

Volume 9, Issue 4 (10-2024)
CJHR 2024, 9(4): 237-248 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Kasmaei P, Yousefi P, Farmanbar R, Omidi S, Karimy M, Bab Eghbal S, et al . The Impact of Health Belief Model-based Education on Self-care Behaviors of Hypertensive Patients. CJHR 2024; 9 (4) :237-248
URL: http://cjhr.gums.ac.ir/article-1-382-en.html
URL: http://cjhr.gums.ac.ir/article-1-382-en.html
Parisa Kasmaei1 
 , Pegah Yousefi2 , Rabiollah Farmanbar1 , Saeed Omidi1 , Mahmood Karimy3 , Sedighe Bab Eghbal *4 , Maryam Shakiba5 , Morvarid Molaee6
, Pegah Yousefi2 , Rabiollah Farmanbar1 , Saeed Omidi1 , Mahmood Karimy3 , Sedighe Bab Eghbal *4 , Maryam Shakiba5 , Morvarid Molaee6
, Pegah Yousefi2 , Rabiollah Farmanbar1 , Saeed Omidi1 , Mahmood Karimy3 , Sedighe Bab Eghbal *4 , Maryam Shakiba5 , Morvarid Molaee6
1- Department of Health Education and Promotion, Research Center of Health and Environment, Faculty of Health, Guilan University of Medical Sciences, Rasht, Iran.
2- Deputy of Health, Guilan University of Medical Sciences, Rasht, Iran.
3- Social Determinants of Health Research Center, Saveh University of Medical Sciences, Saveh, Iran.
4- Department of Obstetrics and Gynecology, Reproductive Health Research Center, Faculty of Medicine, Al-Zahra Hospital, Guilan University of Medical Sciences, Rasht, Iran. ,Sedigheh.eghbal@yahoo.com
5- Department of Biostatistics and Epidemiology, Faculty of Health, Guilan University of Medical Sciences, Rasht, Iran.
6- Department of Psychology, Faculty of Humanities, Rasht Branch, Islamic Azad University, Rasht, Iran.
2- Deputy of Health, Guilan University of Medical Sciences, Rasht, Iran.
3- Social Determinants of Health Research Center, Saveh University of Medical Sciences, Saveh, Iran.
4- Department of Obstetrics and Gynecology, Reproductive Health Research Center, Faculty of Medicine, Al-Zahra Hospital, Guilan University of Medical Sciences, Rasht, Iran. ,
5- Department of Biostatistics and Epidemiology, Faculty of Health, Guilan University of Medical Sciences, Rasht, Iran.
6- Department of Psychology, Faculty of Humanities, Rasht Branch, Islamic Azad University, Rasht, Iran.
Full-Text [PDF 640 kb]
(847 Downloads)
| Abstract (HTML) (1029 Views)
Full-Text: (1123 Views)
Introduction
Hypertension is the most potent modifiable risk factor for heart failure, ischemic heart disease, cerebrovascular incidents, and chronic kidney diseases (CKDs) worldwide, and its harmful consequences continue to grow due to the continuous and global increase in the aging population [1, 2]. Mortality from cardiovascular and cerebrovascular diseases accounts for almost half of all deaths in developed regions and a quarter of deaths in developing regions in the 21st century [3]. Hypertension remains the most critical health issue in both developed and developing countries [4, 5], with its prevalence estimated to be 30% to 40% in different regions worldwide [6]. It is projected that the majority of hypertension will increase by 60%, affecting 1.56 billion people by 2025 [7, 8].
A meta-analysis comprising 29 studies in Iran reported the prevalence of hypertension to be 21.9% at. It noted that the prevalence was higher in Iran than other countries, warranting an investigation into this disease’s determinants and control strategies [9]. Based on studies in various areas of Iran, hypertension in adults is estimated to be between 17% and 25%, with a higher prevalence observed in men than in women [6].
High blood pressure is the force blood flow exerts on the blood vessel walls. It is influenced by several factors, including obesity, improper diet, excessive salt consumption, lack of physical activity, alcohol intake, and smoking [10, 11]. The American Heart Association states normal blood pressure should be below 120/80 mm Hg [12]. High blood pressure leads to inflammation and damage to the artery walls, resulting in fat accumulation and arteriosclerosis. Eventually, this leads to wear to the small and fragile arteries of internal organs, heart attacks, retinopathy, stroke, peripheral arterial diseases (PADs), and kidney failure [13].
The most significant characteristic of hypertension is its asymptomatic nature [14]. It can develop without noticeable symptoms for years, posing a significant barrier to the diagnosis and control of hypertension [8]. Effective management of high blood pressure is paramount to minimize the risk of complications. Patients’ self-care behaviors are crucial in managing high blood pressure, achieving successful hypertension management, and reducing its risk factors. Implementing effective self-care practices reduces hospitalization and healthcare costs while improving the overall quality of life [15, 16]. Despite evidence showing that lifestyle changes and adherence to therapeutic recommendations can effectively control high blood pressure and reduce mortality, many patients, especially in developing countries, do not engage in self-care behaviors, fail to comply with antihypertensive diets, neglect physical activity recommendations, or are unwilling to follow dietary guidelines [17]. In developing countries, lack of knowledge and insufficient implementation of self-care measures account for over three-quarters of hypertension cases [18].
Our research team found a lack of comprehensive studies on the status of high blood pressure self-care behaviors in hypertensive patients based on its determinants, including non-smoking, daily exercise, regular blood pressure measurement, maintaining a healthy weight, avoiding high-fat foods, using vegetable oils for cooking, adhering to medication schedules, consuming fruits and vegetables, and reducing salt intake [9].
Health professionals utilize health education and promotion models to encourage healthy practices, such as self-care behaviors. The health belief model (HBM) has been successful in this field and is employed to formulate and design preventive programs. The model assumes that personal beliefs shape appropriate and healthy behaviors, and modifying these beliefs can lead to behavioral changes [17, 19-21]. Using the HBM, we can gain better insights into the main determinants influencing individuals’ health decisions concerning hypertension prevention. Therefore, the present study employed the HBM as the primary framework for our research. Considering the high prevalence of hypertension in society and the necessity of preventive measures for patients, this study aims to determine the impact of an HBM-based educational intervention on self-care behaviors among hypertensive patients in Rasht County.
