

Volume 9, Issue 4 (10-2024)
CJHR 2024, 9(4): 225-236 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sarkar J, Sarkar C. Study of Role of Internet Access and Frontline Workers in Community-based Child Nutrition Programs for Budget Allocation of National Health Services. CJHR 2024; 9 (4) :225-236
URL: http://cjhr.gums.ac.ir/article-1-367-en.html
URL: http://cjhr.gums.ac.ir/article-1-367-en.html


1- Department of Life Sciences, University of Mumbai, Mumbai, India.
2- Department of Life Sciences, University of Mumbai, Mumbai, India. ,chiradeep.sarkar@gnkhalsa.edu.in
2- Department of Life Sciences, University of Mumbai, Mumbai, India. ,
Full-Text [PDF 792 kb]
(283 Downloads)
| Abstract (HTML) (1012 Views)
Full-Text: (618 Views)
Introduction
Malnutrition due to poor child-feeding practices increases vulnerability to diseases like diarrhea, malaria, and pneumonia. It is a reason for about 45% of deaths worldwide among children under five years [1]. More than 90% of such kind of child mortality are seen in sub-Saharan Africa and South Asia [2]. Malnutrition also affects cognitive development of the child [3].
Feeding decisions are influenced by various determinants like education of mother [4, 5], knowledge of feeding practice [6], and social and cultural factors [7]. The study carried out by World Health Organization (WHO) on feeding practices in 57 low- and middle-income countries (LMICs) highlights breastfeeding practices are improving worldwide but are still not as per the feeding recommendations framed by WHO and they are differed across the WHO regions [8]. Similar studies suggest constant efforts are needed to improve the feeding practices [9, 10].
In 2011, government of India has launched home based new born care (HBNC) program to bring down neonatal mortality and morbidity specifically in health care of deprived rural and remote areas. With one of the objectives of promoting breastfeeding, accredited social health activist (ASHA) workers were appointed for scheduled home visits. With the objective of improving health and nutrition of children in the age group of 3-15 months, home-based care for young child programme (HBYC) was launched by the government in 2018. This was part of the programs called the national health mission and POSHAN Abhiyan. One of the objectives of this program is counselling by ASHA workers for exclusive breastfeeding till six months and continued breastfeeding with adequate complementary feeding afterward [11]. The data by national family health survey (NFHS) (2019-21) would help us to identify how these programs have impacted the targeted population of the country in achieving the goal of an adequate diet.
Earlier studies indicate that to achieve health care delivery, health literacy, and public health broadband internet is necessary [12, 13]. Access to the internet significantly expands the average health condition and improves health inequality [14, 15]. The COVID-19 pandemic has shown our dependence on internet as an essential utility like water and electricity [16].
Broadband internet access is one of the most important determinants of health as many other social determinants like education, health care, food, income are based on it [17]. A study shows that women give lot of preference for internet health information [18, 19]. Over fifty percent of Indians (759 million) are active internet users and it is interesting to know that 57% of all new users were women in 2022 [20].
The Indian government has allocated 99243.69 million Indian Rupees (INR) for 2019-2020, 1023071.708 million INR for 2020-2021, and 1052765.58 million INR for 2021-2022 for improving reproductive and child health [21]. When allocated funds are not strategically managed, it reduces the quality and accessibility of health care and other services [22].
There is no study available as far as the role of the internet and child feeding practices especially with the government’s efforts under the programs like HBNC and HBYC are concerned. The status of internet access in urban and rural India for women needs to be studied. Understanding how access to the internet for women like ASHAs and lactating mothers can bring awareness into the child feeding practices can help us to frame the targeted interventions better. Therefore, this study has been designed to identify the role of technology like internet access to women population and community health workers in improving infant and young child feeding (IYCF) practices.
Materials and Methods
Type of the study
This is a secondary data analysis that was performed on the data related to ASHAs working in individual state or :union: territories for the national health mission (NHM) was obtained from Ministry of Health and Family Welfare (MoHFW) [23]. Data related to the percentage of women with internet access and children getting adequate diet was obtained from national family health survey-5 (NFHS-5) from MoHFW, Government of India [24].
The data provides information for 707 districts, 28 states, and 8 :union: territories (UTs). The survey work for the NFHS-5 was planned in two phases. The 1st phase was carried out for 17 states and 5 :union: territories from 17 June 2019 to 30 January 2020 and the 2nd phase has been completed in 11 states and 3 UTs from 2 January 2020 to 30 April 2021.
Study population
A population of 724,115 women in the age group of 15-49 years were covered in this study. Women population is divided into two sub-samples for study-urban and rural women. The population of children is also divided into urban and rural children. For better analysis of data, the country is divided into regions: 1) The northern region- has six states-Punjab, Himachal Pradesh, Haryana, Delhi, Uttarakhand, and Uttar Pradesh; 2) The five states of the southern region contains: Andhra Pradesh, Telangana, Karnataka, Tamil Nadu, and Kerala; 3) Eastern region- is consisting of four states like Bihar, Jharkhand, Odisha, and West Bengal, 4) Rajasthan, Maharashtra Gujarat and Goa are states of western India; 5) Madhya Pradesh and Chhattisgarh are part of central region, 6) North-East region includes-eight states viz. Manipur, Meghalaya, Mizoram, Nagaland Arunachal Pradesh, Assam, Sikkim and Tripura. :union: territories like Jammu & Kashmir, Ladakh, Andaman and Nicobar Islands, Chandigarh, Dadra and Nagar Haveli, Daman and Diu, Lakshadweep, and Puducherry are grouped as per their geographical locations.
We have targeted children getting an adequate diet in the age group of 6-23 months. Adequate diet is defined as breastfed children are getting 4 or more food groups and a minimum meal frequency. At the same time, non-breastfed children are fed with a minimum of 3 IYCF. That is, they are fed at least twice a day with other milk or milk products and minimum meal frequency. As per the data, the minimum meal frequency is, receiving solid or semi-solid food at least twice a day for breastfed infants who are 6-8 months old, and at least three times a day for breastfed children in the age group of 9-23 months.
Study approval
This study is based on the data available on the MoHFW website. This is publicly available dataset of the NFHS-5 surveys where there is no identifiable information on the participants. As per the data provided, the ethical approval for the NFHS-5 surveys is obtained from the ethics review board of the International Institute for Population Sciences, Mumbai, India. These surveys are reviewed and approved by the ICF Institutional Review Board, USA. Informed written consent for participation in this survey is obtained from the respondents during the survey. Each individual’s approval is sought before the patient interview, as per the consistent methodology followed in these national surveys.
