

Volume 10, Issue 1 (1-2025)
CJHR 2025, 10(1): 1-20 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shahabi M, Hasani J, Asadpour M. Factors Influencing Rumination in Post-traumatic Growth: A Systematic Review and Meta-analysis. CJHR 2025; 10 (1) :1-20
URL: http://cjhr.gums.ac.ir/article-1-393-en.html
URL: http://cjhr.gums.ac.ir/article-1-393-en.html


1- Department of Psychology, School of Humanities, Shahid Motahari University, Tehran, Iran. , mn_shahabi@motahari.ac.ir
2- Department of Clinical Psychology, School of Psychology and Education, Kharazmi University of Tehran, Teheran, Iran.
3- Department of General Psychology, School of Psychology, University of Vienna, Vienna, Austria.
2- Department of Clinical Psychology, School of Psychology and Education, Kharazmi University of Tehran, Teheran, Iran.
3- Department of General Psychology, School of Psychology, University of Vienna, Vienna, Austria.
Keywords: Posttraumatic growth, Rumination disorder, Deliberate rumination (DR), Gender differences, Trauma
Full-Text [PDF 894 kb]
(734 Downloads)
| Abstract (HTML) (831 Views)
Full-Text: (633 Views)
Introduction
understanding the factors contributing to post-traumatic growth (PTG) is essential for creating effective interventions and support systems for trauma survivors. Rumination, involving repetitive and intrusive thoughts about past events, has been linked to both increased distress and growth following trauma. However, the relationship between rumination and PTG remains complex. This study addresses this gap through a systematic review and meta-analysis, examining the association between rumination and PTG across diverse study designs and populations.
Traumatic events are unfortunately prevalent worldwide [1] and people respond differently to them. The available data suggests that at least a minority of people who have experienced trauma, e.g. earthquake, cancer, and traumatic experience reported meaningful levels of personal growth [2-4]. Such that some individuals experience personal growth and positive changes after experiencing trauma [5]. PTG refers to positive changes such as feeling strength and wisdom, increasing value to friends and family, and finding a fresh appreciation for each new day, that result from struggling to cope with a traumatic event [6, 7].
Moreover, it is important to mention that the positive changes or growth are not results of the event itself, but rather results of the struggle to cope with it. In this context, various strategies exist to cope with trauma, yet rumination may significantly influence the process of developing PTG [8]. Rumination is a cognitive process that repetitively and passively focuses on the meaning, causes, and consequences of negative emotions [9, 10].
The PTG model [11] suggests that people may review their personal belief systems and think regularly about traumatic events, which may include two forms of rumination: Intrusive and deliberate. Due to Zhou and colleagues [12] intrusive and deliberate ruminations are two different functional forms that may play different roles in posttraumatic psychology. Intrusive rumination (IR) refers to the negative focus on trauma-related cues or negative mood and has a complex relationship with PTG. While some studies found that IR provides a basis for further cognitive processing of PTG [13-15], others found no significant correlation between IR and PTG [17-19]. Deliberate rumination (DR), on the other hand, may facilitate individuals to reconstruct their understanding of the post-traumatic world and realize PTG [20]. Results have suggested that DR is an important predictive factor for PTG [21-28].
Calhoun and colleagues [29] pointed out that DR refers to one’s deliberate reexamining and contemplation of the traumatic event and traumatic-related DR can help individuals think positively about the meaning associated with trauma, facilitate themselves to reconstruct their understanding about the post-traumatic world and facilitate the realization of PTG [20]. Therefore, however, the relationship between rumination and PTG is complex, with some studies showing positive relationships between DR and IR and PTG [29-38], while others show a negative relationship between IR and PTG [4, 36-38].
This statement highlights the findings of several meta-analyses related to the correlation between positive aspects of emotion regulation strategies and PTG. The studies mentioned suggest that acceptance and reappraisal are positively correlated with PTG, while acceptance coping yielded the smallest effect size. Additionally, the meta-analysis by Prati and Pietrantoni [39] found that religious coping and positive reappraisal coping produced the largest effect sizes. Furthermore, the meta-analysis by Shiyko et al. [40] showed that change in spirituality had a medium to large effect size on PTG. A systematic review and meta-analysis by Gower et al. [41] revealed that downward comparison bias, positive attention bias, and growth beliefs had stronger correlations with perceived PTG than did defensiveness, memory bias, and social desirability bias. However, while meta-analytic data from traumatized individuals suggest that emotion regulation problems are associated with post-traumatic stress disorder (PTSD); this has yet to be studied in the context of PTG.
Allen and colleagues [42] conducted a meta-analysis exploring the profound effects of trauma on core beliefs and the ensuing process of PTG via rumination. Their study investigates the links between event-related IR and DR and PTG while considering moderating factors like age, time elapsed since trauma, and the nature of the traumatic experience. Their analysis revealed a significant association between retrospective DR soon after trauma and PTG. However, IR displayed non-significant and variable associations. These findings emphasize the importance of promoting deliberate cognitive processing among trauma survivors to encourage PTG, highlighting the necessity for longitudinal research into the temporal role of event-related rumination in PTG development. They identified 46 studies up to May 1, 2021, involving 12,048 participants. The study analyzed 46 studies involving 12,048 participants up to May 1, 2021, but lacked details about study design (cross-sectional vs. longitudinal) and gender.
In contrast, our study reviewed 56 studies up to February 10, 2024 encompassing 17,918 participants, while considering both study design and gender differences. The differing focus, methodologies, and outcomes between these two systematic reviews provide novel insights for researchers into the complex relationship between rumination and PTG. Despite the growing number of studies investigating this link, results remain inconsistent, raising critical questions about the factors contributing to these disparities. The primary aim of this paper is to explore the association between rumination and PTG, focusing on the differential impacts, study categories, and potential moderators that shape this relationship.
Materials and Methods
Information sources
Regarding the guidelines of databases, we searched Scopus, PubMed, PsycINFO, ScienceDirect, Web of Sciences, ProQuest, and Google Scholar from January 1, 1996 to February 10, 2024. This time range was chosen because the introductory paper on the posttraumatic growth inventory (PTGI) by Tedeschi and Calhoun [7] was first published in 1996. The database search was conducted between February 10 and 20, 2024.
Search terms
We utilized the MeSH database and related strategies to identify essential synonyms for our keywords. These layers were then combined using the “AND” and “OR” Boolean operators. The search terms included: “PTG” OR “post-traumatic growth” OR “posttraumatic Growth” OR “psychological post-traumatic growth” OR “psychological posttraumatic growth” OR “growth, posttraumatic” OR “post-traumatic growth, psychological” OR “psychological growth, post-traumatic” AND “rumination” OR “deliberate rumination” OR “DR” OR “intrusive rumination” OR “IR”. This comprehensive strategy ensured the inclusion of all relevant studies.
Eligible studies for inclusion
It is important to note that the inclusion and exclusion criteria were established prior to study selection to ensure that the selected studies were of high quality and were relevant to the research question. The criteria included factors such as: 1) Published in English language; 2) Design empirically, based on quantitative statistics and peer-reviewed original research; 3) Sufficient sample size of at least 50 participants; 4) Reporting the family of correlation coefficient (r) of DR, IR, and PTG; 5) Employed a quantitative measure of both PTG and rumination, necessary data such as Cohen’s coefficient, correlation, sample size or standard error or variance have been reported.
Studies that did not meet these criteria were excluded from the review to maintain the rigor and validity of the analysis. Additionally, the authors focused on studies that utilized the event related rumination inventory (ERRI) or a related questionnaire to ensure consistency in the measurement of rumination and PTG. The selection process for the systematic review involved two reviewers independently screening studies based on the inclusion and exclusion criteria and extracting relevant data using standardized forms. Any disagreements or discrepancies between the two reviewers during the selection or data extraction process were resolved through discussion and, if necessary, consultation with a third reviewer to reach a consensus. This approach ensured the reliability and accuracy of the study selection and data extraction process.
