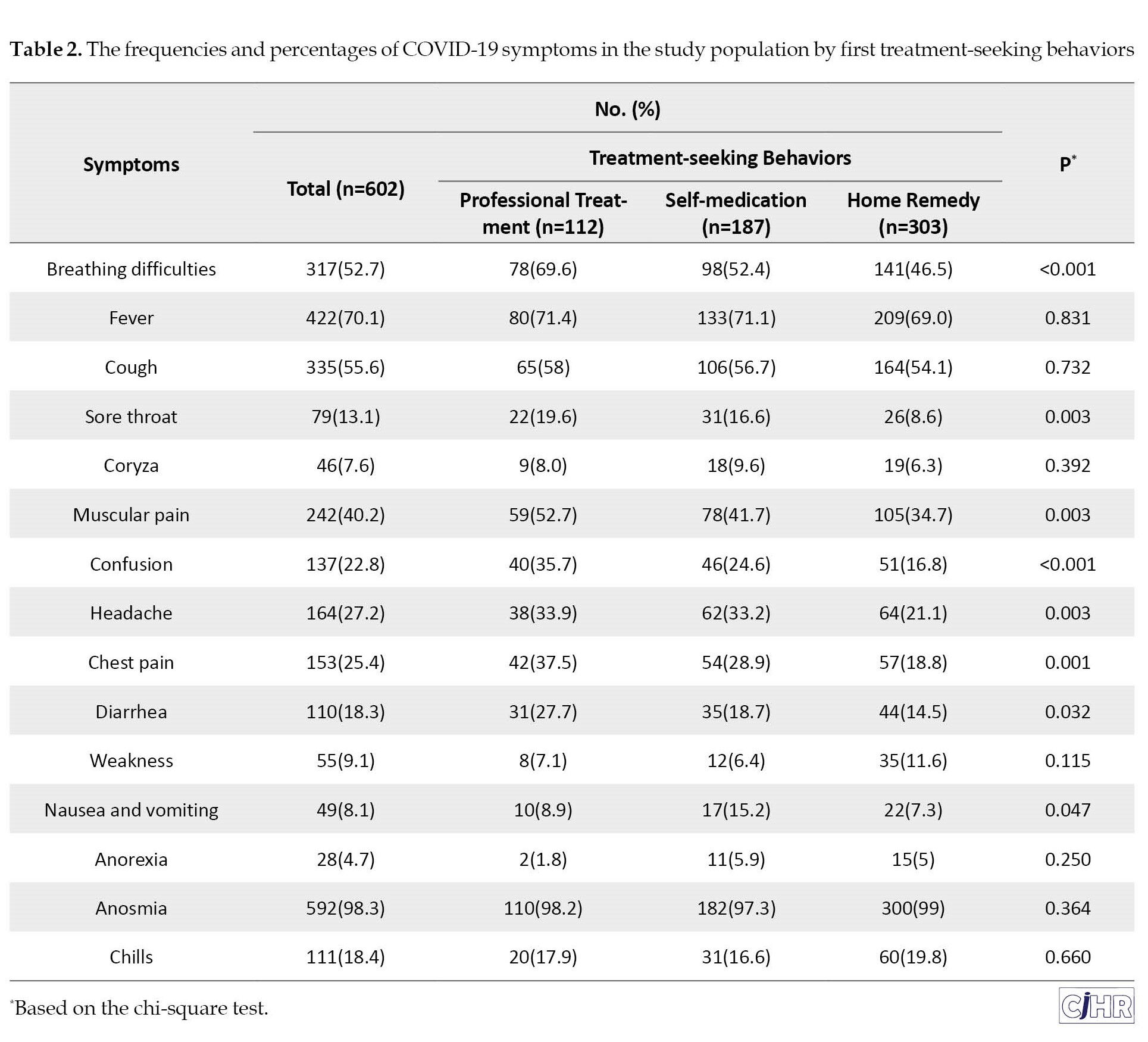
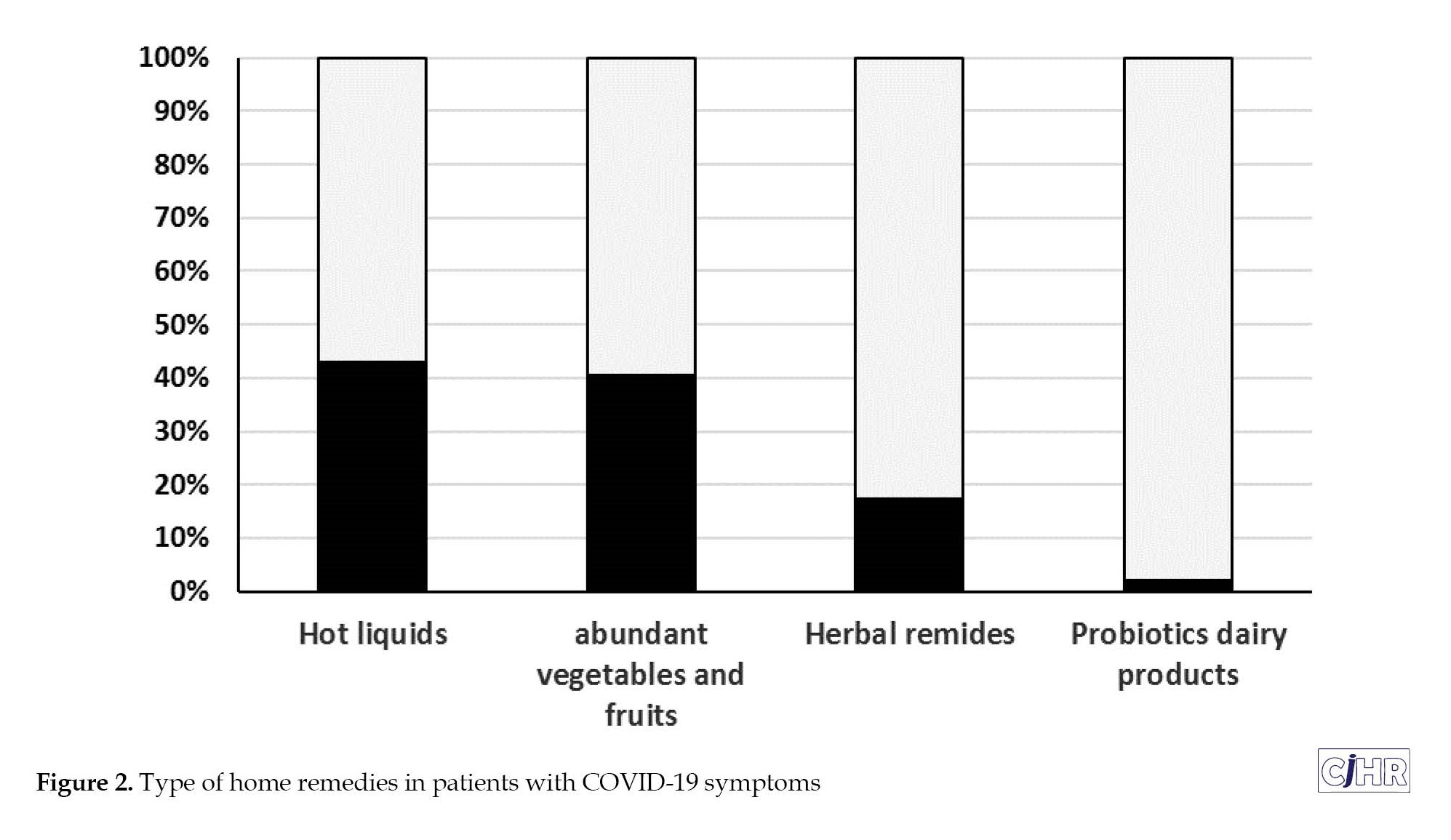
Regarding the first reaction to COVID-19 symptoms, only 18.6% of patients reported professional treatment-seeking and most of the patients reported home remedies (50.3%) as first treatment-seeking behaviors (Table 1). Type of self-medication and home remedies presented in Figures 1 and 2 respectively.
The first treatment-seeking behaviors of patients to COVID-19 symptoms according to characteristics of study population are shown in Table 1. Home remedies were significantly (P=0.021) more common in less educated patient (53.5%) than more educated (41.7%). Also, older patient (≥60 years) was significantly (P=0.004) more likely to seek home remedies behaviors (59.1%) than younger ones (45.3%). Self-medication were significantly (P=0.029) more common in patients with family history of corona infection (38.3%) than those with no history (27.2%). Professional treatment-seeking increased significantly (P=0.002) in patient with a history of respiratory disease (40.5%) than those with no history (17.2%).
As shown in Table 2, patient with symptom of breathing difficulties, headache, muscular pain, confusion, chest pain, diarrhea and sore throat were significantly more likely to seek professional treatment (All P<0.05).