Materials and Methods
Design, procedure, and study sample
The present quasi-experimental pre-test-post-test study was conducted on hypertensive patients from rural health centers in Rasht County, North of Iran. The patients were selected using multi-stage sampling method, and then included in the study. Sample size was calculated based on the results of a previous study by Izadirad et al. [22]. Considering an effect size of 0.65 to calculate the difference in mean of blood pressure with 95% confidence interval and power of 80%, and accounting for a potential 20% dropout rate, a total of 48 samples were calculated in each group.
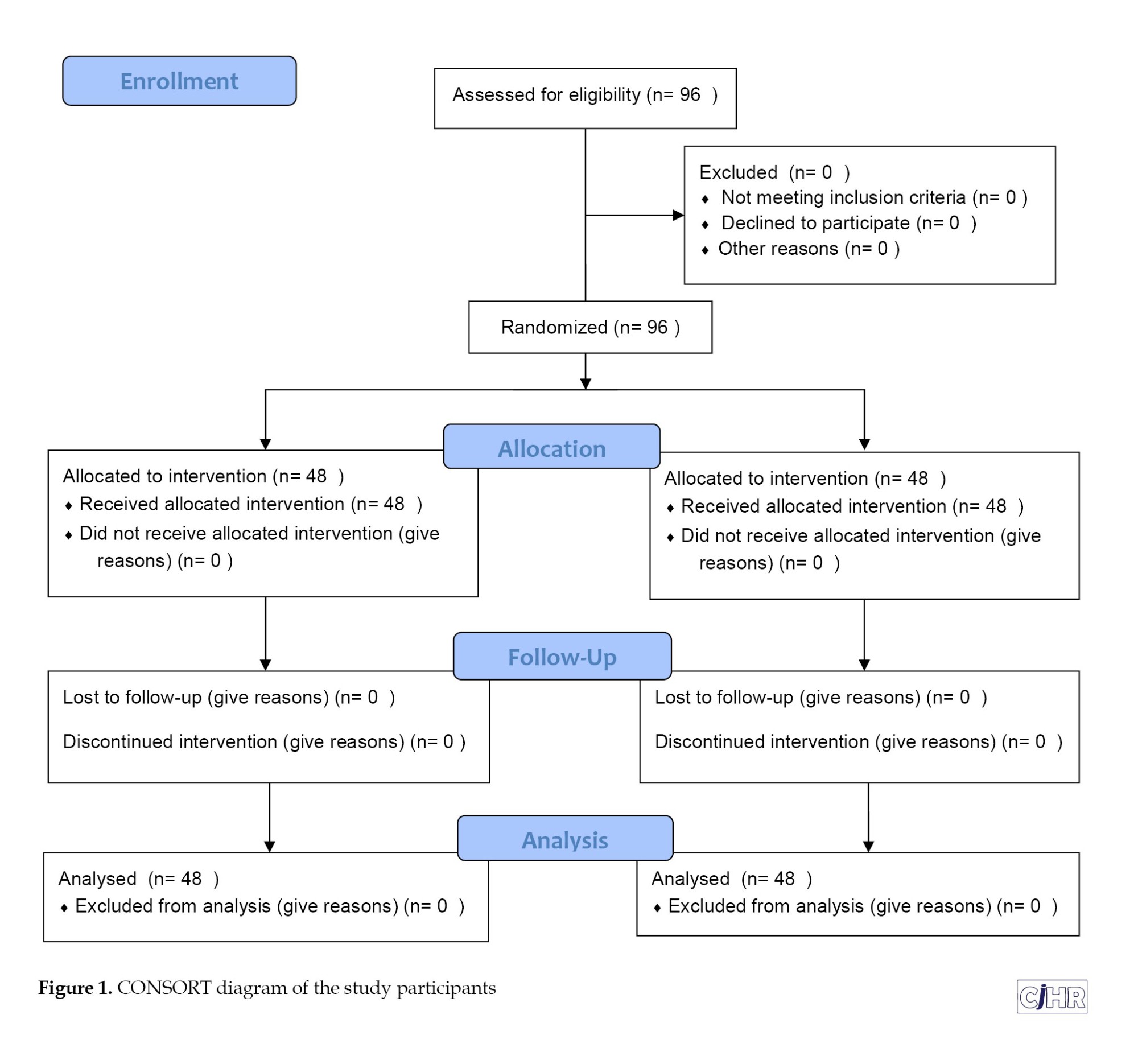
The multi-stage sampling method was conducted as follows: Firstly, a list of all 13 rural healthcare centers in Rasht County was prepared, and then using simple random sampling method one rural healthcare center was selected as the intervention and another as the control center. At each center, 48 samples were randomly selected from the list of patients with hypertension (Figure 1).
The inclusion criteria of the study were as follows: Being diagnosed with hypertension based on the medical records in the center, residing in a village, having at least 6 months since diagnosis, possessing the ability to understand and speak, expressing willingness to participate in the study, and not having any well-known physical or mental debilitating diseases. Exclusion criteria were defined as follows: absence in two training sessions, withdrawal from or unwillingness to participate in the study, migration from the village, or hospitalization during the study.
Measures
The data collection instrument comprised a valid and reliable [23] questionnaire with four parts. The 1st part covered demographic characteristics; the 2nd part consisted of a 12-question survey to assess awareness; the 3rd part included questions about HBM constructs, specifically perceived sensitivity (5 questions), perceived severity (6 questions), perceived benefits (7 questions), perceived barriers (5 questions), cues to action (7 questions), and perceived self-efficacy (10 questions). The 4th part addressed high blood pressure self-care behaviors with nine questions. The responses to the knowledge questions were graded as follows: “Yes” scored 3 points, “I do not know” scored 2 points, and “no” scored 1 point. The questions related to HBM constructs were measured on a 3-point Likert scale: “Agree” scored 3 points, “neutral” scored 2 points, and “disagree” scored 1 point. The self-care behavior questions were graded as follows: “No” scored 0 points, “yes” scored 1 point, and “Always” scored 2 points. A higher score indicated a better individual status in performing high blood pressure self-care behaviors.