Study selection
The present study followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines [43] and used data extraction methods based on Lipsey and Wilson [44]. The following information was extracted from each study: a) Authors and year of publication; b) Study design (cross-sectional or longitudinal); c) Sample size; d) Percentage of female participants; e) Mean age of participants; f) Mean±SD of rumination and PTG; and g) Type of injury experienced (e.g. cancer, earthquake, traumatic experience).
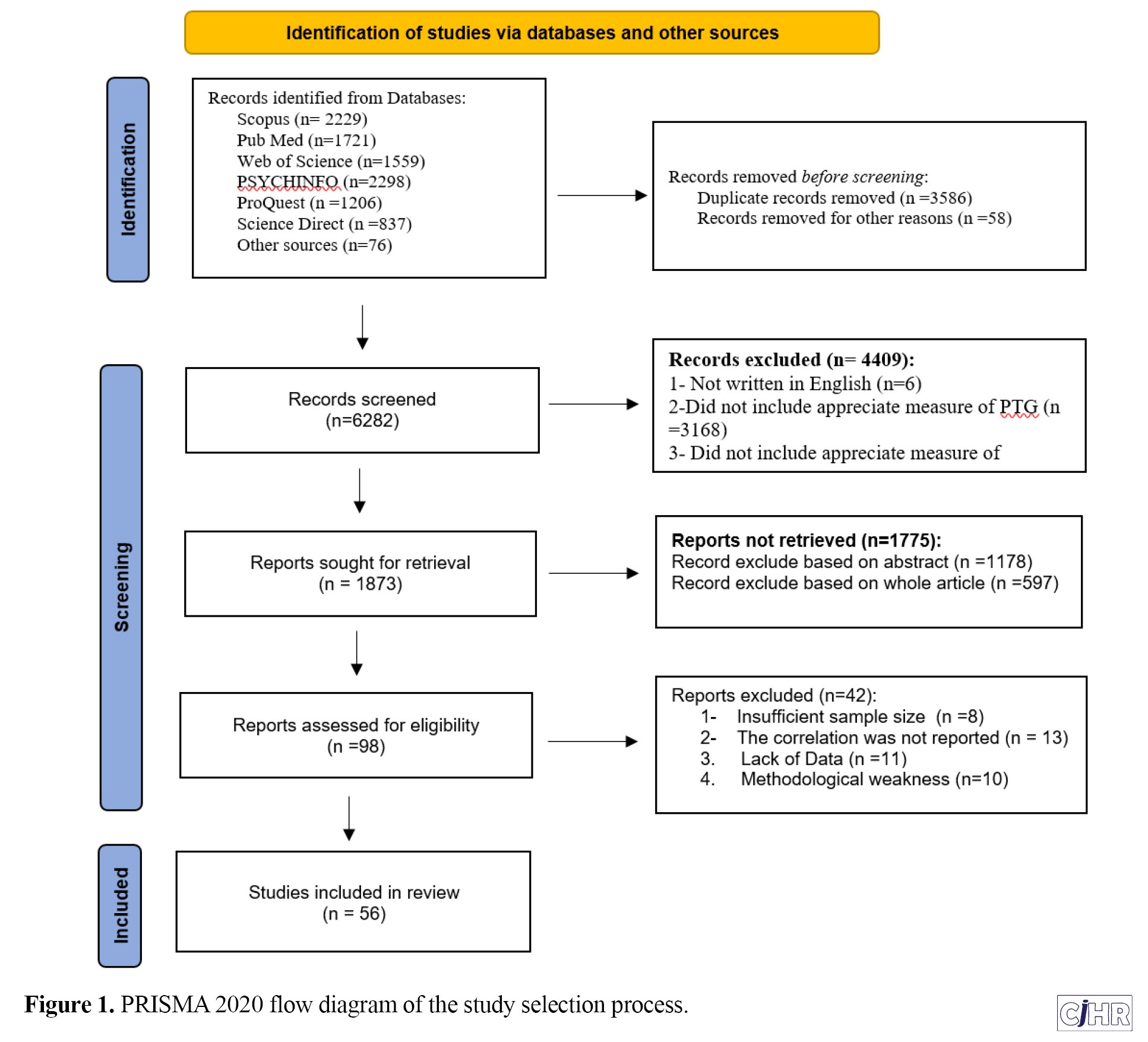
Out of the records screened, 56 studies met the inclusion criteria, with 49 studies being cross-sectional and 7 studies being longitudinal. The samples were composed of individuals who experienced a variety of traumas such as miscarriage, autism, natural disasters, terrorist attacks, amputation, cancer, and interpersonal violence, among others. The participants included parents of children with autism, aid workers, storm survivors, firefighters, natural disaster survivors, terror attack survivors, earthquake survivors, traumatic experience survivors, hemodialysis patients, COVID-19 pandemic survivors, and front line nurses. Figure 1 provides an overview of the screening process, including the reasons for exclusions at each stage.
Methodological quality assessment
To thoroughly and confidently evaluate the methodological quality and risk of bias of the included studies, we utilized two criteria. Firstly, we employed the risk of bias utilized for surveys tool (ROBUST) in this review. This measure was designed to be flexible and accessible, contributing to the standardization of risk-of-bias evaluations and aiding in the interpretation of meta-analytic findings. The items in the tool were adapted to match the exact nature of the research question, and the final score in eight questions was calculated by adding up the numbers across items. A score of 8 points indicates the highest level of confidence in the results (low risk of bias), while 0 indicates the lowest level (high risk of bias). Additionally, to determine the quality and potential for bias in reporting, two reviewers independently assessed the quality of research using the quality of survey studies in psychology tool [45].
Two criteria were used to assess the methodological quality and risk of bias of the included studies.
Second, the standard quality assessment criteria for evaluating primary research papers from a variety of fields [46] with 14 criteria were used to assess the quality of eligible studies. For example, criteria included evaluating whether the study design was evident and appropriate, whether the outcome and exposure measures were well defined and robust against measurement, misclassification bias, and whether the analytic methods were described/justified and appropriate. The overall score for this assessment was 22, after bypassing the three criteria of interventional studies, which were scored as not applicable for correlational studies (items number 5, 6, 7). After calculating the total score, papers that scored lower than the cutoff point of 0.70 were excluded from the meta-analysis by consensus of the authors. The quality of the studies was classified as low risk of bias (a score of 18 or higher) and moderate risk of bias (a score between 16 and 17). Both reviewers assigned the same overall score to the studies.
Data extraction and coding of studies
The data extraction process followed the methodology outlined in Lipsey and Wilson [44]. After ensuring that the inclusion criteria were met, the first author coded the full-text of each study according to the following variables: a) Authors and year of publication; b) Study design (i.e. cross-sectional or longitudinal); c) Sample size; d) Gender (i.e. percentage of females); e) Mean age (in years); f) Mean score of PTG; g) Mean score of rumination; h) Name of trauma; and i) Risk of bias.
Statistical analysis
To calculate the pooled correlation effect measure, we utilized Fisher’s method to transform correlations into Z-scores, which were then pooled under a random-effects model. The random-effects model, an updated version of the DerSimonian and Laird method [47], assumes that different studies estimate different but related effects. All studies included in our analysis had separate samples. We utilized the random-effects model based on the results of the Funnel plot and asymmetry test. Additionally, we investigated heterogeneity using the I-squared statistic, which ranges from 0 to 100% with values of 0 indicating no heterogeneity, 25% indicating low heterogeneity, 50% indicating moderate heterogeneity, and 75% indicating high heterogeneity. We also conducted a meta-regression to examine potential explanations for study variation by adding covariates as predictors of the pooled effect size.