Table 3 reveals the results univariate and multivariate logistic regression to explore the predictors of professional treatment -seeking.
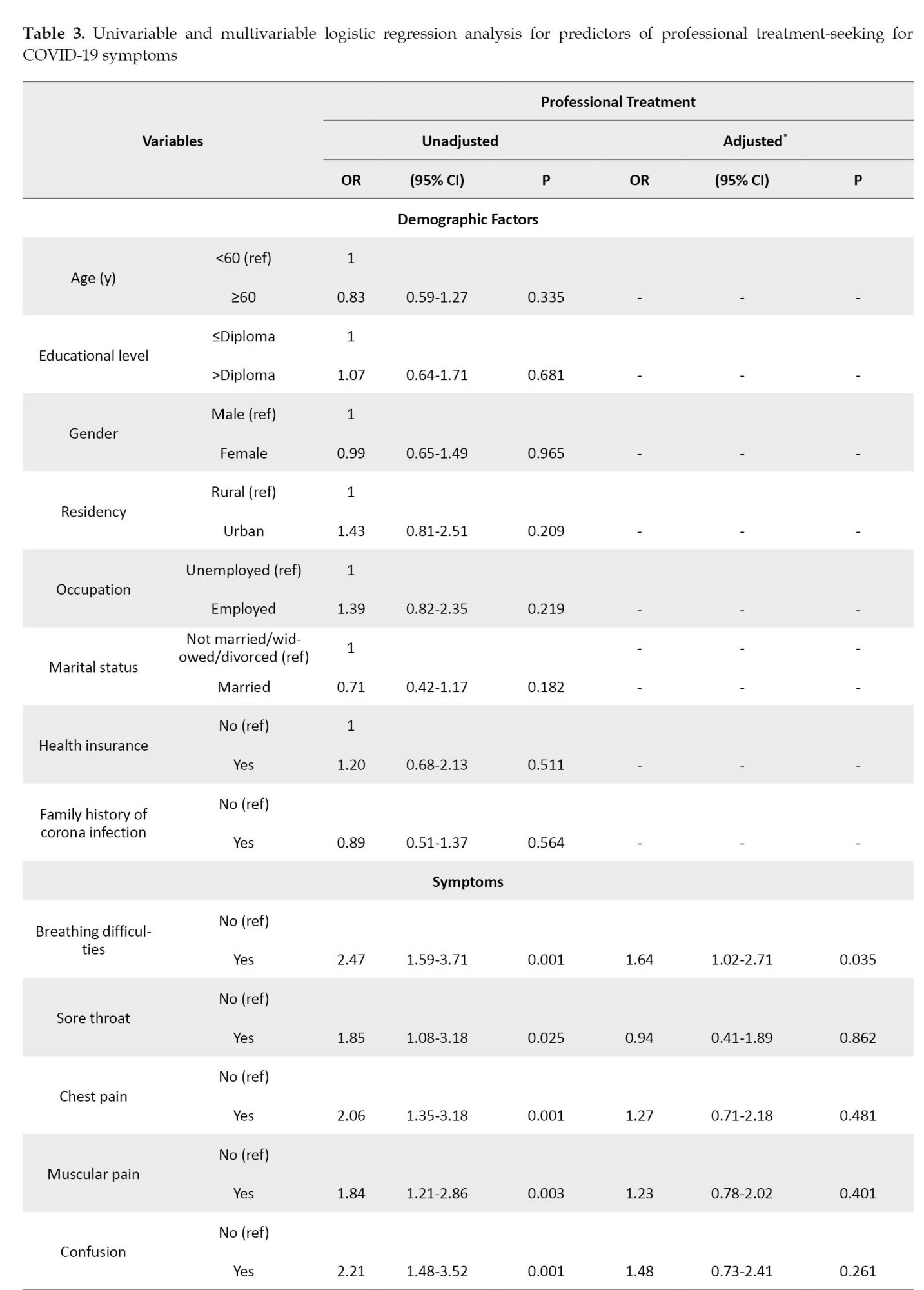

Only breathing difficulties symptom and past history of respiratory disease were identified as an independent factor associated with professional treatment–seeking. Patient with breathing difficulties symptom had greater odds (adjusted OR=1.6, P=0.03) of professional treatment seeking. Also, patient with history of respiratory disease had greater odds (adjusted OR=3.3, P=0.001) of professional treatment seeking. There was no independent association of demographic factor and past history of diabetes, hypertension and obesity with professional treatment-seeking (Table 3).