The reliability of the questionnaire was assessed using Cronbach’s α test on 20 hypertensive patients (in addition to the groups participating in the study) who were demographically similar to the statistical population. The Cronbach’s α coefficients were as follows: 78% for perceived sensitivity, 72% for perceived severity, 82% for perceived benefits, 76% for perceived barriers, 73% for perceived self-efficacy, 81% for cues to action, 87% for knowledge, and 86% for self-care behaviors.
The study commenced after obtaining permission from the ethics committee of Guilan University of Medical Sciences. Additionally, all necessary legal permits were obtained from health centers, and informed consent was obtained from the participants after emphasizing the research purpose, the method of cooperation, and the advantages and disadvantages of participation. They were also assured that all data would be kept confidential and anonymous questionnaires would be used
Intervention
Educational needs assessment was conducted before the educational intervention using questionnaires in both the experimental and control groups. The patients completed the questionnaires, and the research team analyzed the data. The educational intervention was designed based on HBM and the pre-test results. It was then delivered in five 45-minute educational sessions, held once a week, with four groups of 12 participants each. The sessions incorporated lectures, questions and answers, group discussions, slide shows, practical demonstrations, and role-playing for the experimental group. Educational content was shared via WhatsApp in virtual groups for each class, and patients were encouraged to discuss their positive and negative experiences related to hypertension and healthy or unhealthy lifestyles. The educational content covered the definition of hypertension, its complications, causes, and risk factors (modifiable and non-changeable), as well as healthy lifestyle practices such as physical activity, proper diet, smoking cessation, weight loss, proper medication use, healthy nutrition, mental health improvement, and stress reduction methods. The same educational content was presented to all four experimental groups while ensuring confidentiality.
The control group received their routine educational programs and care during this period. Three months after the educational intervention, the initial questionnaire used in the pre-test was administered again to both groups and completed by the patients. Following the post-test, two educational sessions were conducted for the control group, and the entire educational content was provided to them to adhere to ethical guidelines.
Statistical analysis
Frequency distribution was employed to describe qualitative variables, while central indices, such as mean and dispersion indices, such as standard deviation, were used to describe quantitative variables. The subscale mean was divided by the number of each subscale items. The study utilized the Wilcoxon paired t-test to investigate the effect of education based on the HBM constructs in the intervention group before and after instruction. Additionally, the independent t-test and Mann-Whitney U test were employed to compare the mean changes in scores of the constructs before and after the intervention in both the control and intervention groups. The data were analyzed using SPSS software, version 21.
Results
In the intervention and control groups, most patients were over 60 (41.7%, control group: 47.9%). The majority of patients were female (intervention group: 85.4%, control group: 81.3%) and illiterate (intervention group: 66.7%, control group: 52.1%), with a family history of hypertension (intervention group: 66.7%, control group: 58.3%). The majority of participants were housewives (intervention group: 85.4%, control group: 81.3%) and married (intervention group: 91.7%, control group: 79.2%).
Regarding blood pressure, most participants had a systolic blood pressure of 140-159 mm Hg (intervention group: 68.8%, control group: 54.2%) and a diastolic blood pressure of 100-109 mm Hg in both groups (47.9%). The chi-square test did not show any statistically significant differences concerning demographic variables in both experimental and control groups (P>0.05) (Table 1).

There was no statistically significant difference in the mean score of knowledge and the HBM constructs (perceived sensitivity, severity, benefits, barriers, self-efficacy, and cues to action), self-care, and systolic and diastolic blood pressures between the intervention and control groups before the educational intervention (P>0.05). However, three months after the educational intervention, the mean score of knowledge, self-care, and all constructs of HBM, except for perceived barriers, significantly increased in the experimental group, and the mean blood pressure score increased decreased (P<0.05). In contrast, there were no statistically significant differences in the variables of the control group before and after the educational intervention (P>0.05). Additionally, there was a substantial difference between the mean scores of all variables in the experimental and control groups after education (P<0.05) (Tables 2 and 3).


Discussion
The present study evaluated the effects of educational interventions based on the HBM on high blood pressure self-care behaviors and blood pressure levels in hypertensive patients. Based on the results, the HBM-based intervention improved the mean score of knowledge and HBM constructs, leading to better patient blood pressure control. This result was consistent with studies by Kheiri et al. [24], Parmar et al. [25], Imtichan et al. [26], and Nematzad et al. [27]. Health professionals believe that designing educational programs using psychological theories of behavior, paying attention to the needs and characteristics of the target population [24], educating in health centers, and engaging and attracting active participation of participants in training classes [25] are practical steps in disease managment. The HBM, utilized as an educational framework in the present study, is an important model that seeks to identify the determinants of behavior and relevant processes in health-related fields. According to health education experts, HBM is a psychosocial model that can encourage healthy behavior by determining individuals’ belief-related factors that affect their behavior. Many hypertensive patients are in an unfavorable status regarding disease control and are exposed to complications. Relevant education based on this model can effectively create self-care and improve the patient’s health to control this critical problem [28, 29].
In our study, the intervention significantly increased the mean scores of perceived sensitivity and severity in the intervention group. The results of this study were consistent with studies by Zangiabadi et al. [30], Kamran et al. [31], and Obrikorang et al. [32] as the educational intervention increased perceived sensitivity and severity in hypertensive patients in their study. Patients must know that they are susceptible to complications of uncontrolled hypertension to adopt self-care behaviors. Higher perceptions of vulnerability and seriousness lead to more vital adherence to treatment [33]. After education, many hypertensive patients believe they will be exposed to it.
In the present study, the mean scores of the perceived benefits and barriers of the intervention group showed a significant change after the educational intervention. This finding was consistent with studies by Yazdanpanah et al. [34], Shen et al. [35], and Azadi et al., who reported that HBM-based educational programs increased perceived benefits and decreased perceived barriers in the intervention group [36]. Previous studies also indicated that reducing perceived barriers in patients for self-care behaviors helped them overcome barriers and prepare to perform regular and proper self-care behaviors. Further, increasing perceived benefits can boost the patients’ motivation and willingness towards self-care behaviors and adherence [32, 37, 38]. Khorsandi also reported that perceived barriers were the most critical factors affecting self-care behavior in hypertensive patients and the main reasons for refusing to follow the doctors’ prescriptions. Karimi’s study proved an inverse significant relationship between perceived barriers and self-care behaviors [28].