We used the funnel plots and Egger’s test, which examines the likelihood of asymmetry in the final result by testing the Y-intercept=0 from a linear regression of normalized effect estimate (estimate divided by its standard error) against precision (reciprocal of the standard error of the estimate). Additionally, we stratified the data based on covariates to calculate the pooled measure of the association between rumination and PTG by various factors, whenever possible.
We used comprehensive meta-analysis software (CMA) version 3 [48] for all statistical analyses.
Results
Description of relevant studies
The search strategy identified 9926 studies, and the PRISMA flow diagram is presented in Figure 1. outlining the study selection process to ensure the reliability and validity of the study results. Following the removal of duplicate research, 6,282 papers were screened based on their titles, abstracts, and including appreciate measure of PTG or rumination. Deduplication, including the removal of identical records retrieved from multiple databases and identifying multiple articles published from the same dataset, was performed manually by exporting records into an EXCEL file and sorting them alphabetically by title and first author, as well as by date. Out of the 4409 records, those lacking measures for appreciating PTG or rumination were excluded. In this phase, the study focused on studies that utilized the ERERI [21] or a related questionnaire to ensure consistency in the measurement of rumination and PTG. In addition, out of the 1775 records, exclusions were made based on the abstract or the entire article. Of these, 98 studies were identified as potentially eligible for inclusion in the analysis and retrieved for full-text review. 