Discussion
The study sought to determine the treatment seeking behaviors for COVID-19 symptoms and its related factors in northern Iranian population. The findings revealed that roughly half of symptomatic patient reported home remedies as first treatment-seeking behaviors and only breathing difficulties symptom or past history of respiratory disease were identified as an independent factor associated with professional treatment–seeking. Although, the use of home remedies is common in patients experience flu-like symptoms such COVID-19, worldwide [18-20], but it can increase the risk of developing more severe symptoms specially in patient with comorbidities such as diabetes, hypertension, cancer and respiratory disease [21]. Elderly, diabetics, hypertensive and obese patients were at increased risk for severe illness and death from COVID-19 infections [22, 23]. National guidelines for diagnosis and treatment of COVID-19 recommended that early detection by RT-PCR and early therapy with chloroquine may be beneficial in symptomatic high-risk patient [24].
The results of current study revealed that the independent determinants of professional treatment-seeking were breathing difficulties symptom and past history of respiratory disease. It might be due to participant’s awareness of importance and risk of respiratory involvement and take necessary precautionary measures. The mass media played a role in increase this knowledge and attitude [10, 25]. However, we found no independent association of demographic factor and past history of diabetes, hypertension and obesity with professional treatment-seeking, while elderly and these underling diseases were at risk of severe illness and death from COVID-19 infections [21]. Thus, sensitizing patients with underling disease and older age to seeking professional treatment is crucial.
Although, patient with symptom of muscular pain, confusion, chest pain, diarrhea and sore throat were meaningfully more likely to seek professional treatment, but this association disappeared after fully adjustment for other medical and demographic factors. Since, the symptom screening has become a universal tool to limit further spread of COVID-19 [26]. Our results indicate that it is critical to raise population’s awareness of initial and mild symptoms of COVID-19.
However, in this situation, without specific anti-viral drug regime for COVID-19 [27], research on efficacy and limitation of home remedies and traditional therapies for COVID-19 might be an interesting issue that needs to be explored and communication of updated evidence to the public would help improve appropriate seeking treatment. This study has a limitation, due to the hospital-based design and selection of more severe illness that limited generalizability of findings.
Conclusion
The results of current study indicated that roughly half of symptomatic COVID-19 patient reported home remedies as first treatment-seeking behaviors and only breathing difficulties symptom and past history of respiratory disease were identified as an independent predictor of professional treatment–seeking. However, we found no more professional treatment -seeking behaviors among elderly, diabetic, hypertensive and obese patients, while there were at risk of severe illness and death from COVID-19 infections. Thus, behavior change interventions in population with underling disease (including diabetes, hypertension and obesity) and older age is crucial to improve professional treatment-seeking behaviors. We hope that the results of this study can be a lesson for the future.
Limitation
This study investigated people’s seeking behavior in the early months of the COVID-19 pandemic, when strict home quarantine measures were in place in society and there were numerous recommendations for people to avoid crowded areas, including hospitals. The initial fear caused by the pandemic was the primary factor influencing people’s treatment-seeking behaviors.
Additionally, the severity and simultaneity of symptoms of COVID-19 is another significant confounding factor in the selection of treatment seeking behavior that has not been addressed.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Guilan University of Medical Sciences (Code: IR.GUMS.REC.1399.005). Written informed consent was obtained from every participating respondent.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Fariborz Mansour-Ghanaei, Mohammadreza Naghipour, Farahnaz Joukar, Mehrnaz Asgharnezhad and Saman Maroufizadeh; Supervision: Fariborz Mansour-Ghanaei, Farahnaz Joukar, Mohammadreza Naghipour; Methodology: Saman Maroufizadeh; Investigation: Mehrnaz Asgharnezhad; Data collection: Dorrin Aghajani Nargessi, Behzad Zohrehvandi, Mahsa Safizadeh, Alireza Gholizadeh and Zahra Rajabian Moghaddam; Data analysis: Saman Maroufizadeh; Writing the original draft: Fariborz Mansour-Ghanaei, Farahnaz Joukar, Mohammadreza Naghipour, Mehrnaz Asgharnezhad; Review and editing: Farahnaz Joukar, Mehrnaz Asgharnezhad and Saman Maroufizadeh.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors appreciate the assistance Heydar Ali Balou.