Study variables
The primary outcome variable or dependent variable in this study is the percentage of children in the age group of 6-23 months getting an adequate diet. The independent variable or explanatory variable is the number of ASHA workers per state and the percentage of women getting internet access. The information on the percentage of children getting adequate diet, women getting internet access and ASHAs was obtained by asking ‘yes’ or ‘no’ questions orally.
Statistical analysis
A descriptive statistical analysis of the collected data was done. Mean, median, and range were calculated as per the standard formulas. The association between studies variables was explored using Pearson correlation coefficient and linear regression analysis. The Statistics Kingdom [25] was used for data analysis.
Results
The national level data showed that the children aged 6-23 months receiving an adequate diet is remarkably low in urban (12.3%) as well as in rural populations (11.0%). For the overall population, only 11.3% of children in the country are getting an adequate diet. Compared to NFHS-4 data (9.6%), the percentage of children receiving adequate diet is higher in NFHS-5 (11.3%) but still, it is far below the satisfactory level (Table 1, Figure 1).


The analysis of data for the northern region has shown Uttar Pradesh with an alarming number of urban (6.8%), rural (5.9%), and total (6.1%) children getting adequate diets. Jammu & Kashmir, Himachal Pradesh, Haryana, and Delhi are the states where rural children are more in number compared to urban counterparts who are getting adequate diets. In the rest of the states like Punjab, Uttarakhand, Uttar Pradesh, Ladakh, and Chandigarh urban children are higher in number who get adequate diet as compared to their rural counterparts. When compared to NFHS-4 data (23.5%), except for Jammu and Kashmir (13.6%) rest of all the states and :union: territories of the northern region have shown improvement in the number of children getting an adequate diet (Table 2).

The data analysis of the Northern region of India shows interesting figures. The state of Uttar Pradesh has the highest number (163407) of ASHAs in the region and a total of 30.6% of women have internet access but the number of children getting adequate diet is (6.1%) that was lowest in the region. On the contrary, Chandigarh which is :union: territory has the highest number of women with internet access (75.2%) as well as the highest number of children getting adequate diet (19.1%) in the region.
Children in rural populations of states like Telangana (9.7%), Karnataka (13.7%), Kerala (25.4%), and the :union: territory of Puducherry (31.9%) have adequate diets in age 6-23 months when compared to the urban children of these states. In states like Andhra Pradesh (16.7%), Tamil Nadu (17.9%), and :union: territories of Andaman & Nicobar (27.7%), and Lakshadweep (21.8%), higher urban children are getting adequate diets compared to rural ones. When NFHS-5 data of the southern region is compared with NFHS-4 data, states like Tamil Nadu (16.3%), Telangana (9.2%), and the :union: territory of Lakshadweep (19.0%) have shown a reduction in number of children getting adequate diet in 6-23 months of age.
The results of south India are similar to the northern region where the :union: territory of Puducherry with highest number of women with internet access (61.9%) and only 206 ASHAs have 22.9% of children with adequate diet. The state of Kerala has 61.1% of women with internet access but 30113 ASHAs have 23.5% of children with adequate diet (Table 3).

Compared to NFHS-4 data, the number of children getting adequate diets is improved in every state of the eastern region (Table 4). Barring the state of West Bengal, in the rest of the three states more rural children are getting adequate diets as compared to urban ones (Table 4). In the eastern region of India, the highest number of ASHAs were in the state of Bihar (89437), followed by West Bengal (61545), Odisha (46566), and Jharkhand (41312).

When NFHS-4 data is compared with NFHS-5 data, every state of the western region of India has shown an increase in several children getting adequate diets. In states of Goa and the :union: territories of Dadra, Nagar Haveli, Diu, and Daman have shown a greater number of rural children getting adequate diet compared to their urban counterparts (Table 5). The results of this (western) region of India are interesting, the state of Goa has no appointed ASHA workers. But here, the highest number of (73.7%) women have access to the internet, and the highest number of children (21.5%) have adequate diet in the region.

Compared to NFHS-4 data, Chhattisgarh has shown a decline in several children getting adequate diets but in the state of Madhya Pradesh, the number of children getting adequate diets has increased (Table 6). In both states, more urban children are getting adequate diets as compared to rural ones.

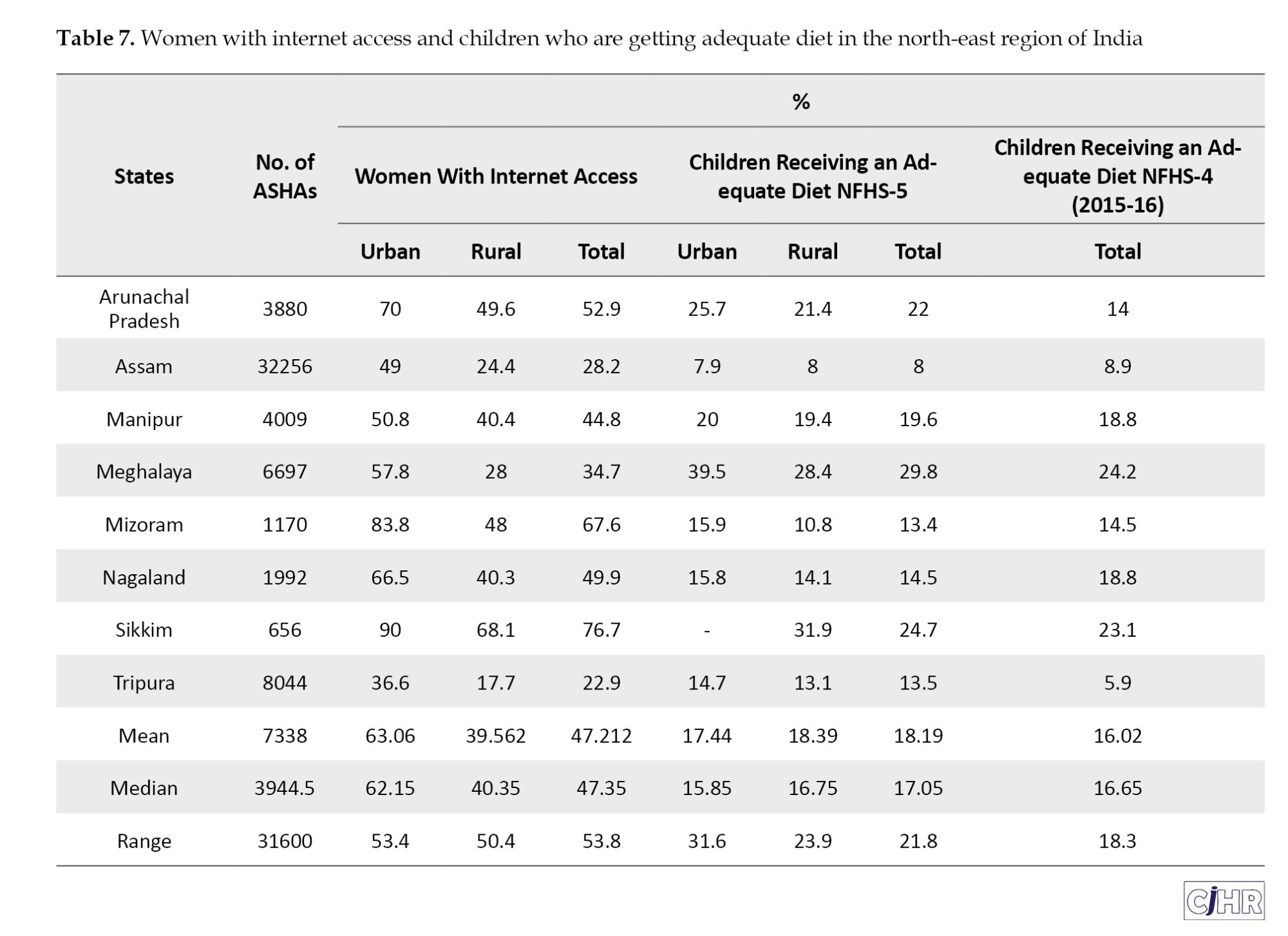
When comparing the study data with NFHS-4 data, the state of Mizoram (13.4%) is the only state that has shown a declining number of children getting adequate diet (Table 7). The state of Assam is the only state where rural children are more in number getting an adequate diet as compared to urban ones. In the rest of the states of the north-eastern region, higher the number of urban children get an adequate diet as compared to rural ones. In this region of the country, the state of Assam has shown the highest number (32256) of ASHAs, and a lower number (28.2%) of women with internet access. In such a situation, the state shows the lowest number (8%) of children with adequate diet.