42 papers were excluded due to incomplete data, the use of a different questionnaire, or failure to report the correlation value in the article. Ultimately, we included 56 papers (representing 100 effect sizes) that met our eligibility criteria.
Characteristics of the finally included studies
Table 1 summarizes the key characteristics of the studies included in the analysis.
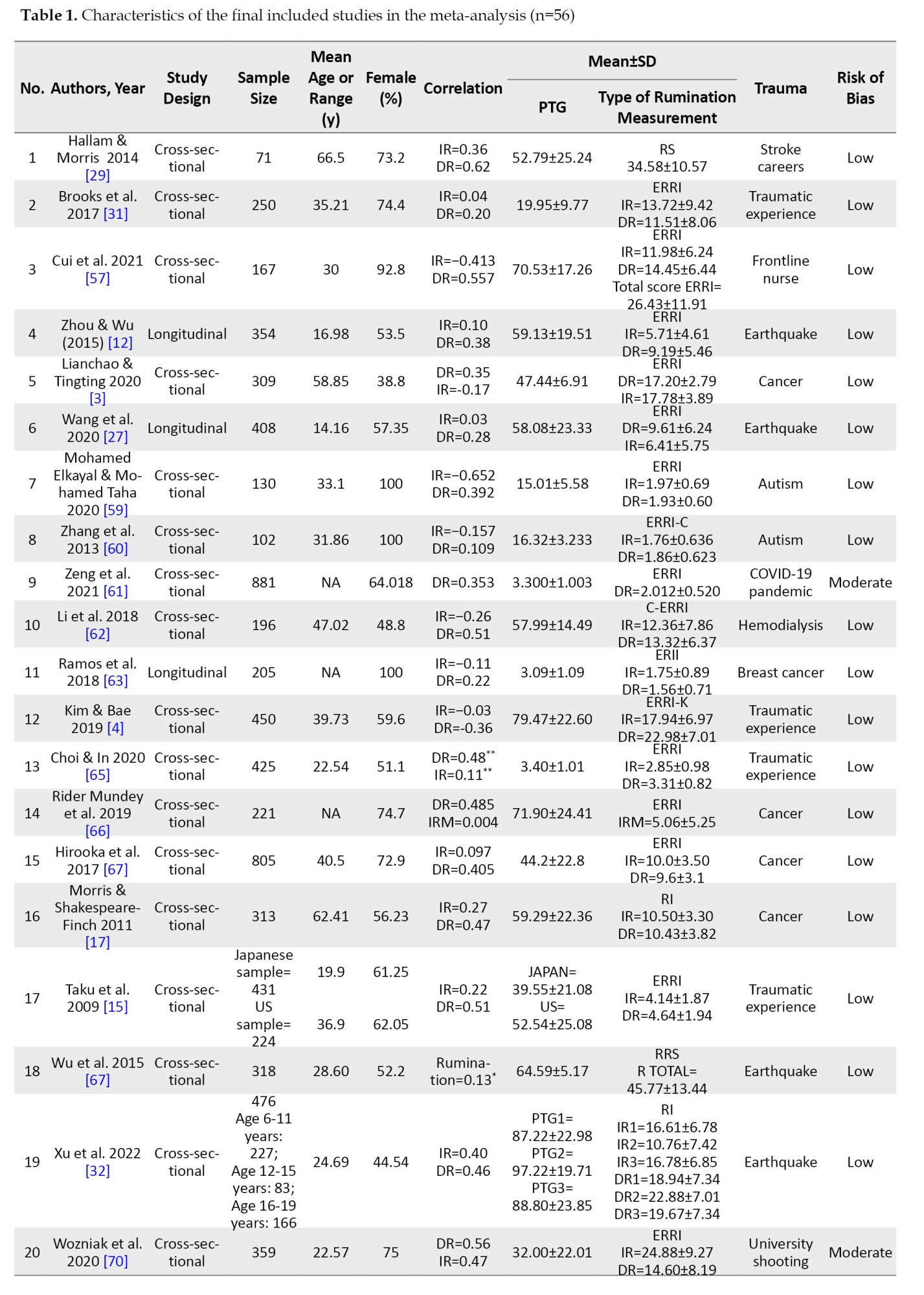
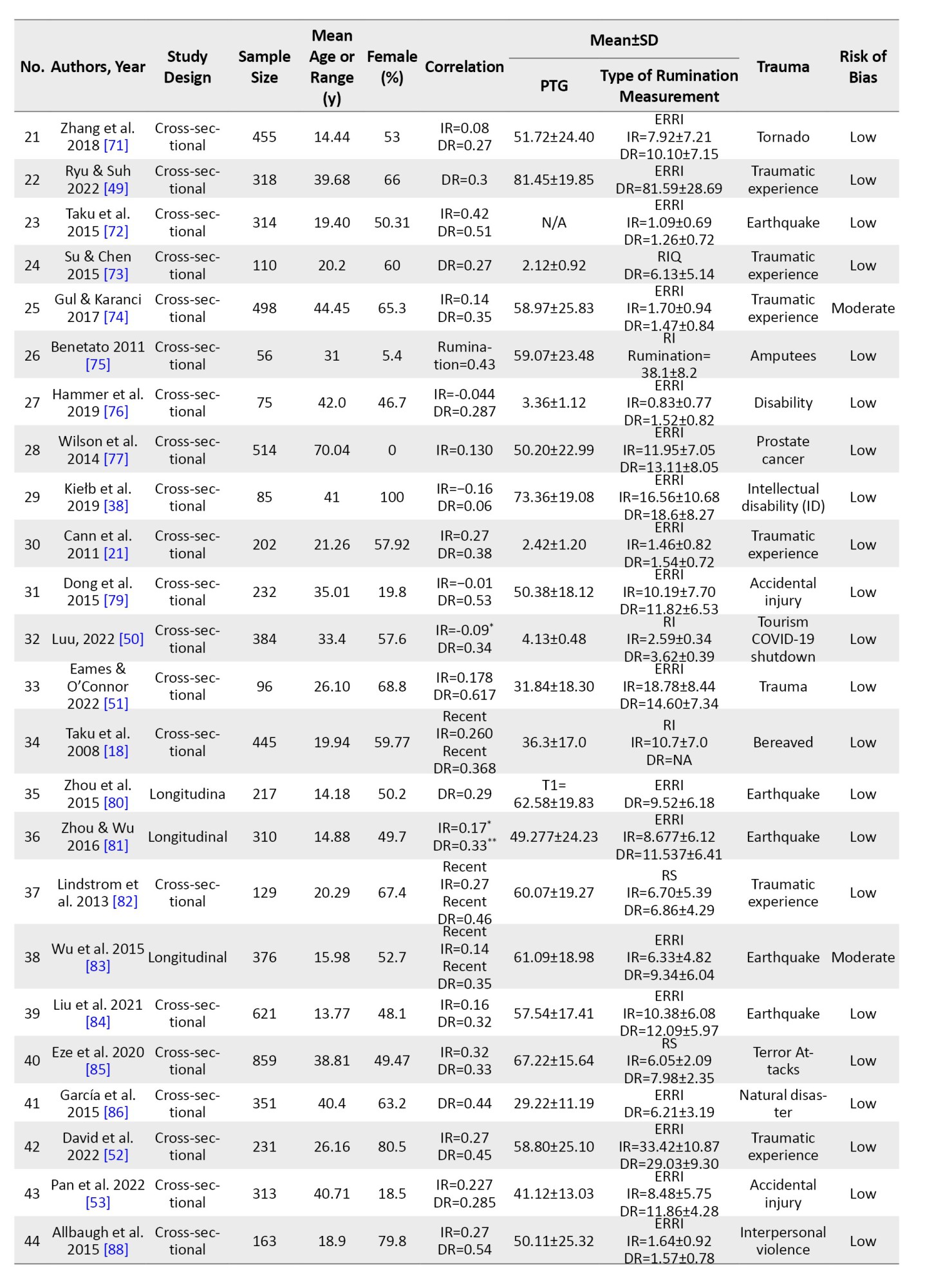
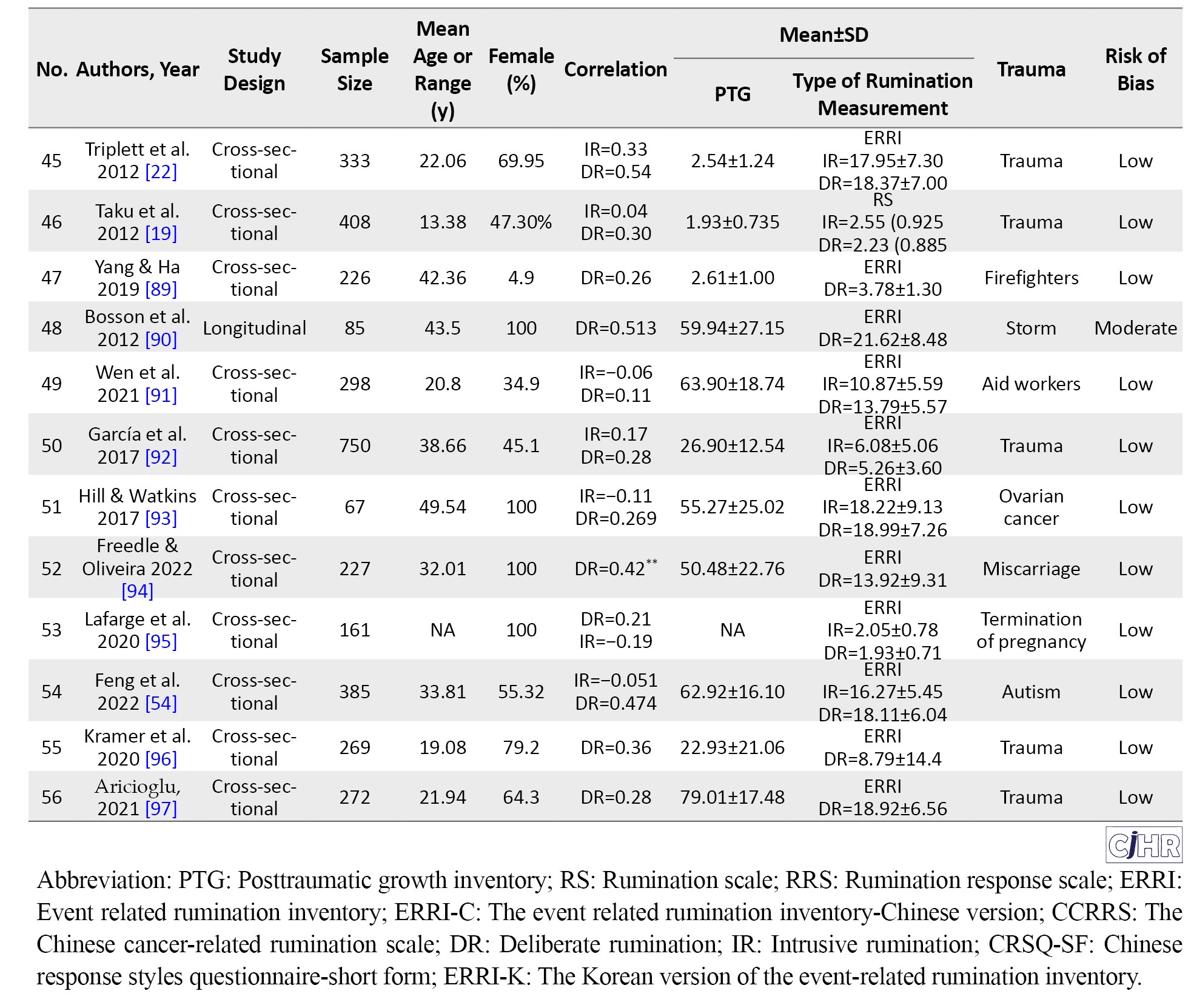
The studies were classified as either cross-sectional (n=49) or longitudinal (n=7) and were published between 2008 Taku et al. [18] and July 2023 [32, 49-54]. The total number of participants across all studies was 17,918, with 7,967 males and 9,951 females. The age range of the participants was 13.77 to 70.04 years, with a mean age of approximately 32.66.
Quality assessment summary
As presented in additional Table 1, out of 56 papers included in the analysis, 5 articles had a moderate risk of bias due to certain limitations such as small sample size, inadequate description of the methods, or incomplete reporting of the results. The rest of the studies were judged to have high quality and low risk of bias by the authors. The mean study quality rating of the included studies was 19.38±1.69 (range 0 to 22). It is noteworthy that, as explained in detail in Section 1.5, the RoB tool was used for quality assessment. All studies that met the inclusion criteria demonstrated an inter-rater agreement of <0.70, which was set as the cutoff point, between two independent reviewers.