References
In December 2019, a new virus called corona virus disease 2019 (COVID-19), as an acute respiratory syndrome disease, emerged in Wuhan, Hubei Province, China [1]. The corona virus 2019 spread rapidly to other countries, despite China’s extensive efforts to control it and in 2 months infected 25 countries worldwide [2] and on March 11, 2020, World Health Organization (WHO) declared the global pandemic of corona virus as a public health emergency of international concern [3]. As of July 16, 2020, there are roughly 13.700.000 COVID-19 cases and 586.000 deaths worldwide [3].
Following its global outbreak, on February 19, Iranian officials announced the outbreak of corona virus 2019 in the country and Qom and Guilan (northern provinces of Iran) was the first provinces infected [4]. The virus spread rapidly in Iran and by March 5, 2020, all 31 provinces were infected through person-to-person transmission. The total number of confirmed cases by July 16 was 264561, with 13410 deaths and 227561 recoveries reported in Iran [3].
Average of incubation period of this virus varies between 5-7 days, so the suspected contacts are recommended to quarantine for 14 days [5]. The most common clinical manifestation at the disease onset includes sore throat, fever, myalgia and cough [6]. Severe illness occurs in about 15% of patients, leading to hospitalization [7].
According to the Centers for Disease Control and Prevention (CDC) recommendation, home management may be appropriate for patients who have a mild infection or who can be treated outpatient and isolated in appropriate conditions [8]. The management of such patients should focus on preventing the virus transmission and monitoring the clinical condition to hospitalize immediately if needed [8].
Despite extreme precautions to seek medical attention in case of cough, fever and difficulty breathing, in many cases people with symptoms avoid contacting health care provider. A recent Gallup study shows that in the United States, 14% of adults do not seek treatment for corona virus for themselves or a household member [9]. There have also been frequent reports of patient avoiding professional medical care in low- and middle-income countries [10]. About two-thirds of corona victims in Russia first decided to self-care and then found themselves in critical condition in hospitals [11].
Early detection of individual suspected to COVID-19 and contact tracing is necessary for infection control [12]. Identifying and limiting obstacles to appropriate treatment seeking for symptomatic patient improves disease management and control [13].
COVID-19 will not be the last pandemic in our deeply interconnected world, and sadly it won’t be the worst. With all preventive measures in the face of COVID-19, we will certainly face pandemics in the future. However, the world must obviously prepare for future pandemics in light of the lessons learnt from the Coronavirus disease 2019 (COVID-19) pandemic [14]. Availability of health care providers, perceived susceptibility and severity of disease, social and demographic characteristics of individuals may be affected treatment-seeking behaviors [15]. Since the patients’ treatment-seeking behavior can change in different cultures and time periods [16], and considering the importance of the early detection of individual suspected to COVID-19, Therefore, this study was conducted to investigate the treatment seeking behavior of suspected to COVID-19 infections among northern Iranian population and its related factors.
Materials and Methods
Study design
This hospital-based cross-sectional study was conducted for a period of 2 months between March and May 2020 in Guilan (northern provinces of Iran) at the onset of the corona epidemic in Iran.
Study participants were selected by a convenient sampling method from the only referral hospital in the province. The sample size was estimated to be 606 participants, based on the main outcome, namely, treatment seeking behavior and the number of related factors, with confidence level of 95% and test power of 80%. The inclusion criteria were patients who were hospitalized with a confirmed COVID-19 diagnosis. Confirmed case of COVID-19 was defined as positive real-time fluorescent quantitative polymerase chain reaction (RT-PCR) and/or chest CT manifestations including sub pleural ground glass shadows, with or without pulmonary interstitial thickening [17]. If the participant’s skipping a question led to missing data, they were excluded from study.
Data collection
In this study, relevant information was collected using a questionnaire containing five areas.
Section 1 collected data on sociodemographic characteristics of patient, including age, education, gender, occupation, residency, marital status and health insurance. Section 2 collected data on symptom of COVID-19 infection including fever, cough, sore throat, breathing difficulties, coryza, weakness, muscular pain, confusion, headache, chest pain, diarrhea, nausea and vomiting, anorexia, anosmia and chills. Section 3 collected data on past medical history including diabetes mellitus, hypertension, respiratory diseases and obesity (body mass index (BMI) ≥30). Section 4 collected data on self-reported first action with onset of COVID-19 symptoms as treatment seeking behavior. Treatment-seeking was classified as following: a) Seeking care from professionals including all private or public hospitals, health centers or private doctors. b) Self-medication. c) Traditional care or home remedy.