The data for internet access to women in all the regions of the country have shown more urban women have access to the internet when compared to rural ones. A similar trend was noticed in the southern, eastern, western, and north-eastern regions of India. In the central region of the country, urban women are double in number for internet access as compared to rural ones. When the data was analyzed for the internet access to women in the northern region, except Delhi, the rest all the states showed a higher number of urban women with internet access than their rural counterparts. The internet access to women was lowest in eastern India (25.6%). Women in the northern region have the highest internet access (51.92%), followed by the northeast region (47.21%), west (43.22%), south (42.95%), and central (26.8%) region. When the region-wise data compared for children getting adequate diet (%), the North-east region has shown 18.19% children followed by south (16.56%), east (16.3%), north (14.98%), west (10.98%), and central (8.35%) region (Figure 2).

There was a significant direct relationship between percentage of women with internet access and children receiving adequate diet (R=0.513, P=0.001). In contrast, number of ASHA workers showed non-significant correlation with percent of children receiving adequate diet (R=-0.17, P=0.30). The multiple linear regression model predicting children receiving adequate diet with both independent variables revealed a beta coefficient of 0.23 (95% confidence interval (CI), 0.09%, 0.36%, P=0.002) for percentage of women with internet access and 0.09 (95% CI, -0.12%, 0.31%, P=0.377) for ASHA workers indicating percentage of women with internet access as an independent predictor of children receiving adequate diet. The model R-squared (R2) was 0.28.
Discussion
ASHA workers are appointed by the Indian Ministry of Health and Family Welfare. They are an all-female cadre of community health workers (CHWs) which are the link between the government or public health care facilities and the population and mobile is the only link between ASHAs and the population they are serving. Our study highlights the fact that just appointing ASHAs will not help to bring desired results but equipping them with internet access may bring the change.
Our study indicates that there are widespread variations in regional prevalence and determinants related to IYCF practices in India. Our results are similar to the earlier studies where the difference was observed in child feeding practices of various geographical or regional levels [26, 27]. By putting targeted national and regional efforts on vulnerable mothers like those with limited or no education and those with limited access to health facilities, feeding practices can be improved in geographically and culturally varied country like India.
The nutrition in the 1st 1000 days, from conception to two years plays important role in determining ideal health and development of the child [28]. Our study shows the percentage of children receiving an adequate diet is very low in the country. The numbers are better in urban areas if compared to rural ones. Earlier studies support the results of our study that a very smaller number of breastfeeding children in the age group of 6 to 23 months receives recommended diet and this situation is more or less same in the country in the past few years [29].
ASHAs are an important connecting bridge between the public or Government funded health services and the population in remote and rural areas, and even for the urban population who is in need. A review based on twelve studies highlights the challenges faced by these CHWs in fields like they are not provided with adequate supplies, minimum or no respect from the serving community, and lack of appropriate knowledge or communication skills. Along with this their serving communities are reluctant to change existing behaviours, show skepticism towards health messages of CHWs, and communities have limited health literacy [30].
The data analysis of the northern, southern, western, and northeastern regions of the country indicates that access to the internet for women may be one of the determinants of lessening malnutrition in children. The results of the state of Goa show that despite no appointed ASHAs, with a greater number of women with internet access, a greater number of children are having adequate diets.
A similar urban-rural divide which was noted in our study is also seen when the study was carried out in the children of less than 2 years of age in the Mysuru region of the Indian state of Karnataka [31]. Here, results have shown that 35% of rural children had poor, 57.1% of children get average and 7.9% of children get good IYCF practices. On the contrary, in urban parts of this region, 19.3% of children had poor diets, 55.0% of children had average diets and 25.7% of children had good diets. The study carried out in the children of Mysuru, Karnataka supports our findings that the overall feeding practices are poorer in rural than in urban areas [32].
As far as HBNC and HBYC programs are concerned, ASHAs are going door to door briefing families on breastfeeding and following adequate diet. There is one ASHA per 1000 population in rural areas and one for every 2500 persons in urban areas [33] the gap is still visible.
Our study results support earlier studies that proved the incidence of recommended child feeding practices differs significantly in the country as well as among various countries [33, 34].
Compared to NFHS-4 data (2015-16) the situation shows marginal improvement in NFHS-5 data. Despite robust programs like HBNC and HBYC where around 1.04 million ASHAs are perceiving one of the objectives of an adequate diet for every child, the prevalence of children with adequate nutrition is not encouraging. Our results are similar to the earlier studies [35, 36].