Synthesis of results: The main analysis
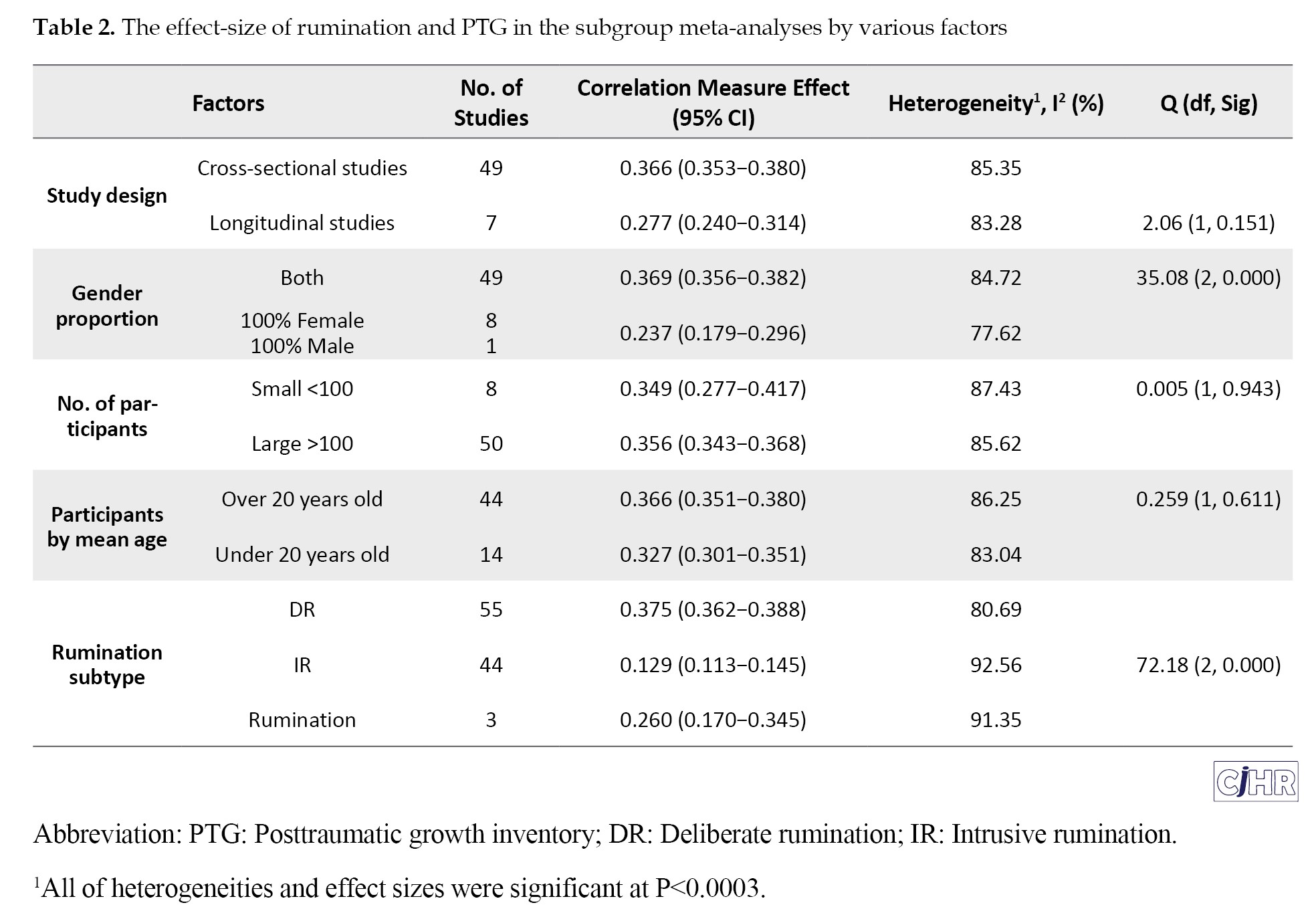
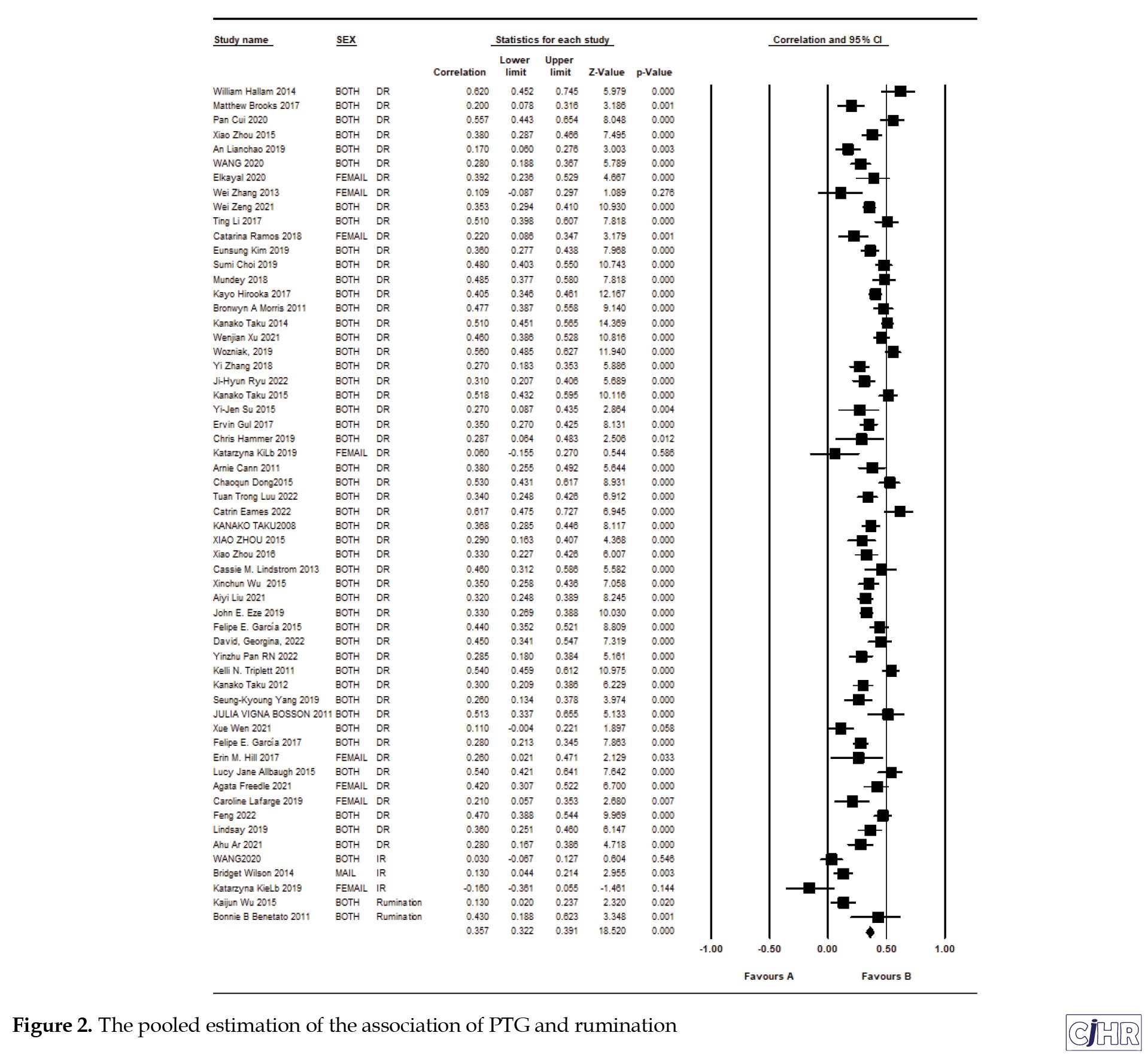
As shown in Table 2 and Figure 2 (forest plot) the point estimate of the pooled correlation meta-analysis indicated a significant positive association between rumination and PTG across different categories of studies, including cross-sectional studies (r=0.358; 95%CI, 0.323%, 0.393%; P=0.001) and longitudinal studies (r=0.342; 95%CI, 0.236%, 0.440%; P=0.001).
 Moreover, the positive correlation was significant for both male and female participants, with a slightly stronger effect size in female participants (r=0.364; 95%CI, 0.324%, 0.404%; P=0.001) compared to male participants (r=0.340; 95%CI, 0.291%, 0.389%; P=0.001). The age of participants did not significantly moderate the relationship between rumination and PTG (r=0.342; 95%CI, 0.295%, 0.389%; P=0.001 for age <40 years; r=0.364; 95%CI, 0.318%, 0.410%; P=0.001 for age ≥40 years).