Data analyses
Data analyses were performed by SPSS software, version 17.0. Frequency distribution of the first treatment-seeking behaviors according to characteristics of patient, symptoms of patients and past medical history were compared with chi-square test. Univariate and multivariate logistic regression analysis were performed to identify significant predictors of professional treatment-seeking. Factors with a P<0.05 on a univariate model were entered into a multivariate logistic regression model. Unadjusted and adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated.
Result
Characteristics of patient
Of the total 602 subjects who participated in the study (two patients excluded due to incomplete data), 54.7% were men. The age of patient ranged from 19 to 99 years old, with an average age of 54.6±13.9 years. Half of patients (50%) were between the ages of 46–64. The majority of the patients were urban residents (80.0%), were married (82.1%), had diploma or less level of education (72.9%), covered by health insurance (85.9%), and 43.3% of them were employed (Table 1).
One-third of patients had positive family history of corona infection and past history of diabetes, hypertension, respiratory disease and obesity was reported in 19.3%, 9.6%, 6.1% and 31.6% of patient respectively (Table 1).
The most prevalent symptoms of COVID-19 in the study population were anosmia (98.3%) and fever (70.1%) (Table 2).
Treatment-seeking behaviors
Regarding the first reaction to COVID-19 symptoms, only 18.6% of patients reported professional treatment-seeking and most of the patients reported home remedies (50.3%) as first treatment-seeking behaviors (Table 1). Type of self-medication and home remedies presented in Figures 1 and 2 respectively.
The first treatment-seeking behaviors of patients to COVID-19 symptoms according to characteristics of study population are shown in Table 1. Home remedies were significantly (P=0.021) more common in less educated patient (53.5%) than more educated (41.7%). Also, older patient (≥60 years) was significantly (P=0.004) more likely to seek home remedies behaviors (59.1%) than younger ones (45.3%). Self-medication were significantly (P=0.029) more common in patients with family history of corona infection (38.3%) than those with no history (27.2%). Professional treatment-seeking increased significantly (P=0.002) in patient with a history of respiratory disease (40.5%) than those with no history (17.2%).
As shown in Table 2, patient with symptom of breathing difficulties, headache, muscular pain, confusion, chest pain, diarrhea and sore throat were significantly more likely to seek professional treatment (All P<0.05).
Table 3 reveals the results univariate and multivariate logistic regression to explore the predictors of professional treatment -seeking.
Only breathing difficulties symptom and past history of respiratory disease were identified as an independent factor associated with professional treatment–seeking. Patient with breathing difficulties symptom had greater odds (adjusted OR=1.6, P=0.03) of professional treatment seeking. Also, patient with history of respiratory disease had greater odds (adjusted OR=3.3, P=0.001) of professional treatment seeking. There was no independent association of demographic factor and past history of diabetes, hypertension and obesity with professional treatment-seeking (Table 3).
Discussion
The study sought to determine the treatment seeking behaviors for COVID-19 symptoms and its related factors in northern Iranian population. The findings revealed that roughly half of symptomatic patient reported home remedies as first treatment-seeking behaviors and only breathing difficulties symptom or past history of respiratory disease were identified as an independent factor associated with professional treatment–seeking. Although, the use of home remedies is common in patients experience flu-like symptoms such COVID-19, worldwide [18-20], but it can increase the risk of developing more severe symptoms specially in patient with comorbidities such as diabetes, hypertension, cancer and respiratory disease [21]. Elderly, diabetics, hypertensive and obese patients were at increased risk for severe illness and death from COVID-19 infections [22, 23]. National guidelines for diagnosis and treatment of COVID-19 recommended that early detection by RT-PCR and early therapy with chloroquine may be beneficial in symptomatic high-risk patient [24].
The results of current study revealed that the independent determinants of professional treatment-seeking were breathing difficulties symptom and past history of respiratory disease. It might be due to participant’s awareness of importance and risk of respiratory involvement and take necessary precautionary measures. The mass media played a role in increase this knowledge and attitude [10, 25]. However, we found no independent association of demographic factor and past history of diabetes, hypertension and obesity with professional treatment-seeking, while elderly and these underling diseases were at risk of severe illness and death from COVID-19 infections [21]. Thus, sensitizing patients with underling disease and older age to seeking professional treatment is crucial.
Although, patient with symptom of muscular pain, confusion, chest pain, diarrhea and sore throat were meaningfully more likely to seek professional treatment, but this association disappeared after fully adjustment for other medical and demographic factors. Since, the symptom screening has become a universal tool to limit further spread of COVID-19 [26]. Our results indicate that it is critical to raise population’s awareness of initial and mild symptoms of COVID-19.