Our results indicated a significant difference between the mean scores of perceived self-efficacies in the experimental group before and three months after the educational intervention. Self-efficacy promotes proper acceptance of the disease by the patient due to increasing their ability and reducing anxiety and stress resulting from the inability to control the disease. Therefore, patients with higher self-efficacy become more committed and have better behavior [39]. Studies by Kim et al. [3], Azadi et al. [36], and Nematzad et al [27]. indicated that higher self-efficacy enhanced patient treatment adherence and self-care. Similarly, Karimi reported that self-efficacy significantly contributed to adopting self-care behaviors and was a mechanism to control chronic diseases [28]. The HBM developers also found that confidence in individuals’ ability to change outcomes (self-efficacy) was a key to health behavior change [40, 41].
In the present study, the mean score of cues to action significantly changed in the intervention group after the educational intervention. This result was consistent with studies by Yue et al. [38] and Zangiabadi et al. [30]. Behavioral scientists believe that cues to action are necessary to encourage individual engagement in healthy behavior. These stimuli are driving forces for the feeling of reaction in a person. Therefore, detecting such stimuli can encourage a person to act [39].
In the present study, the mean score of self-care behaviors increased from 1.18 before the intervention to 1.80 after the intervention in the intervention group, indicating a significant increase. This result was consistent with studies by Nematzad et al. [27]. Since managing chronic diseases is generally patient-based, and medical personnel and technologies are only used as monitoring tools, adopting self-care behavior is essential. The evidence indicates that self-care is learnable, and improving self-care behaviors is the 1st step to helping chronic patients control their diseases [42]. Previous studies showed that self-care effectively prevented hypertension complications like stroke, myocardial infarction, and chronic heart and kidney failures [43, 44]. Therefore, it seems that health professionals should adopt strategies that motivate, empower, and encourage hypertensive patients to make informed decisions and take responsibility for self-care to have effective interventions in hypertension control.
As a research limitation, we could not observe long-term persistence in participants’ behavior; the data collection about patients’ self-care behavior was based on self-report that can induce information bias and the patients may provide information that might differ from their actual behavior.
Conclusion
In the present study, the significant reduction in patients’ blood pressure indicates the successful effect of the intervention using the HBM on self-care and hypertension control in the population. Therefore, this educational approach is suggested as a practical, cost-effective, and safe therapeutic solution in hypertension control programs.
This research also emphasizes the need for greater attention to theory-based education in chronic diseases to promote a healthy lifestyle and proper behavioral habits. Education not only improves patients’ performance and prevents the spread of disease and its complications but also fosters the development of appropriate behavioral patterns and healthy lifestyles in society.
We recommend conducting new studies and interventions using other health behavior theories and educational strategies to evaluate their effectiveness in promoting patient self-care behavior.
Ethical Considerations
Compliance with ethical guidelines
The Ethics Committee of Guilan University of Medical Sciences approved the study protocol (Code: IR.GUMS.REC.1394.179).
Funding
This study was funded by Guilan University of Medical Sciences.
Authors' contributions
Conceptualization: Parisa Kasmaei and Sedighe Bab Eghbal; Methodology: Mahmood Karimy and Maryam Shakiba; Investigation: Morvarid Molaee; Data collection and writing the original draft: Pegah Yousefi; Review and editing: Rabiollah Farmanbar; Data analysis: Saeed Omidi; Supervision: Parisa Kasmaei.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors gratefully acknowledge the very helpful participation of the patients; without whose contribution the present study would not have been completed.
References
Hypertension is the most potent modifiable risk factor for heart failure, ischemic heart disease, cerebrovascular incidents, and chronic kidney diseases (CKDs) worldwide, and its harmful consequences continue to grow due to the continuous and global increase in the aging population [1, 2]. Mortality from cardiovascular and cerebrovascular diseases accounts for almost half of all deaths in developed regions and a quarter of deaths in developing regions in the 21st century [3]. Hypertension remains the most critical health issue in both developed and developing countries [4, 5], with its prevalence estimated to be 30% to 40% in different regions worldwide [6]. It is projected that the majority of hypertension will increase by 60%, affecting 1.56 billion people by 2025 [7, 8].
A meta-analysis comprising 29 studies in Iran reported the prevalence of hypertension to be 21.9% at. It noted that the prevalence was higher in Iran than other countries, warranting an investigation into this disease’s determinants and control strategies [9]. Based on studies in various areas of Iran, hypertension in adults is estimated to be between 17% and 25%, with a higher prevalence observed in men than in women [6].
High blood pressure is the force blood flow exerts on the blood vessel walls. It is influenced by several factors, including obesity, improper diet, excessive salt consumption, lack of physical activity, alcohol intake, and smoking [10, 11]. The American Heart Association states normal blood pressure should be below 120/80 mm Hg [12]. High blood pressure leads to inflammation and damage to the artery walls, resulting in fat accumulation and arteriosclerosis. Eventually, this leads to wear to the small and fragile arteries of internal organs, heart attacks, retinopathy, stroke, peripheral arterial diseases (PADs), and kidney failure [13].
The most significant characteristic of hypertension is its asymptomatic nature [14]. It can develop without noticeable symptoms for years, posing a significant barrier to the diagnosis and control of hypertension [8]. Effective management of high blood pressure is paramount to minimize the risk of complications. Patients’ self-care behaviors are crucial in managing high blood pressure, achieving successful hypertension management, and reducing its risk factors. Implementing effective self-care practices reduces hospitalization and healthcare costs while improving the overall quality of life [15, 16]. Despite evidence showing that lifestyle changes and adherence to therapeutic recommendations can effectively control high blood pressure and reduce mortality, many patients, especially in developing countries, do not engage in self-care behaviors, fail to comply with antihypertensive diets, neglect physical activity recommendations, or are unwilling to follow dietary guidelines [17]. In developing countries, lack of knowledge and insufficient implementation of self-care measures account for over three-quarters of hypertension cases [18].
Our research team found a lack of comprehensive studies on the status of high blood pressure self-care behaviors in hypertensive patients based on its determinants, including non-smoking, daily exercise, regular blood pressure measurement, maintaining a healthy weight, avoiding high-fat foods, using vegetable oils for cooking, adhering to medication schedules, consuming fruits and vegetables, and reducing salt intake [9].