Moreover, the positive correlation was significant for both male and female participants, with a slightly stronger effect size in female participants (r=0.364; 95%CI, 0.324%, 0.404%; P=0.001) compared to male participants (r=0.340; 95%CI, 0.291%, 0.389%; P=0.001). The age of participants did not significantly moderate the relationship between rumination and PTG (r=0.342; 95%CI, 0.295%, 0.389%; P=0.001 for age <40 years; r=0.364; 95%CI, 0.318%, 0.410%; P=0.001 for age ≥40 years).
Furthermore, the association between rumination and PTG remained significant when adjusting for the type of trauma, with a slightly stronger effect size in studies that focused on natural disasters (r=0.375; 95%CI, 0.321%, 0.429%; P=0.001) compared to studies that focused on other types of trauma (r=0.341; 95%CI, 0.302%, 0.380%; P=0.001). The analysis also revealed that the relationship between rumination and PTG was not significantly affected by the risk of bias in the included studies (low risk of bias: r=0.364; 95%CI, 0.327%, 0.401%; P=0.001; moderate risk of bias: r=0.354; 95%CI, 0.260%, 0.439%; P=0.001). Finally, the meta-regression analysis showed that none of the covariates (i.e. sample size, year of publication, mean age, gender, type of trauma, risk of bias) significantly moderated the relationship between rumination and PTG.
Longitudinal versus cross-sectional study design
No significant difference between the two groups in the effect size (Q=2.06, P=0.151). Based on the study design, the point estimate of the effect size (ES) of the relationship between rumination and PTG was calculated. The ES in cross-sectional studies (n=49; participants=15963; mean age=33.05±7.51 years; female=8777; I2=85.35%) was 0.366 (CI, 0.353-0.380). The ES in longitudinal studies (n=7; participants=1955; mean age= 19.94±3.75 years; female=1174; I2=83.28%) was 0.277 (CI, 0.240-0.314). Despite the significant effect size and favorable heterogeneity in both cross-sectional and longitudinal study groups, there was no significant difference between the two groups in the effect size (Q=2.06, P=0.151). To better understand the temporal dynamics of rumination and PTG, future research should prioritize conducting more longitudinal studies. These studies can offer valuable insights into how these processes develop and change over time.
Gender differences
Regarding the gender distribution, the included studies were categorized based on the proportion of males and females, with 1 study consisting entirely of male participants and 8 studies consisting entirely of female participants, while the remaining 47 studies included both genders. Therefore, the focus on these two genders was driven by the availability and distribution of participants across the studies included in the analysis. The effect size was calculated for each group and compared. As shown in Table 2, the effect size for studies including both genders was 0.369 (CI, 0.356-0.382; I2=84.72%), while for studies including only females, it was 0.237 (CI, 0.179-0.294; I2=77.62%). Although both groups showed significant effect sizes with good heterogeneity, there was a significant difference between the two (Q=35.08, P=0.000), with studies including both genders showing a higher effect size than studies including only females.
Sample size and diversity variations
In the subgroup analysis based on age, studies were classified into three groups: Studies conducted on adolescents (n=13), studies conducted on adults (n=41), and studies conducted on mixed age groups (n=4). The results show that the effect size in adolescents (0.307; CI, 0.260-0.354; I2=80.64%) was lower than in adults (0.370; CI, 0.356-0.384; I2=85.09%). Additionally, the effect size in mixed age groups (0.417; CI, 0.351-0.483; I2=91.75%) was higher than in the other two groups.
There was a significant difference between the three groups (Q=17.36, P=0.000).
Reviewing the participants of the included studies reveals diverse cultural populations and countries, such as Japan [15, 18], Turkey [74], the United States [66, 69], the Caucasus [21], China [3, 12], Korea [49], and Egypt [59], among others. Additionally, some studies, such as Taku and colleagues [15], investigated two different populations from Japan and the United States. Similarly, Cann and colleagues [21] included diverse participants, such as Caucasian, African-American, and Asian-American individuals. Moreover, as shown in Table 1, the included studies encompass a variety of trauma types, including cancer [3, 66], earthquakes [12, 27], autism [54, 59], accidental injuries [53, 79], and disabilities [76], among others. These factors enhance the generalizability of the findings and provide a more nuanced understanding of how rumination influences PTG across diverse contexts and populations.
Age differences
The included studies were divided into two groups based on the mean age of the subjects: 1) Over 20 years old (n=44); and 2) under 20 years old (n=14). The results indicated that effect size (ES) in the over 20 years old group (0.366; CI, 0.351-0.380; I2=86.25%) did not differ significantly (Q=0.259, P=0.611) from the under 20 years old group (0.327; CI, 0.301-0.351; I2=83.04%). This suggests that the ES may better represent the true ES among individuals over 20 years old, as it accounts for the possible heterogeneity of the included studies.
Rumination subtype
In the included studies, three subtypes of rumination with 100 effect sizes were used to measure rumination, including DR (n=53), IR (n=44), and general rumination (n=3). Results indicated that the effect size in all three subtypes of studies based on DR (0.375; CI, 0.362 -0.388; I2=80.68%), IR (0.129; CI, 0.113-0.145; I2=92.56%) and general rumination (0.26; CI, 0.17-0.345; I2=91.35%) was significant with good heterogeneity. Moreover, there were significant differences between the effect sizes of the three subtypes of rumination (Q=72.18, P=0.000).
Heterogeneity, risk of publication bias and sensitivity analysis
The results of the publication bias tests indicate that the included studies are unlikely to be affected by publication bias. The funnel plot is the scatterplot used to visually assess the presence of publication bias or heterogeneity by examining the distribution of standard errors across individual studies (Figure 3).
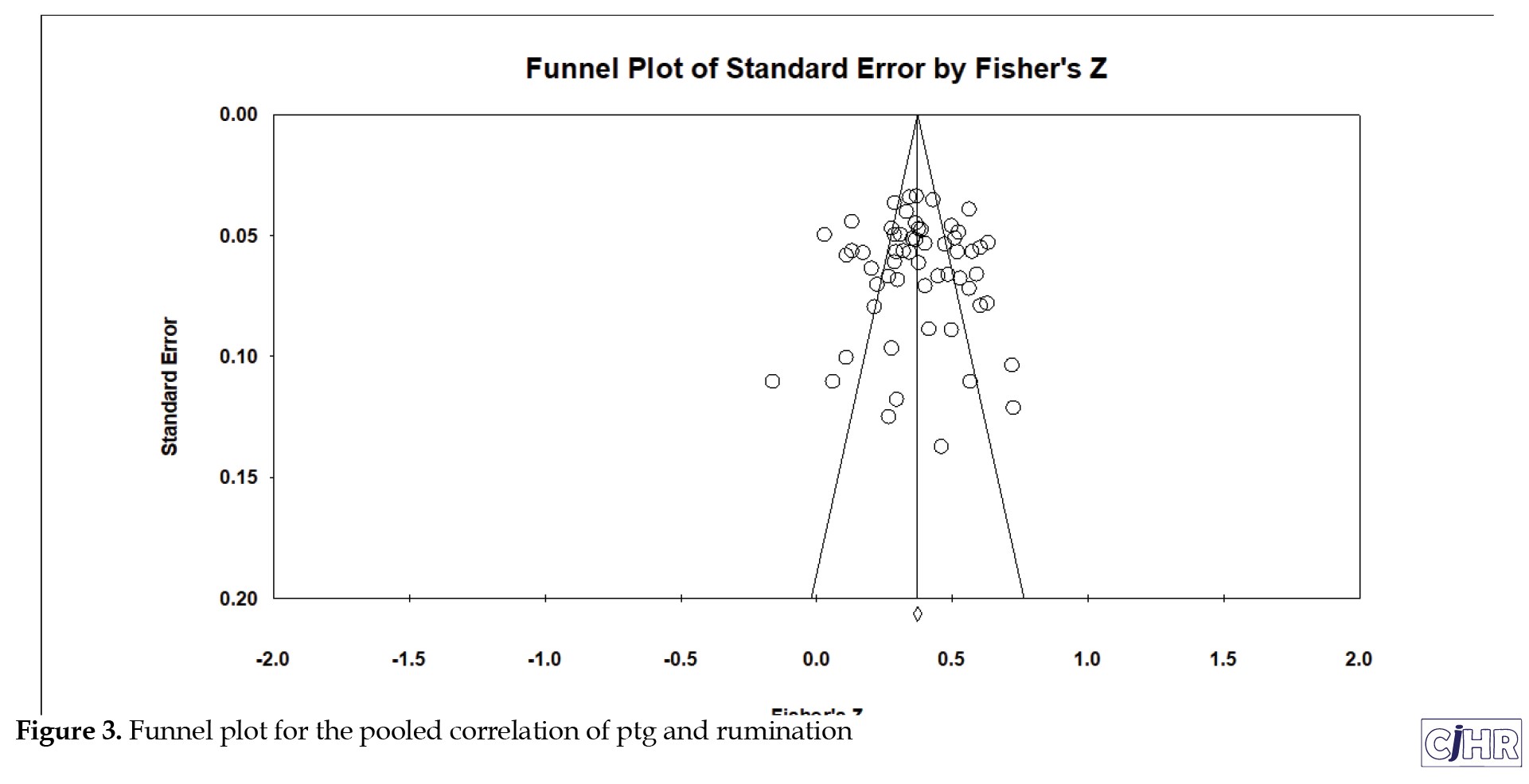 The symmetric shape of the funnel plot and the low significance value obtained from Egger’s test suggest that there is no significant asymmetry in the distribution of effect sizes across studies. The fail-safe N test also shows that a large number of non-significant studies would need to be included in order to alter the significance of the overall effect size. Finally, the Begg and Mazumdar rank correlation test also supports the unlikelihood of publication bias. Overall, these results suggest that the included studies are likely to provide a reliable estimate of the effect size.