However, in this situation, without specific anti-viral drug regime for COVID-19 [27], research on efficacy and limitation of home remedies and traditional therapies for COVID-19 might be an interesting issue that needs to be explored and communication of updated evidence to the public would help improve appropriate seeking treatment. This study has a limitation, due to the hospital-based design and selection of more severe illness that limited generalizability of findings.
Conclusion
The results of current study indicated that roughly half of symptomatic COVID-19 patient reported home remedies as first treatment-seeking behaviors and only breathing difficulties symptom and past history of respiratory disease were identified as an independent predictor of professional treatment–seeking. However, we found no more professional treatment -seeking behaviors among elderly, diabetic, hypertensive and obese patients, while there were at risk of severe illness and death from COVID-19 infections. Thus, behavior change interventions in population with underling disease (including diabetes, hypertension and obesity) and older age is crucial to improve professional treatment-seeking behaviors. We hope that the results of this study can be a lesson for the future.
Limitation
This study investigated people’s seeking behavior in the early months of the COVID-19 pandemic, when strict home quarantine measures were in place in society and there were numerous recommendations for people to avoid crowded areas, including hospitals. The initial fear caused by the pandemic was the primary factor influencing people’s treatment-seeking behaviors.
Additionally, the severity and simultaneity of symptoms of COVID-19 is another significant confounding factor in the selection of treatment seeking behavior that has not been addressed.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Guilan University of Medical Sciences (Code: IR.GUMS.REC.1399.005). Written informed consent was obtained from every participating respondent.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Fariborz Mansour-Ghanaei, Mohammadreza Naghipour, Farahnaz Joukar, Mehrnaz Asgharnezhad and Saman Maroufizadeh; Supervision: Fariborz Mansour-Ghanaei, Farahnaz Joukar, Mohammadreza Naghipour; Methodology: Saman Maroufizadeh; Investigation: Mehrnaz Asgharnezhad; Data collection: Dorrin Aghajani Nargessi, Behzad Zohrehvandi, Mahsa Safizadeh, Alireza Gholizadeh and Zahra Rajabian Moghaddam; Data analysis: Saman Maroufizadeh; Writing the original draft: Fariborz Mansour-Ghanaei, Farahnaz Joukar, Mohammadreza Naghipour, Mehrnaz Asgharnezhad; Review and editing: Farahnaz Joukar, Mehrnaz Asgharnezhad and Saman Maroufizadeh.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors appreciate the assistance Heydar Ali Balou.
References
- The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. Vital surveillances: The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)—China, 2020. China CDC Wkly. 2020; 2(8):113-22. [DOI:10.46234/ccdcw2020.032]
- Chauhan S. Comprehensive review of coronavirus disease 2019 (COVID-19). Biomed J. 2020; 43(4):334–40. [DOI:10.1016/j.bj.2020.05.023]
- World Health Organization (WHO). Coronavirus disease 2019 (COVID-19): Situation report-70. Geneva: World Health Organization; 2020. [Link]
- Ministry of Health and Medical Education. [Coronavirus arrives in Iran: Two people test positive in Qom (Persian)]. Tehran: Ministry of Health and Medical Education; 2020. [Link]
- Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet. 2020; 395(10223):507-13. [DOI:10.1016/S0140-6736(20)30211-7] [PMID] [PMCID]
- Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020; 382(18):1708-20. [DOI:10.1056/NEJMoa2002032] [PMID] [PMCID]
- Liu H, Xu JW, Ai Z, Yu Y, Yu B. Treatment seeking behavior and associated factors of suspected dengue fever among Shan people in eastern Shan special region IV, Myanmar: A cross-sectional study. BMC Health Serv Res. 2020; 20(1):318. [DOI:10.1186/s12913-020-05163-z] [PMID] [PMCID]
- Centers for Disease Control and Prevention. Cases Globally. 2019-nCoV situation. Georgia: Centers for Disease Control and Prevention; 2020.