Health professionals utilize health education and promotion models to encourage healthy practices, such as self-care behaviors. The health belief model (HBM) has been successful in this field and is employed to formulate and design preventive programs. The model assumes that personal beliefs shape appropriate and healthy behaviors, and modifying these beliefs can lead to behavioral changes [17, 19-21]. Using the HBM, we can gain better insights into the main determinants influencing individuals’ health decisions concerning hypertension prevention. Therefore, the present study employed the HBM as the primary framework for our research. Considering the high prevalence of hypertension in society and the necessity of preventive measures for patients, this study aims to determine the impact of an HBM-based educational intervention on self-care behaviors among hypertensive patients in Rasht County.
Materials and Methods
Design, procedure, and study sample
The present quasi-experimental pre-test-post-test study was conducted on hypertensive patients from rural health centers in Rasht County, North of Iran. The patients were selected using multi-stage sampling method, and then included in the study. Sample size was calculated based on the results of a previous study by Izadirad et al. [22]. Considering an effect size of 0.65 to calculate the difference in mean of blood pressure with 95% confidence interval and power of 80%, and accounting for a potential 20% dropout rate, a total of 48 samples were calculated in each group.
The multi-stage sampling method was conducted as follows: Firstly, a list of all 13 rural healthcare centers in Rasht County was prepared, and then using simple random sampling method one rural healthcare center was selected as the intervention and another as the control center. At each center, 48 samples were randomly selected from the list of patients with hypertension (Figure 1).
The inclusion criteria of the study were as follows: Being diagnosed with hypertension based on the medical records in the center, residing in a village, having at least 6 months since diagnosis, possessing the ability to understand and speak, expressing willingness to participate in the study, and not having any well-known physical or mental debilitating diseases. Exclusion criteria were defined as follows: absence in two training sessions, withdrawal from or unwillingness to participate in the study, migration from the village, or hospitalization during the study.
Measures
The data collection instrument comprised a valid and reliable [23] questionnaire with four parts. The 1st part covered demographic characteristics; the 2nd part consisted of a 12-question survey to assess awareness; the 3rd part included questions about HBM constructs, specifically perceived sensitivity (5 questions), perceived severity (6 questions), perceived benefits (7 questions), perceived barriers (5 questions), cues to action (7 questions), and perceived self-efficacy (10 questions). The 4th part addressed high blood pressure self-care behaviors with nine questions. The responses to the knowledge questions were graded as follows: “Yes” scored 3 points, “I do not know” scored 2 points, and “no” scored 1 point. The questions related to HBM constructs were measured on a 3-point Likert scale: “Agree” scored 3 points, “neutral” scored 2 points, and “disagree” scored 1 point. The self-care behavior questions were graded as follows: “No” scored 0 points, “yes” scored 1 point, and “Always” scored 2 points. A higher score indicated a better individual status in performing high blood pressure self-care behaviors.
The reliability of the questionnaire was assessed using Cronbach’s α test on 20 hypertensive patients (in addition to the groups participating in the study) who were demographically similar to the statistical population. The Cronbach’s α coefficients were as follows: 78% for perceived sensitivity, 72% for perceived severity, 82% for perceived benefits, 76% for perceived barriers, 73% for perceived self-efficacy, 81% for cues to action, 87% for knowledge, and 86% for self-care behaviors.
The study commenced after obtaining permission from the ethics committee of Guilan University of Medical Sciences. Additionally, all necessary legal permits were obtained from health centers, and informed consent was obtained from the participants after emphasizing the research purpose, the method of cooperation, and the advantages and disadvantages of participation. They were also assured that all data would be kept confidential and anonymous questionnaires would be used
Intervention
Educational needs assessment was conducted before the educational intervention using questionnaires in both the experimental and control groups. The patients completed the questionnaires, and the research team analyzed the data. The educational intervention was designed based on HBM and the pre-test results. It was then delivered in five 45-minute educational sessions, held once a week, with four groups of 12 participants each. The sessions incorporated lectures, questions and answers, group discussions, slide shows, practical demonstrations, and role-playing for the experimental group. Educational content was shared via WhatsApp in virtual groups for each class, and patients were encouraged to discuss their positive and negative experiences related to hypertension and healthy or unhealthy lifestyles. The educational content covered the definition of hypertension, its complications, causes, and risk factors (modifiable and non-changeable), as well as healthy lifestyle practices such as physical activity, proper diet, smoking cessation, weight loss, proper medication use, healthy nutrition, mental health improvement, and stress reduction methods. The same educational content was presented to all four experimental groups while ensuring confidentiality.
The control group received their routine educational programs and care during this period. Three months after the educational intervention, the initial questionnaire used in the pre-test was administered again to both groups and completed by the patients. Following the post-test, two educational sessions were conducted for the control group, and the entire educational content was provided to them to adhere to ethical guidelines.
Statistical analysis
Frequency distribution was employed to describe qualitative variables, while central indices, such as mean and dispersion indices, such as standard deviation, were used to describe quantitative variables. The subscale mean was divided by the number of each subscale items. The study utilized the Wilcoxon paired t-test to investigate the effect of education based on the HBM constructs in the intervention group before and after instruction. Additionally, the independent t-test and Mann-Whitney U test were employed to compare the mean changes in scores of the constructs before and after the intervention in both the control and intervention groups. The data were analyzed using SPSS software, version 21.
Results
In the intervention and control groups, most patients were over 60 (41.7%, control group: 47.9%). The majority of patients were female (intervention group: 85.4%, control group: 81.3%) and illiterate (intervention group: 66.7%, control group: 52.1%), with a family history of hypertension (intervention group: 66.7%, control group: 58.3%). The majority of participants were housewives (intervention group: 85.4%, control group: 81.3%) and married (intervention group: 91.7%, control group: 79.2%).
Regarding blood pressure, most participants had a systolic blood pressure of 140-159 mm Hg (intervention group: 68.8%, control group: 54.2%) and a diastolic blood pressure of 100-109 mm Hg in both groups (47.9%). The chi-square test did not show any statistically significant differences concerning demographic variables in both experimental and control groups (P>0.05) (Table 1).