The symmetric shape of the funnel plot and the low significance value obtained from Egger’s test suggest that there is no significant asymmetry in the distribution of effect sizes across studies. The fail-safe N test also shows that a large number of non-significant studies would need to be included in order to alter the significance of the overall effect size. Finally, the Begg and Mazumdar rank correlation test also supports the unlikelihood of publication bias. Overall, these results suggest that the included studies are likely to provide a reliable estimate of the effect size.
A sensitivity analysis was conducted to assess the robustness of the effect size in the presence of heterogeneity. The one-study removed method was used to identify any possible study that could be responsible for the heterogeneity. The forest plot is a useful graphical display of findings from the meta-analysis and in Figure 4 shows that there are no obvious outliers, indicating that no single study could significantly influence the effect size estimate.
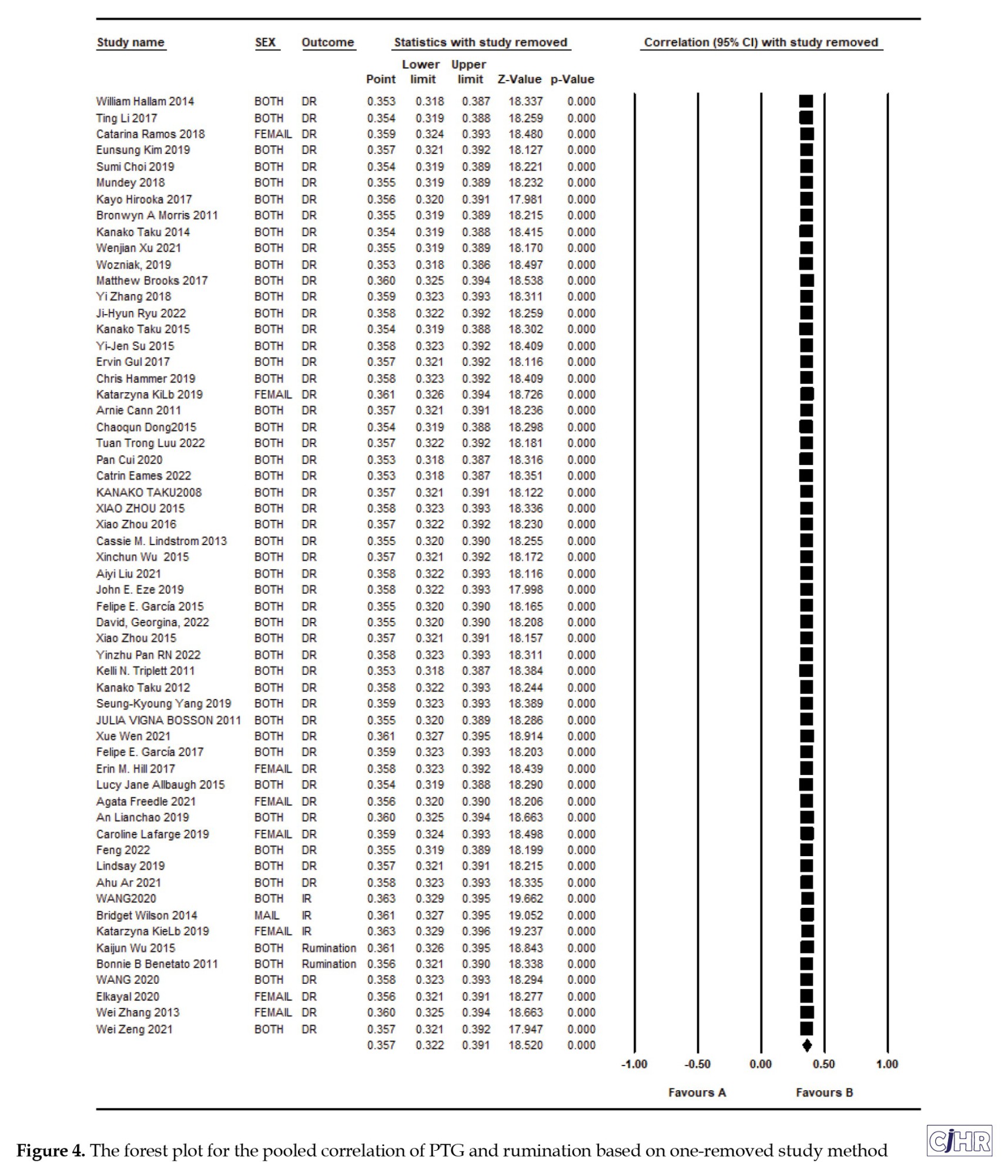 Therefore, the results of this meta-analysis are likely robust and not influenced by the inclusion of any particular study.
Therefore, the results of this meta-analysis are likely robust and not influenced by the inclusion of any particular study.
Retrospective power analysis
To ensure the reliability and validity of the current study, we conducted a power analysis using the formula proposed by Valentine et al. [98]. Based on the summary of effect size, the mean number per group, and the number of effect sizes, the power analysis yielded a value of 0.9993, indicating excellent statistical power despite the high heterogeneity of the included studies. Therefore, with a P=0.007, we can confidently conclude that the number of studies included in this meta-analysis is sufficient to establish the statistical significance and meaningfulness of the overall pooled correlation.