- Antinyan A, Bassetti T, Corazzini L, Pavesi F. Trust in the healthcare system and COVID-19 treatment in the developing world”, survey and experimental evidence from Armenia. Univ Ca' Foscari Venice Dept Econs Res Pap Ser No. 10/WP/2020; [Unpublished]. [DOI:10.2139/ssrn.3619825]
- Taherian Z, Motamedi N. [Risk communication in COVID-19 pandemic crisis (Persian)]. J Isfahan Med Sch. 2020; 38(570):227-30. [DOI:10.22122/jims.v38i570.12912]
- Konarasinghe K. Modeling COVID-19 epidemic of USA, UK and Russia”. J New Front Healthcare Biol Sci. 2020; 1(1):1-14. [Link]
- Cheng VCC, Wong SC, Chen JHK, Yip CCY, Chuang VWM, Tsang OTY, et al. Escalating infection control response to the rapidly evolving epidemiology of the coronavirus disease 2019 (COVID-19) due to SARS-CoV-2 in Hong Kong. Infect Control Hosp Epidemiol. 2020; 41(5):493-8. [DOI:10.1017/ice.2020.58] [PMID] [PMCID]
- Singhal T. A review of coronavirus disease-2019 (COVID-19). Indian J Pediatr. 2020; 87(4):281-6. [DOI:10.1007/s12098-020-03263-6] [PMID] [PMCID]
- Türe Z, Alp E. Future pandemics: How can we be ready? Turk J Med Sci. 2022; 52(4):1400-3. [DOI:10.55730/1300-0144.5447] [PMID] [PMCID]
- Nkoka O, Chuang TW, Chen YH. Multilevel analysis of factors associated with treatment-seeking behaviors among caregivers with febrile children in Malawi. Am J Trop Med Hyg. 2019; 100(6):1454-65. [DOI:10.4269/ajtmh.18-0900] [PMID] [PMCID]
- Liu K, Fang YY, Deng Y, Liu W, Wang MF, Ma JP, et al. Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province. Chin Med J. 2020; 133(9):1025-31. [DOI:10.1097/CM9.0000000000000744] [PMID] [PMCID]
- Xiong Z, Fu L, Zhou H, Liu JK, Wang AM, Huang Y, et al. [Construction and evaluation of a novel diagnosis pathway for 2019-Corona virus disease (Chinese)]. Zhonghua Yi Xue Za Zhi. 2020; 100(16):1223-9. [DOI:10.3760/cma.j.cn112137-20200228-00499] [PMID]
- Hsu E, Zhu B, Ding Z. Allium fistulosum congee as a home remedy to ward off the corona virus at an early stage. Integr Med Res. 2020; 9(3):100463. [DOI:10.1016/j.imr.2020.100463] [PMID] [PMCID]
- Azam MNK, Mahamud RA, Hasan A, Jahan R, Rahmatullah M. Some home remedies used for treatment of COVID-19 in Bangladesh. J Med Plants. 2020; 8(4):27-32. [Link]
- Quandt SA, Sandberg JC, Grzywacz JG, Altizer KP, Arcury TA. Home remedy use among African American and white older adults. J Natl Med Assoc. 2015; 107(2):121-9. [DOI:10.1016/S0027-9684(15)30036-5] [PMID] [PMCID]
- Jordan RE, Adab P, Cheng KK. Covid-19: Risk factors for severe disease and death. BMJ. 2020; 368:m1198. [DOI:10.1136/bmj.m1198] [PMID]
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the chinese center for disease control and prevention. JAMA. 2020; 323(13):1239-42. [DOI:10.1001/jama.2020.2648] [PMID]
- Fang L, Karakiulakis G, Roth M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir Med. 2020; 8(4):e21. [DOI:10.1016/S2213-2600(20)30116-8] [PMID] [PMCID]
- Raoofi A, Takian A, Akbari Sari A, Olyaeemanesh A, Haghighi H, Aarabi M. COVID-19 pandemic and comparative health policy learning in Iran. Arch Iran Med. 2020; 23(4):220-34. [DOI:10.34172/aim.2020.02] [PMID]
- Majid S, Rahmat NA. Information needs and seeking behavior during the H1N1 virus outbreak. J Inf Sci Theory Pract. 2013; 1(1):42-53. [DOI:10.1633/JISTaP.2013.1.1.3]
- Lauer SA, Grantz KH, Bi Q, Jones FK, Zheng Q, Meredith HR, et al. The Incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application. Ann Intern Med. 2020; 172(9):577-82. [DOI:10.7326/M20-0504] [PMID] [PMCID]
- Cunningham AC, Goh HP, Koh D. Treatment of COVID-19: Old tricks for new challenges. Crit Care. 2020; 24(1):91. [DOI:10.1186/s13054-020-2818-6] [PMID] [PMCID]
Article Type: Original Contributions |
Subject:
Health Management
Received: 2023/11/10 | Accepted: 2024/02/28 | Published: 2024/04/1
Received: 2023/11/10 | Accepted: 2024/02/28 | Published: 2024/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