There was no statistically significant difference in the mean score of knowledge and the HBM constructs (perceived sensitivity, severity, benefits, barriers, self-efficacy, and cues to action), self-care, and systolic and diastolic blood pressures between the intervention and control groups before the educational intervention (P>0.05). However, three months after the educational intervention, the mean score of knowledge, self-care, and all constructs of HBM, except for perceived barriers, significantly increased in the experimental group, and the mean blood pressure score increased decreased (P<0.05). In contrast, there were no statistically significant differences in the variables of the control group before and after the educational intervention (P>0.05). Additionally, there was a substantial difference between the mean scores of all variables in the experimental and control groups after education (P<0.05) (Tables 2 and 3).
Discussion
The present study evaluated the effects of educational interventions based on the HBM on high blood pressure self-care behaviors and blood pressure levels in hypertensive patients. Based on the results, the HBM-based intervention improved the mean score of knowledge and HBM constructs, leading to better patient blood pressure control. This result was consistent with studies by Kheiri et al. [24], Parmar et al. [25], Imtichan et al. [26], and Nematzad et al. [27]. Health professionals believe that designing educational programs using psychological theories of behavior, paying attention to the needs and characteristics of the target population [24], educating in health centers, and engaging and attracting active participation of participants in training classes [25] are practical steps in disease managment. The HBM, utilized as an educational framework in the present study, is an important model that seeks to identify the determinants of behavior and relevant processes in health-related fields. According to health education experts, HBM is a psychosocial model that can encourage healthy behavior by determining individuals’ belief-related factors that affect their behavior. Many hypertensive patients are in an unfavorable status regarding disease control and are exposed to complications. Relevant education based on this model can effectively create self-care and improve the patient’s health to control this critical problem [28, 29].
In our study, the intervention significantly increased the mean scores of perceived sensitivity and severity in the intervention group. The results of this study were consistent with studies by Zangiabadi et al. [30], Kamran et al. [31], and Obrikorang et al. [32] as the educational intervention increased perceived sensitivity and severity in hypertensive patients in their study. Patients must know that they are susceptible to complications of uncontrolled hypertension to adopt self-care behaviors. Higher perceptions of vulnerability and seriousness lead to more vital adherence to treatment [33]. After education, many hypertensive patients believe they will be exposed to it.
In the present study, the mean scores of the perceived benefits and barriers of the intervention group showed a significant change after the educational intervention. This finding was consistent with studies by Yazdanpanah et al. [34], Shen et al. [35], and Azadi et al., who reported that HBM-based educational programs increased perceived benefits and decreased perceived barriers in the intervention group [36]. Previous studies also indicated that reducing perceived barriers in patients for self-care behaviors helped them overcome barriers and prepare to perform regular and proper self-care behaviors. Further, increasing perceived benefits can boost the patients’ motivation and willingness towards self-care behaviors and adherence [32, 37, 38]. Khorsandi also reported that perceived barriers were the most critical factors affecting self-care behavior in hypertensive patients and the main reasons for refusing to follow the doctors’ prescriptions. Karimi’s study proved an inverse significant relationship between perceived barriers and self-care behaviors [28].
Our results indicated a significant difference between the mean scores of perceived self-efficacies in the experimental group before and three months after the educational intervention. Self-efficacy promotes proper acceptance of the disease by the patient due to increasing their ability and reducing anxiety and stress resulting from the inability to control the disease. Therefore, patients with higher self-efficacy become more committed and have better behavior [39]. Studies by Kim et al. [3], Azadi et al. [36], and Nematzad et al [27]. indicated that higher self-efficacy enhanced patient treatment adherence and self-care. Similarly, Karimi reported that self-efficacy significantly contributed to adopting self-care behaviors and was a mechanism to control chronic diseases [28]. The HBM developers also found that confidence in individuals’ ability to change outcomes (self-efficacy) was a key to health behavior change [40, 41].
In the present study, the mean score of cues to action significantly changed in the intervention group after the educational intervention. This result was consistent with studies by Yue et al. [38] and Zangiabadi et al. [30]. Behavioral scientists believe that cues to action are necessary to encourage individual engagement in healthy behavior. These stimuli are driving forces for the feeling of reaction in a person. Therefore, detecting such stimuli can encourage a person to act [39].
In the present study, the mean score of self-care behaviors increased from 1.18 before the intervention to 1.80 after the intervention in the intervention group, indicating a significant increase. This result was consistent with studies by Nematzad et al. [27]. Since managing chronic diseases is generally patient-based, and medical personnel and technologies are only used as monitoring tools, adopting self-care behavior is essential. The evidence indicates that self-care is learnable, and improving self-care behaviors is the 1st step to helping chronic patients control their diseases [42]. Previous studies showed that self-care effectively prevented hypertension complications like stroke, myocardial infarction, and chronic heart and kidney failures [43, 44]. Therefore, it seems that health professionals should adopt strategies that motivate, empower, and encourage hypertensive patients to make informed decisions and take responsibility for self-care to have effective interventions in hypertension control.
As a research limitation, we could not observe long-term persistence in participants’ behavior; the data collection about patients’ self-care behavior was based on self-report that can induce information bias and the patients may provide information that might differ from their actual behavior.
Conclusion
In the present study, the significant reduction in patients’ blood pressure indicates the successful effect of the intervention using the HBM on self-care and hypertension control in the population. Therefore, this educational approach is suggested as a practical, cost-effective, and safe therapeutic solution in hypertension control programs.
This research also emphasizes the need for greater attention to theory-based education in chronic diseases to promote a healthy lifestyle and proper behavioral habits. Education not only improves patients’ performance and prevents the spread of disease and its complications but also fosters the development of appropriate behavioral patterns and healthy lifestyles in society.
We recommend conducting new studies and interventions using other health behavior theories and educational strategies to evaluate their effectiveness in promoting patient self-care behavior.
Ethical Considerations
Compliance with ethical guidelines
The Ethics Committee of Guilan University of Medical Sciences approved the study protocol (Code: IR.GUMS.REC.1394.179).
Funding
This study was funded by Guilan University of Medical Sciences.