The urban-rural divide was observed in our study for women’s internet access. The possible reason behind this might be the low/no income of rural women as compared to urban ones as internet access rates increase with income [37]. Studies have already highlighted the importance of the internet as a source of health-related information [38, 39]. The gap in the internet for urban and rural women including ASHAs might be the reason for the gap noticed in children getting adequate diets at urban and rural levels.
Similar results were observed when the relation of child feeding practices with mass media like television, newspaper, and movies was studied in the Indian population [40]. This study highlights the selection of right medium of mass communication for intervention programs related to child nutrition can encourage recommended child feeding practices at a large scale. Specifically selecting a media to create mass awareness about different child feeding practices, specifically in urban-rural settings could help adapt intervention programs to influence recommended behaviours. The health information preferably provided in regional languages via internet access to mothers and ASHAs might bring the desired change.
ASHAs can be effective where the illiteracy rate is higher but, in the areas where the women are more educated, access to the internet will give better results for improving child nutrition and overall maternal and child nutrition/health. States with high women literacy like Kerala, Mizoram, Nagaland, Tripura, Sikkim, Manipur, etc should be given higher priority for internet access to women. In states like Rajasthan where illiteracy is high among women, more preference should be given to the ASHAs, especially by training and equipping them with online health information preferably in regional languages.
Before COVID-19, ASHAs were using personal mobiles with 2G/3G SIM but network availability in remote tribal areas was a challenge [41, 42]. Consequently, some of the states have decided to provide 4G SIM cards to ASHAs [43].
India has shown rapid advancement in internet penetration over the last decade but our study highlights, that there are still significant gender differences, regional differences, state-level differences, and urban and rural differences. Forty cities of India have more than a million population, whereas three hundred ninety six cities are with population between 1,00,000 and 1 million people, and 2500 Indian cities are with population between 10,000 to 1,00,000 population [44]. On a priority basis, the internet and electricity should be provided in these areas.
Conclusion
This study strengthens our understanding of various factors related to IYCF practices in India especially in the context of technology and community health workers. Overall penetration of internet technology in the country, urban-rural, and regional divide related to technology and IYCF is highlighted in the study. Improving IYCF practice awareness through penetration of the internet in rural and remote areas of the country can help to achieve the goals related to child nutrition and health. Barriers like illiteracy can be overcome through interpersonal counseling by ASHA workers. Strengthening the knowledge base of ASHAs may also be required to bring nationwide changes in sociocultural habits associated with IYCF practices.
Limitations and future research directions
This research study has highlighted some important findings which can help to improve child feeding practices, but at the same time it has some limitations too. These limitations need to work on in future research. First, the limitations which are related to any secondary data are also related to this data. There is no data available for the internet access to women population in urban as well as rural areas of India in NFHS-4 for comparison with data of NFHS-5. Internet technology has penetrated India over the period of time, and there is need to study the role of this technology access in public health. Second, due to data unavailability, the exact role of ASHAs in IYCF practices is not incorporated into the analysis. There is need to study, the relationship between internet access to ASHAs and improvement in various parameters of infant care with updated data. There are many factors affecting the IYCF practices in the population. Only one factor is studied in this work, and other related factor which can impact the results are not considered such as social and cultural barriers. It will be interesting to investigate the topic at microlevel determinants like the availability of electricity, and personal and family characteristics.
Ethical Considerations
Compliance with ethical guidelines
The ethical approval for the NFHS-5 surveys is obtained from the ethics review board of the International Institute for Population Sciences, Mumbai, India. These surveys are reviewed and approved by the ICF Institutional Review Board. Informed written consent for participation in this survey is obtained from the respondents during the survey. Patient consent for publication is not applicable.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, methodology, analysis, and investigation: Jaimini Sarkar; Supervision, and statistical analysis: Chiradeep Sarkar; Writing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors thank the Ministry of Health and Family Welfare, Government of India for the open data of national family health surveys which became foundation of this research study in public health.
References
Malnutrition due to poor child-feeding practices increases vulnerability to diseases like diarrhea, malaria, and pneumonia. It is a reason for about 45% of deaths worldwide among children under five years [1]. More than 90% of such kind of child mortality are seen in sub-Saharan Africa and South Asia [2]. Malnutrition also affects cognitive development of the child [3].
Feeding decisions are influenced by various determinants like education of mother [4, 5], knowledge of feeding practice [6], and social and cultural factors [7]. The study carried out by World Health Organization (WHO) on feeding practices in 57 low- and middle-income countries (LMICs) highlights breastfeeding practices are improving worldwide but are still not as per the feeding recommendations framed by WHO and they are differed across the WHO regions [8]. Similar studies suggest constant efforts are needed to improve the feeding practices [9, 10].
In 2011, government of India has launched home based new born care (HBNC) program to bring down neonatal mortality and morbidity specifically in health care of deprived rural and remote areas. With one of the objectives of promoting breastfeeding, accredited social health activist (ASHA) workers were appointed for scheduled home visits. With the objective of improving health and nutrition of children in the age group of 3-15 months, home-based care for young child programme (HBYC) was launched by the government in 2018. This was part of the programs called the national health mission and POSHAN Abhiyan. One of the objectives of this program is counselling by ASHA workers for exclusive breastfeeding till six months and continued breastfeeding with adequate complementary feeding afterward [11]. The data by national family health survey (NFHS) (2019-21) would help us to identify how these programs have impacted the targeted population of the country in achieving the goal of an adequate diet.
Earlier studies indicate that to achieve health care delivery, health literacy, and public health broadband internet is necessary [12, 13]. Access to the internet significantly expands the average health condition and improves health inequality [14, 15]. The COVID-19 pandemic has shown our dependence on internet as an essential utility like water and electricity [16].
Broadband internet access is one of the most important determinants of health as many other social determinants like education, health care, food, income are based on it [17]. A study shows that women give lot of preference for internet health information [18, 19]. Over fifty percent of Indians (759 million) are active internet users and it is interesting to know that 57% of all new users were women in 2022 [20].
The Indian government has allocated 99243.69 million Indian Rupees (INR) for 2019-2020, 1023071.708 million INR for 2020-2021, and 1052765.58 million INR for 2021-2022 for improving reproductive and child health [21]. When allocated funds are not strategically managed, it reduces the quality and accessibility of health care and other services [22].
There is no study available as far as the role of the internet and child feeding practices especially with the government’s efforts under the programs like HBNC and HBYC are concerned. The status of internet access in urban and rural India for women needs to be studied. Understanding how access to the internet for women like ASHAs and lactating mothers can bring awareness into the child feeding practices can help us to frame the targeted interventions better. Therefore, this study has been designed to identify the role of technology like internet access to women population and community health workers in improving infant and young child feeding (IYCF) practices.