Authors' contributions
Conceptualization: Parisa Kasmaei and Sedighe Bab Eghbal; Methodology: Mahmood Karimy and Maryam Shakiba; Investigation: Morvarid Molaee; Data collection and writing the original draft: Pegah Yousefi; Review and editing: Rabiollah Farmanbar; Data analysis: Saeed Omidi; Supervision: Parisa Kasmaei.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors gratefully acknowledge the very helpful participation of the patients; without whose contribution the present study would not have been completed.
References
- Dominguez L, Veronese N, Barbagallo M. Magnesium and hypertension in old age. Nutrients. 2020; 13(1):139. [DOI:10.3390/nu13010139] [PMID]
- Kengne AP, Brière JB, Gudiña IA, Jiang X, Kodjamanova P, Bennetts L, et al. The impact of non-pharmacological interventions on adherence to medication and persistence in Dyslipidaemia and hypertension: A systematic review. Expert Rev Pharmacoecon Outcomes Res. 2024; 24(7):807-16. [DOI:10.1080/14737167.2024.2319598] [PMID]
- Kim HC, Cho SMJ, Lee H, Lee HH, Baek J, Heo JF. Korea hypertension fact sheet 2020: Analysis of nationwide population-based data. Clin Hypertens. 2021; 27(8):1-4. [DOI:10.1186/s40885-021-00166-2]
- Thiboutot J, Stuckey H, Binette A, Kephart D, Curry W, Falkner B, et al. A web-based patient activation intervention to improve hypertension care: Study design and baseline characteristics in the web hypertension study. Contemp Clin Trials. 2010; 31(6):634-46. [DOI:10.1016/j.cct.2010.08.012] [PMID]
- Nieuwlaat R, Schwalm JD, Khatib R, Yusuf S. Why are we failing to implement effective therapies in cardiovascular disease? Eur Heart J. 2013; 34(17):1262-9. [DOI:10.1093/eurheartj/ehs481] [PMID]
- Shojaeifar S, Shojaeifar H, Sobhani A. [The effect of educational intervention based on health belief model on blood pressure control in patients with hypertension referring to the clinic of Shariati Hospital in Isfahan 2017-2018 (Persian)]. Jundishapur Sci Med J. 2022; 20(6):506-17. [DOI:10.32598/JSMJ.20.6.1889]
- Baghianimoghadam M, Aivazi S, Mzloomy SS, Baghianimoghadam B. Factors in relation with self-regulation of Hypertension, based on the Model of Goal Directed behavior in Yazd city. J Med Life. 2011; 4(1):30-5. [PMID]
- KH SJ. Primary hypertension in internal medicine textbooks. Jakarta: Balai Penerbit FK UI; 2005.
- Chodosh J, Morton SC, Mojica W, Maglione M, Suttorp MJ, Hilton L, et al. Meta-analysis: Chronic disease self-management programs for older adults. Ann Intern Med. 2005; 143(6):427-38. [DOI:10.7326/0003-4819-143-6-200509200-00007]
- Hatefnia E, Kimiafar M, Moghimbeigi A, Safari-Moradabadi A. Factors predicting physical activity behaviors related to hypertension in overweight male employees: Application of Health Belief Model. Health Educ Health Promot. 2023; 11(2):311-6. [Link]
- Komaç F, Duru P. The effect of education based on a health belief model and motivational interviews on cardiovascular disease risk factors and healthy lifestyle behaviour changes in patients with essential hypertension: A randomized controlled trial. Patient Educ Couns. 2024; 120:108126. [DOI:10.1016/j.pec.2023.108126] [PMID]
- Hazavehei S, Dashti S, Moeini B, Faradmal J, Shahrabadi R, Yazdi AH. [Factors related to self-care behaviors in hypertensive individuals based on Health Belief Model (Persian)]. Koomesh.2015; 17(1):37-44. [Link]
- Perez V, Chang ET. Sodium-to-potassium ratio and blood pressure, hypertension, and related factors. Adv Nutr. 2014; 5(6):712-41. [DOI:10.3945/an.114.006783] [PMID]
- Hatami H, Razavi SM, Eftekhar Ardabili H, Maglesi F, Sayed Nozadi MJ. [Text book of public health (Persian)]. Tehran: Argmand; 2019. [Link]
- Esen K, Kolcu M. The relationship between health literacy and self-care management in patients with hypertension attending primary healthcare centers. J Public Health. 2022; 32(2):175-83. [DOI:10.1007/s10389-022-01801-4]
- Avegno KS, Roberson KB, Onsomu EO, Edwards MF, Dean EL, Bertoni AG. Evaluating a telephone and home blood pressure monitoring intervention to improve blood pressure control and self-care behaviors in adults with low-socioeconomic status. Int J Environ Res Public Health. 2023; 20(7):5287. [DOI:10.3390/ijerph20075287] [PMID]
- Glanz K, Rimer BK, Viswanath K. Health behavior and health education theory, research, and practice. San Francisco: Jossey-Bass; 2008. [Link]
- Melaku T, Bayisa B, Fekeremaryam H, Feyissa A, Gutasa A. Self-care practice among adult hypertensive patients at ambulatory clinic of tertiary teaching Hospital in Ethiopia: A cross-sectional study. J Pharm Policy Pract. 2022; 15(1):23. [DOI:10.1186/s40545-022-00421-3] [PMID]
- Bensley RJ, Brookins-Fisher J. Community health education methods: A practical guide. New York: Jones and Bartllet publisher; 2003. [Link]
- Hayden J. Introduction to health behavior theory. Massachusetts: Jones & Bartlett Learning; 2009. [Link]
- Butler JT. Principles of health education and health promotion. Belmon: Wadsworth Publication; 2001. [Link]
- Izadirad H, Masoudi G R, Zareban I. [The effect of family counseling on blood pressure on patients with hypertension (Persian)]. J Health. 2015; 6 (2):211-7. [DOI:10.20286/jech-02036]
- Zareban I, Araban M, Rohani MR, Karimy M, Zamani-Alavijeh F, Babanejad M, et al. High blood pressure self-care among hypertensive patients in Iran: A theory-driven study. J Hum Hypertens. 2022; 36(5):445-52. [DOI:10.1038/s41371-020-00429-9] [PMID]