Materials and Methods
Type of the study
This is a secondary data analysis that was performed on the data related to ASHAs working in individual state or :union: territories for the national health mission (NHM) was obtained from Ministry of Health and Family Welfare (MoHFW) [23]. Data related to the percentage of women with internet access and children getting adequate diet was obtained from national family health survey-5 (NFHS-5) from MoHFW, Government of India [24].
The data provides information for 707 districts, 28 states, and 8 :union: territories (UTs). The survey work for the NFHS-5 was planned in two phases. The 1st phase was carried out for 17 states and 5 :union: territories from 17 June 2019 to 30 January 2020 and the 2nd phase has been completed in 11 states and 3 UTs from 2 January 2020 to 30 April 2021.
Study population
A population of 724,115 women in the age group of 15-49 years were covered in this study. Women population is divided into two sub-samples for study-urban and rural women. The population of children is also divided into urban and rural children. For better analysis of data, the country is divided into regions: 1) The northern region- has six states-Punjab, Himachal Pradesh, Haryana, Delhi, Uttarakhand, and Uttar Pradesh; 2) The five states of the southern region contains: Andhra Pradesh, Telangana, Karnataka, Tamil Nadu, and Kerala; 3) Eastern region- is consisting of four states like Bihar, Jharkhand, Odisha, and West Bengal, 4) Rajasthan, Maharashtra Gujarat and Goa are states of western India; 5) Madhya Pradesh and Chhattisgarh are part of central region, 6) North-East region includes-eight states viz. Manipur, Meghalaya, Mizoram, Nagaland Arunachal Pradesh, Assam, Sikkim and Tripura. :union: territories like Jammu & Kashmir, Ladakh, Andaman and Nicobar Islands, Chandigarh, Dadra and Nagar Haveli, Daman and Diu, Lakshadweep, and Puducherry are grouped as per their geographical locations.
We have targeted children getting an adequate diet in the age group of 6-23 months. Adequate diet is defined as breastfed children are getting 4 or more food groups and a minimum meal frequency. At the same time, non-breastfed children are fed with a minimum of 3 IYCF. That is, they are fed at least twice a day with other milk or milk products and minimum meal frequency. As per the data, the minimum meal frequency is, receiving solid or semi-solid food at least twice a day for breastfed infants who are 6-8 months old, and at least three times a day for breastfed children in the age group of 9-23 months.
Study approval
This study is based on the data available on the MoHFW website. This is publicly available dataset of the NFHS-5 surveys where there is no identifiable information on the participants. As per the data provided, the ethical approval for the NFHS-5 surveys is obtained from the ethics review board of the International Institute for Population Sciences, Mumbai, India. These surveys are reviewed and approved by the ICF Institutional Review Board, USA. Informed written consent for participation in this survey is obtained from the respondents during the survey. Each individual’s approval is sought before the patient interview, as per the consistent methodology followed in these national surveys.
Study variables
The primary outcome variable or dependent variable in this study is the percentage of children in the age group of 6-23 months getting an adequate diet. The independent variable or explanatory variable is the number of ASHA workers per state and the percentage of women getting internet access. The information on the percentage of children getting adequate diet, women getting internet access and ASHAs was obtained by asking ‘yes’ or ‘no’ questions orally.
Statistical analysis
A descriptive statistical analysis of the collected data was done. Mean, median, and range were calculated as per the standard formulas. The association between studies variables was explored using Pearson correlation coefficient and linear regression analysis. The Statistics Kingdom [25] was used for data analysis.
Results
The national level data showed that the children aged 6-23 months receiving an adequate diet is remarkably low in urban (12.3%) as well as in rural populations (11.0%). For the overall population, only 11.3% of children in the country are getting an adequate diet. Compared to NFHS-4 data (9.6%), the percentage of children receiving adequate diet is higher in NFHS-5 (11.3%) but still, it is far below the satisfactory level (Table 1, Figure 1).
The analysis of data for the northern region has shown Uttar Pradesh with an alarming number of urban (6.8%), rural (5.9%), and total (6.1%) children getting adequate diets. Jammu & Kashmir, Himachal Pradesh, Haryana, and Delhi are the states where rural children are more in number compared to urban counterparts who are getting adequate diets. In the rest of the states like Punjab, Uttarakhand, Uttar Pradesh, Ladakh, and Chandigarh urban children are higher in number who get adequate diet as compared to their rural counterparts. When compared to NFHS-4 data (23.5%), except for Jammu and Kashmir (13.6%) rest of all the states and :union: territories of the northern region have shown improvement in the number of children getting an adequate diet (Table 2).
The data analysis of the Northern region of India shows interesting figures. The state of Uttar Pradesh has the highest number (163407) of ASHAs in the region and a total of 30.6% of women have internet access but the number of children getting adequate diet is (6.1%) that was lowest in the region. On the contrary, Chandigarh which is :union: territory has the highest number of women with internet access (75.2%) as well as the highest number of children getting adequate diet (19.1%) in the region.
Children in rural populations of states like Telangana (9.7%), Karnataka (13.7%), Kerala (25.4%), and the :union: territory of Puducherry (31.9%) have adequate diets in age 6-23 months when compared to the urban children of these states. In states like Andhra Pradesh (16.7%), Tamil Nadu (17.9%), and :union: territories of Andaman & Nicobar (27.7%), and Lakshadweep (21.8%), higher urban children are getting adequate diets compared to rural ones. When NFHS-5 data of the southern region is compared with NFHS-4 data, states like Tamil Nadu (16.3%), Telangana (9.2%), and the :union: territory of Lakshadweep (19.0%) have shown a reduction in number of children getting adequate diet in 6-23 months of age.
The results of south India are similar to the northern region where the :union: territory of Puducherry with highest number of women with internet access (61.9%) and only 206 ASHAs have 22.9% of children with adequate diet. The state of Kerala has 61.1% of women with internet access but 30113 ASHAs have 23.5% of children with adequate diet (Table 3).
Compared to NFHS-4 data, the number of children getting adequate diets is improved in every state of the eastern region (Table 4). Barring the state of West Bengal, in the rest of the three states more rural children are getting adequate diets as compared to urban ones (Table 4). In the eastern region of India, the highest number of ASHAs were in the state of Bihar (89437), followed by West Bengal (61545), Odisha (46566), and Jharkhand (41312).