- Kheiri M, Khani Jeihooni A, Alkamel A, Afzali Harsini P. The effect of educational intervention based on the health belief model on the promotion of cardiovascular disease (CVD) preventive behaviors among subjects referred to health centers in Fasa city (Fars province, Iran). Kontakt, 2019. 21(2):206-13. [DOI:10.32725/kont.2019.021]
- Parmar P, Rathod GB, Rathod S, Goyal R, Aggarwal S, Parikh A. Study of knowledge, attitude and practice of general population of Gandhinagar towards hypertension. Int J Curr Microbiol Appl Sci. 2014; 3(8):680-5. [Link]
- Imtichan SN, Tamtomo D, Sulaeman ES. Path analysis: Application of health belief model on the determinants of clean and healthy behavior among elderly with hypertension. J Health Promot Behav. 2019; 4(2):110-20. [DOI:10.26911/thejhpb.2019.04.02.03]
- Nematzad P, Pourghane P, Besharati F, Gholami-Chaboki B. Effects of health belief model in promoting self-care behaviors among hypertensive older adults. J Educ Health Promot. 2023; 12(1):208. [DOI:10.4103/jehp.jehp_689_22]
- Zareban I, Niknami S, Hidarnia A, Rakhshani F, Shamsi M, Karimy M. Effective intervention of self-care on glycaemia control in patients with type 2 diabetes. Iran Red Crescent Med J. 2014; 16(12):e8311. [DOI:10.5812/ircmj.8311] [PMID]
- Eghbal SB, Karimy M, Kasmaei P, Roshan ZA, Valipour R, Attari SM. Evaluating the effect of an educational program on increasing cervical cancer screening behavior among rural women in Guilan, Iran. BMC Womens Health. 2020; 20(1):149. [DOI:10.1186/s12905-020-01020-7] [PMID]
- Zangiabadi A, Shah Esmaili A, Ahmady Tabatabaei V, Movahed E, SHhankestani H. Factors regarding adherence to medication in patients with hypertension based on health belief model in the South of Kerman, Iran, in 2019. J CommunHealth Res. 2022; 11(2):82-90. [DOI:10.18502/jchr.v11i2.9995]
- Kamran A, Ahari SS, Biria M, Malpour A, Heydari H. Determinants of patient’s adherence to hypertension medications: Application of health belief model among rural patients. Ann Med Health Sci Res. 2014; 4(6):922-7. [Link]
- Obirikorang Y, Obirikorang C, Acheampong E, Odame Anto E, Gyamfi D, Philip Segbefia S, et al. Predictors of noncompliance to antihypertensive therapy among hypertensive patients Ghana: application of health belief model. Int J Hypertens. 2018; 2018(1):4701097.[DOI:10.1155/2018/4701097]
- Peltzer K. Health beliefs and prescription medication compliance among diagnosed hypertension clinic attenders in a rural South African Hospital. Curationis. 2004; 27(3):15-23. [DOI:10.4102/curationis.v27i3.994] [PMID]
- Yazdanpanah Y, Saleh Moghadam AR, Mazlom SR, Haji Ali Beigloo R, Mohajer S. Effect of an educational program based on health belief model on medication adherence in elderly patients with hypertension. Evid Based Care J. 2019; 9(1):52-62. [DOI:10.22038/ebcj.2019.35215.1895]
- Shen Y, Wang TT, Gao M, Hu K, Zhu XR, Zhang X, et al. [Effectiveness evaluation of health belief model-based health education intervention for patients with hypertension in community settings (Chinese)]. Zhonghua Yu Fang Yi Xue Za Zhi. 2020; 54(2):155-9. [PMID]
- Azadi NA, Ziapour A, Lebni JY, Irandoost SF, Abbas J, Chaboksavar F. The effect of education based on health belief model on promoting preventive behaviors of hypertensive disease in staff of the Iran University of Medical Sciences. Arch Public Health. 2021; 79(1):69. [DOI:10.1186/s13690-021-00594-4] [PMID]
- Attamimy HB, Qomaruddin MB. [Aplikasi health belief model pada perilaku pencegahan demam berdarah dengue (Indonesian)]. J Promkes. 2017; 5(2):245. [DOI:10.20473/jpk.V5.I2.2017.245-255]
- Yue Z, Li C, Weilin Q, Bin W. Application of the health belief model to improve the understanding of antihypertensive medication adherence among Chinese patients. Patient Educ Couns. 2015; 98(5):669-73. [DOI:10.1016/j.pec.2015.02.007] [PMID]
- Setiyaningsih R, Tamtomo D, Suryani N. Health belief model: Determinants of hypertension prevention behavior in adults at community health center, sukoharjo, central java. J Health Promot Behav. 2016; 1(3):160-70. [DOI:10.26911/thejhpb.2016.01.03.03]
- Onoruoiza SI, Musa A, Umar BD, Kunle YS. Using health beliefs model as an intervention to non compliance with hypertension information among hypertensive patient. J Humanities Soc Sci. 2015; 20(9):11-16. [Link]
- Karimy M, Higgs P, Abadi SS, Armoon B, Araban M, Rouhani MR, et al. Oral health behavior among school children aged 11-13 years in Saveh, Iran: An evaluation of a theory-driven intervention. BMC Pediatr. 2020; 20(1):476. [DOI:10.1186/s12887-020-02381-6] [PMID]
- Shabibi P, Zavareh MSA, Sayehmiri K, Qorbani M, Safari O, Rastegarimehr B, et al. Effect of educational intervention based on the Health Belief Model on promoting self-care behaviors of type-2 diabetes patients. Electron Physician. 2017; 9(12):5960-8. [DOI:10.19082/5960] [PMID]
- Khader IA, Malak MZ, Asia M, Jallad M, Zahran H. Factors correlating with self-care behaviors among patients with coronary artery disease: A cross-sectional study. Contemp Nurse. 2023; 59(3):189-201. [DOI:10.1080/10376178.2023.2220424] [PMID]
- Ma C. An investigation of factors influencing self-care behaviors in young and middle-aged adults with hypertension based on a health belief model. Heart Lung. 2018; 47(2):136-41. [DOI:10.1016/j.hrtlng.2017.12.001] [PMID]
Article Type: Original Contributions |
Subject:
Health Education and Promotion
Received: 2024/05/17 | Accepted: 2024/07/20 | Published: 2024/10/1
Received: 2024/05/17 | Accepted: 2024/07/20 | Published: 2024/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