When NFHS-4 data is compared with NFHS-5 data, every state of the western region of India has shown an increase in several children getting adequate diets. In states of Goa and the :union: territories of Dadra, Nagar Haveli, Diu, and Daman have shown a greater number of rural children getting adequate diet compared to their urban counterparts (Table 5). The results of this (western) region of India are interesting, the state of Goa has no appointed ASHA workers. But here, the highest number of (73.7%) women have access to the internet, and the highest number of children (21.5%) have adequate diet in the region.
Compared to NFHS-4 data, Chhattisgarh has shown a decline in several children getting adequate diets but in the state of Madhya Pradesh, the number of children getting adequate diets has increased (Table 6). In both states, more urban children are getting adequate diets as compared to rural ones.
When comparing the study data with NFHS-4 data, the state of Mizoram (13.4%) is the only state that has shown a declining number of children getting adequate diet (Table 7). The state of Assam is the only state where rural children are more in number getting an adequate diet as compared to urban ones. In the rest of the states of the north-eastern region, higher the number of urban children get an adequate diet as compared to rural ones. In this region of the country, the state of Assam has shown the highest number (32256) of ASHAs, and a lower number (28.2%) of women with internet access. In such a situation, the state shows the lowest number (8%) of children with adequate diet.
The data for internet access to women in all the regions of the country have shown more urban women have access to the internet when compared to rural ones. A similar trend was noticed in the southern, eastern, western, and north-eastern regions of India. In the central region of the country, urban women are double in number for internet access as compared to rural ones. When the data was analyzed for the internet access to women in the northern region, except Delhi, the rest all the states showed a higher number of urban women with internet access than their rural counterparts. The internet access to women was lowest in eastern India (25.6%). Women in the northern region have the highest internet access (51.92%), followed by the northeast region (47.21%), west (43.22%), south (42.95%), and central (26.8%) region. When the region-wise data compared for children getting adequate diet (%), the North-east region has shown 18.19% children followed by south (16.56%), east (16.3%), north (14.98%), west (10.98%), and central (8.35%) region (Figure 2).
There was a significant direct relationship between percentage of women with internet access and children receiving adequate diet (R=0.513, P=0.001). In contrast, number of ASHA workers showed non-significant correlation with percent of children receiving adequate diet (R=-0.17, P=0.30). The multiple linear regression model predicting children receiving adequate diet with both independent variables revealed a beta coefficient of 0.23 (95% confidence interval (CI), 0.09%, 0.36%, P=0.002) for percentage of women with internet access and 0.09 (95% CI, -0.12%, 0.31%, P=0.377) for ASHA workers indicating percentage of women with internet access as an independent predictor of children receiving adequate diet. The model R-squared (R2) was 0.28.
Discussion
ASHA workers are appointed by the Indian Ministry of Health and Family Welfare. They are an all-female cadre of community health workers (CHWs) which are the link between the government or public health care facilities and the population and mobile is the only link between ASHAs and the population they are serving. Our study highlights the fact that just appointing ASHAs will not help to bring desired results but equipping them with internet access may bring the change.
Our study indicates that there are widespread variations in regional prevalence and determinants related to IYCF practices in India. Our results are similar to the earlier studies where the difference was observed in child feeding practices of various geographical or regional levels [26, 27]. By putting targeted national and regional efforts on vulnerable mothers like those with limited or no education and those with limited access to health facilities, feeding practices can be improved in geographically and culturally varied country like India.
The nutrition in the 1st 1000 days, from conception to two years plays important role in determining ideal health and development of the child [28]. Our study shows the percentage of children receiving an adequate diet is very low in the country. The numbers are better in urban areas if compared to rural ones. Earlier studies support the results of our study that a very smaller number of breastfeeding children in the age group of 6 to 23 months receives recommended diet and this situation is more or less same in the country in the past few years [29].
ASHAs are an important connecting bridge between the public or Government funded health services and the population in remote and rural areas, and even for the urban population who is in need. A review based on twelve studies highlights the challenges faced by these CHWs in fields like they are not provided with adequate supplies, minimum or no respect from the serving community, and lack of appropriate knowledge or communication skills. Along with this their serving communities are reluctant to change existing behaviours, show skepticism towards health messages of CHWs, and communities have limited health literacy [30].
The data analysis of the northern, southern, western, and northeastern regions of the country indicates that access to the internet for women may be one of the determinants of lessening malnutrition in children. The results of the state of Goa show that despite no appointed ASHAs, with a greater number of women with internet access, a greater number of children are having adequate diets.
A similar urban-rural divide which was noted in our study is also seen when the study was carried out in the children of less than 2 years of age in the Mysuru region of the Indian state of Karnataka [31]. Here, results have shown that 35% of rural children had poor, 57.1% of children get average and 7.9% of children get good IYCF practices. On the contrary, in urban parts of this region, 19.3% of children had poor diets, 55.0% of children had average diets and 25.7% of children had good diets. The study carried out in the children of Mysuru, Karnataka supports our findings that the overall feeding practices are poorer in rural than in urban areas [32].
As far as HBNC and HBYC programs are concerned, ASHAs are going door to door briefing families on breastfeeding and following adequate diet. There is one ASHA per 1000 population in rural areas and one for every 2500 persons in urban areas [33] the gap is still visible.
Our study results support earlier studies that proved the incidence of recommended child feeding practices differs significantly in the country as well as among various countries [33, 34].
Compared to NFHS-4 data (2015-16) the situation shows marginal improvement in NFHS-5 data. Despite robust programs like HBNC and HBYC where around 1.04 million ASHAs are perceiving one of the objectives of an adequate diet for every child, the prevalence of children with adequate nutrition is not encouraging. Our results are similar to the earlier studies [35, 36].
The urban-rural divide was observed in our study for women’s internet access. The possible reason behind this might be the low/no income of rural women as compared to urban ones as internet access rates increase with income [37]. Studies have already highlighted the importance of the internet as a source of health-related information [38, 39]. The gap in the internet for urban and rural women including ASHAs might be the reason for the gap noticed in children getting adequate diets at urban and rural levels.
Similar results were observed when the relation of child feeding practices with mass media like television, newspaper, and movies was studied in the Indian population [40]. This study highlights the selection of right medium of mass communication for intervention programs related to child nutrition can encourage recommended child feeding practices at a large scale. Specifically selecting a media to create mass awareness about different child feeding practices, specifically in urban-rural settings could help adapt intervention programs to influence recommended behaviours. The health information preferably provided in regional languages via internet access to mothers and ASHAs might bring the desired change.
ASHAs can be effective where the illiteracy rate is higher but, in the areas where the women are more educated, access to the internet will give better results for improving child nutrition and overall maternal and child nutrition/health. States with high women literacy like Kerala, Mizoram, Nagaland, Tripura, Sikkim, Manipur, etc should be given higher priority for internet access to women. In states like Rajasthan where illiteracy is high among women, more preference should be given to the ASHAs, especially by training and equipping them with online health information preferably in regional languages.
Before COVID-19, ASHAs were using personal mobiles with 2G/3G SIM but network availability in remote tribal areas was a challenge [41, 42]. Consequently, some of the states have decided to provide 4G SIM cards to ASHAs [43].
India has shown rapid advancement in internet penetration over the last decade but our study highlights, that there are still significant gender differences, regional differences, state-level differences, and urban and rural differences. Forty cities of India have more than a million population, whereas three hundred ninety six cities are with population between 1,00,000 and 1 million people, and 2500 Indian cities are with population between 10,000 to 1,00,000 population [44]. On a priority basis, the internet and electricity should be provided in these areas.
Conclusion
This study strengthens our understanding of various factors related to IYCF practices in India especially in the context of technology and community health workers. Overall penetration of internet technology in the country, urban-rural, and regional divide related to technology and IYCF is highlighted in the study. Improving IYCF practice awareness through penetration of the internet in rural and remote areas of the country can help to achieve the goals related to child nutrition and health. Barriers like illiteracy can be overcome through interpersonal counseling by ASHA workers. Strengthening the knowledge base of ASHAs may also be required to bring nationwide changes in sociocultural habits associated with IYCF practices.
Limitations and future research directions
This research study has highlighted some important findings which can help to improve child feeding practices, but at the same time it has some limitations too. These limitations need to work on in future research. First, the limitations which are related to any secondary data are also related to this data. There is no data available for the internet access to women population in urban as well as rural areas of India in NFHS-4 for comparison with data of NFHS-5. Internet technology has penetrated India over the period of time, and there is need to study the role of this technology access in public health. Second, due to data unavailability, the exact role of ASHAs in IYCF practices is not incorporated into the analysis. There is need to study, the relationship between internet access to ASHAs and improvement in various parameters of infant care with updated data. There are many factors affecting the IYCF practices in the population. Only one factor is studied in this work, and other related factor which can impact the results are not considered such as social and cultural barriers. It will be interesting to investigate the topic at microlevel determinants like the availability of electricity, and personal and family characteristics.
Ethical Considerations
Compliance with ethical guidelines
The ethical approval for the NFHS-5 surveys is obtained from the ethics review board of the International Institute for Population Sciences, Mumbai, India. These surveys are reviewed and approved by the ICF Institutional Review Board. Informed written consent for participation in this survey is obtained from the respondents during the survey. Patient consent for publication is not applicable.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, methodology, analysis, and investigation: Jaimini Sarkar; Supervision, and statistical analysis: Chiradeep Sarkar; Writing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors thank the Ministry of Health and Family Welfare, Government of India for the open data of national family health surveys which became foundation of this research study in public health.
References
- Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013; 382(9890):427-51. [DOI:10.1016/S0140-6736(13)60937-X] [PMID]
- Lassi ZS, Rind F, Irfan O, Hadi R, Das JK, Bhutta ZA. Impact of Infant and Young Child Feeding (IYCF) nutrition interventions on breastfeeding practices, growth and mortality in low- and middle-income countries: Systematic review. Nutrition. 2020; 12(3):722. [DOI:10.3390/nu12030722] [PMID]
- Khandelwal S, Kondal D, Chakravarti AR, Dutta S, Banerjee B, Chaudhry M, et al. Infant young child feeding practices in an indian maternal-child birth cohort in Belagavi, Karnataka. Int J Environ Res Public Health. 2022; 19(9):5088. [DOI:10.3390/ijerph19095088] [PMID]
- Mehlawat U, Puri S, Rekhi TK, Yadav BS, Tiwari SK. A study on Infant and Young Child feeding practices of mothers visiting District Civil Hospital. J Pediatr Assoc India. 2018; 7(3):178. [Link]
- Neves PAR, Barros AJD, Gatica-Domínguez G, Vaz JS, Baker P, Lutter CK. Maternal education and equity in breastfeeding: Trends and patterns in 81 low- and middle-income countries between 2000 and 2019. Int J Equity Health. 2021; 20(1):20. [DOI:10.1186/s12939-020-01357-3] [PMID]
- Mekonnen M, Kinati T, Bekele K, Tesfa B, Hailu D, Jemal K. Infant and young child feeding practice among mothers of children age 6 to 23 months in Debrelibanos district, North Showa zone, Oromia region, Ethiopia. Plos One. 2021; 16(9):e0257758. [DOI:10.1371/journal.pone.0257758] [PMID]
- Kogade P, Gaidhane A, Choudhari S, Khatib MN, Kawalkar U, Gaidhane S, et al. Socio-cultural determinants of infant and young child feeding practices in rural India. Med Sci. 2019; 23(100):1015-22. [Link]
- Zong X, Wu H, Zhao M, Magnussen CG, Xi B. Global prevalence of WHO infant feeding practices in 57 LMICs in 2010-2018 and time trends since 2000 for 44 LMICs. ClinicalMedicine. 2021; 37:100971. [DOI:10.1016/j.eclinm.2021.100971] [PMID]
- Gatica-Domínguez G, Neves PAR, Barros AJD, Victora CG. Complementary feeding practices in 80 low- and middle-income countries: Prevalence and socioeconomic inequalities in dietary diversity, meal frequency, and dietary adequacy. J Nutr. 2021; 151(7):1956-64. [DOI:10.1093/jn/nxab088] [PMID]
- Choudhury S, Headey DD, Masters WA. First foods: Diet quality among infants aged 6-23 months in 42 countries. Food Policy. 2019; 88:101762. [DOI:10.1016/j.foodpol.2019.101762] [PMID]
- Ministry of Health and Family Welfare. National health mission. New Delhi: Ministry of Health and Family Welfare, Government of India; 2024.
- Estacio EV, Whittle R, Protheroe J. The digital divide: Examining socio-demographic factors associated with health literacy, access and use of the internet to seek health information. J Health Psychol. 2019; 24(12):1668-75.[DOI:10.1177/1359105317695429] [PMID]
- Raths D. Expanding internet access improves health outcomes [Internet]. 2020 [Updated June 2020]. Available from: [Link]
- Yu J, Meng S. Impacts of the internet on health inequality and healthcare access: A cross-country study. Front Public Health. 2022; 10:935608. [DOI:10.3389/fpubh.2022.935608] [PMID]
- Benda NC, Veinot TC, Sieck CJ, Ancker JS. Broadband internet access is a social determinant of health. Am J Public Health. 2020; 110(8):1123-5. [DOI:10.2105/AJPH.2020.305784] [PMID]
- Early J, Hernandez A. Digital disenfranchisement and COVID-19: Broadband Internet Access as a social determinant of health. Health Promot Pract. 2021; 22(5):605-10. [DOI:10.1177/15248399211014490]
- Bauerly BC, McCord RF, Hulkower R, Pepin D. Broadband access as a public health issue: The role of law in expanding broadband access and connecting underserved communities for better health outcomes. J Law Med Ethics. 2019; 47(2_suppl):39-42. [DOI:10.1177/1073110519857314] [PMID]
- Jiang Sh, Basnyat I, Liping Liu P. Factors influencing internet health information seeking in India: An application of the comprehensive model of information seeking. Int J Commun. 2021; 15:2047-68. [Link]
- Hallyburton A, Evarts LA. Gender and online health information seeking: A five survey meta-analysis. J ConsumHealth Internet. 2014; 18(2):128-42. [DOI:10.1080/15398285.2014.902268]
- Biswapriya B. Internet in India 2022 [internet]. 2023. [Updated 28 October 2024]. Available from: [Link]
- Press Information Bureau. Press Information Bureau, Government of India: Ministry of Health and Family Welfare. Delhi: Press Information Bureau; 2020. [Link]
- UNICEF. Public finance for children. New York: UNICEF; 2019. [Link]
- Press Information Bureau. Health Expenditure for Children. Delhi: Press Information Bureau; 2022. [Link]
- Ministry of Health and Family Welfare. National Family Health Survey (NFHS-5) 2019-21. New Delhi: Ministry of Health and Family Welfare, Government of India; 2022. [Link]
- Statistics online. Linear Regression Calculator [internet]. 2024. [Updated 20 October 2024]. Available from: [Link]
- Dhami MV, Ogbo FA, Osuagwu UL, Agho KE. Prevalence and factors associated with complementary feeding practices among children aged 6-23 months in India: A regional analysis. BMC Public Health. 2019; 19(1):1034. [DOI:10.1186/s12889-019-7360-6] [PMID]
- Bhati D, Tripathy A, Mishra PS. Srivastava S. Contribution of socio-economic and demographic factors to the trend of adequate dietary diversity intake among children (6-23 months): Evidence from a cross-sectional survey in India. BMC Nutr. 2022; 8(153). [DOI:10.1186/s40795-022-00655-z]
- Javalkar SR. Assessing WHO’s IYCF Indicators in Mangalore Taluk-A cross-sectional study. Indian J Public Health Res Dev. 2019; 10(6):76-80. [DOI:10.5958/0976-5506.2019.01242.7]
- Khan N, Mozumdar A, Kaur S. Dietary adequacy among young children in India: Improvement or Stagnation? An investigation from the National Family Health Survey. Food Nutr Bull. 2019; 40(4):471-87. [DOI:10.1177/0379572119859212] [PMID]
- Greuel M, Sy F, Bärnighausen T, Adam M, Vandormael A, Gates J, et al. Community health worker use of smart devices for health promotion: Scoping review. JMIR Mhealth Uhealth. 2023; 11:e42023. [DOI:10.2196/42023] [PMID]
- Lokesh N, Kulkarni P, Pragadesh R, Basheer S, Sunil Kumar D, Vanmathi A. Comparative study of feeding practices among children less than two years attending rural and urban primary health centers, Mysuru, Karnataka. Int J Community Med Public Health. 2023; 10(9):3219–25. [DOI:10.18203/2394-6040.ijcmph20232681]
- Muttreja P. ASHAs need better working conditions to be more effective [internet]. 2023. [Updated 28 October 2024]. Available from: [Link]
- Tariqujjaman M, Hasan MM, Mahfuz M, Ahmed T, Hossain M. Between and within-country variations in infant and young child feeding practices in South Asia. Int J Environ Res Public Health. 2022; 19(7):4350. [DOI:10.3390/ijerph19074350] [PMID]
- Benedict RK, Craig HC, Torlesse H, Stoltzfus RJ. Trends and predictors of optimal breastfeeding among children 0-23 months, South Asia: Analysis of national survey data. Matern Child Nutr. 2018; 14 Suppl 4(Suppl 4):e12698. [DOI:10.1111/mcn.12698] [PMID]
- Subramanian SV, William J. Putting food at the enter of India’s nutrition agenda [Internet]. 2020 [Updated 18 December 2020]. Available from: [Link]
- Modugu HR, Khanna R, Dash A, Manikam L, Parikh P, Benton L, et al. Influence of gender and parental migration on IYCF practices in 6-23-month-old tribal children in Banswara district, India: findings from the cross-sectional PANChSHEEEL study. BMC Nutr. 2022; ;8(1):10. [DOI:10.1186/s40795-021-00491-7] [PMID]
- Rubin R. Internet access as a social determinant of health. JAMA. 2021; 326(4):298. [DOI:10.1001/jama.2021.11733] [PMID]
- Amaral-Garcia S, Nardotto M, Propper C, Valletti T. Mums go online: Is the Internet changing the demand for healthcare? Munich: Center for Economic Studies and Ifo Institute (CESifo); 2019. [Link]
- Papp-Zipernovszky O, Horváth MD, Schulz PJ, Csabai M. Generation gaps in digital health literacy and their impact on health information seeking behavior and health empowerment in Hungary. Front Public Health. 2021; 9:635943. [DOI:10.3389/fpubh.2021.635943] [PMID]
- Dhawan D, Pinnamaneni R, Viswanath K. Association between mass media exposure and infant and young child feeding practices in India: A cross-sectional study. Sci Rep. 2023; 13(1):19353. [DOI:10.1038/s41598-023-46734-4] [PMID]
- Mander M. Connectivity becomes a problem for ASHAs [internet]. 2022. [Updated 28 October 2024]. Available from: [Link]
- Namrata Sindwani. Data hurdle: ASHA workers lose perks. The New Indian Express [Internet]. 2022 [Updated 15 August 2022]. Available from: [Link]
- Rajeev M. Postpaid 4G connections to Asha and ANMs for effective coordination with headquarters [Internet]. 2021 [Updated 17 May 2021]. Available from: [Link]
- Sarkar J. Are you staying in age ready city? Sci Report. 2022; 20-3. [Link]
Article Type: Original Contributions |
Subject:
Public Health
Received: 2024/02/26 | Accepted: 2024/08/28 | Published: 2024/10/1
Received: 2024/02/26 | Accepted: 2024/08/28 | Published: 2024/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