Discussion
This systematic review and meta-analysis aimed to investigate the relationship between rumination and posttraumatic growth (PTG). Surprisingly, we found a significant positive effect of rumination on PTG, despite the high degree of heterogeneity observed in the analysis. We conducted several subgroup analyses based on different subtypes of rumination, including DR (n=53), IR (n=44), and rumination (n=3), and found significant effect sizes with good heterogeneity in all three subtypes, with significant differences in heterogeneity between subgroups. These findings are consistent with previous research that has found DR and related constructs to be positively associated with PTG [3, 17]. DR plays an important role in facilitating positive psychological change by helping individuals move away from negative psychological reactions and toward a greater understanding of the post-traumatic world. This study supports the Shattered Assumptions theory [59] and the PTG model [20] and findings of Allen and colleagues [42], suggesting that DR can help individuals find positive meaning in traumatic experiences, leading to the development of PTG [21]. According to shattered assumptions theory, when individuals undergo an event that shatters their worldview (i.e. traumatic experience), they cease to view the world as benevolent and predictable, or perceive themselves as competent and invulnerable.
Additionally, studies have shown that DR can also lead to an increase in seeking and receiving perceived social support, which can reduce the negative effects of rumination and promote positive experiences leading to PTG [32, 69]. DR and IR can interact and jointly influence PTGT. On one hand, research suggests that IR may activate DR and also with DR mediating the relationship between IR and PTG [4]. On the other hand, Taku et al. [15] found that while both types of rumination are positively associated with PTG, their effects vary over time: Early IR is positively linked to PTG, whereas recent DR is the strongest predictor of current PTG. This finding suggests that the relationship between rumination and PTG is complex and influenced by various factors, including social support. It highlights the importance of considering these factors in future research and interventions aimed at promoting PTG.
Moreover, it is conceivable that IR serves as a signal, indicating the necessity for engaging in more deliberate and purposeful processing of traumatic events. In this context, experiencing intrusive thoughts might indeed facilitate the transition toward DR and PTG. While many individuals experience IR after traumatic events, some studies have shown a negative relationship between IR and PTG [4, 22, 37, 38, 102] and persistent IR can adversely affect PTG while increasing the likelihood of PTSD [22]. Thus, IR may have a negative relationship with PTG and could contribute to adverse outcomes, such as PTSD. The negative effects of IR may also vary based on contextual factors, such as the type of trauma experienced and individual coping styles. For instance, if the individual is stuck in ongoing IR and uses more avoidance-focused coping, it might lead to more decrease reports of PTG [102]. Additionally, Park and colleagues [102] reviewed studies showing that IR to be negatively associated with various indicators of adjustment and well-being. Specially, IR has been linked to a range of negative outcomes, including poorer psychological adjustment and reduced health-related quality of life for cancer survivors [103]. IR may act as a mechanism through which cancer continues to affect their distress by perpetuating reminders of the illness, either continuously or intermittently [102].
However, it is crucial to acknowledge that the link between IR and PTG is intricate and can be influenced by factors like the severity and nature of the trauma, individual coping strategies, and available social support. Additionally, Allen and colleagues’ study [42] found no significant overall effect in the association between IR and PTG. Consequently, further research is warranted to gain a more comprehensive understanding of the nuanced relationship between IR and PTG.
Different emotional regulation strategies can mediate the relationship between rumination and PTG, providing a broader context for understanding the underlying mechanisms. For example, cognitive reappraisal, as a regulatory strategy, mediates the link between DR and PTG. Higher levels of Dr may promote positive emotional focus and constructive coping, fostering cognitive reappraisal strategies that enhance perspective-taking, positivity, and emotional well-being [104].
In addition, our findings suggest that the relationship between rumination and PTG may not be affected by the timing of the trauma, as there was no significant difference in effect size between cross-sectional and longitudinal study designs. This indicates that rumination may be a useful strategy for promoting PTG both in the short-term and long-term. It is also possible that the degree to which individuals engage in thinking about their emotions and perspectives on their crisis plays a role in the PTG process, regardless of the timing of the study. These results are consistent with previous research that has found a positive relationship between rumination and PTG in both cross-sectional and longitudinal studies [21, 27]. The relationship between rumination and PTG over time is a compelling subject for study. Some research [26] suggests that the predictive effect of DR on PTG fluctuates over time. For instance, Zhou and colleagues [26] found that while DR significantly predicted PTG several years after trauma, this predictive effect was absent in earlier years. This highlights the unstable relationship between DR and PTG at different time points following trauma. These findings underscore the need for more longitudinal research to clarify the dynamic relationship between rumination and PTG over time.
Interestingly, we found a significant difference in the effect sizes between studies based on males and females. Specifically, studies including both sexes had a higher effect size than studies with only female participants. This finding is consistent with previous research suggesting that gender is associated with PTG, with females tending to exhibit higher levels of PTG than males [36, 56, 78, 87]. A meta-analysis by Vishnevsky et al. [55] also revealed a small to moderate gender difference, with women reporting more PTG than men. The findings of Hussain and Bhushan [25] also indicated that females reported significantly higher scores compared with males on traumatic experiences, posttraumatic stress, and PTG.
On the other hand, some studies, such as the meta-analysis by Johnson and Whisman [100], have indicated that females tend to ruminate more than males. Similarly, Rood and colleagues [101] reported in a meta-analysis of child and adolescent literature that girls are more likely to ruminate than boys. Specifically, certain studies [15, 99] have found that both IR and DR are higher among females compared to males. These findings may help in better analyzing the gender differences that arise in the relationship between rumination and PTG.
The higher levels of rumination and PTG reported among females could provide insights into why females exhibit a significantly stronger relationship between rumination and PTG. A possible explanation, as suggested by PTG theorists [11], is that growth requires negative life events and ruminative activity. Since females tend to engage in both IR and DR more than males [15, 99], they may also report higher levels of PTG. Females may have a greater tendency to reflect and ponder over adverse events, which may lead them to discover new possibilities in life, find meaning in the events, re-evaluate their priorities, and experience improvements in relationships and spiritual growth—factors that contribute to PTG [99]. These findings suggest that gender may play an important role in the relationship between rumination and PTG.
Conclusion
In conclusion, our meta-analysis revealed a significant effect of rumination on PTG, contrary to our initial expectation of only finding small pockets of data. Emotion regulation strategies, including rumination, are considered response-focused coping and may be particularly useful in coping with traumatic events that are rooted in the past. However, it is worth noting that previous research has suggested that response-focused emotion regulation strategies may be unhelpful or even harmful in coping with the threatening information brought about by trauma. Our study provides important insights into the potential role of rumination in promoting PTG, and highlights the importance of further research to fully understand the complex relationship between rumination and PTG. However, the significant heterogeneity in the main analyses indicates the need for caution when interpreting the results. Future studies should explore the actual effect that specific aspects of emotion regulation strategies, such as rumination, have on PTG and investigate the influence of gender on rumination and PTG It is important to note that heterogeneity is a common issue in meta analyses of psychological constructs, as these often vary widely across studies.
Limitations
The current meta-analysis has several limitations that should be considered when interpreting the results. The number of studies included in the analysis was adequate but relatively limited, which may have constrained the statistical power of the study to detect treatment efficacy. Additionally, the sample sizes in some studies were relatively small, further limiting the robustness and generalizability of the conclusions. Furthermore, the quality of the trials was suboptimal, with the majority of the included studies classified as high-risk according to the Cochrane RoB assessment.
Moreover, potential biases may have influenced the findings and to address these biases, it is important to interpret the findings with caution. For example, the inter-rater agreement could not be computed due to the database being built over several years, involving multiple raters in the screening and selection process. This variability in the screening process may have introduced inconsistencies in study inclusion. Additionally, the possibility of reporting bias cannot be entirely ruled out, as studies with significant results are more likely to be published, potentially skewing the overall findings. While the sensitivity and meta-regression analyses indicate that these biases did not significantly influence the overall results, the presence of moderate bias in a subset of studies and variability in the screening process highlight the need for standardized methods in future research. Furthermore, the potential impact of small sample sizes on the robustness of conclusions underscores the importance of including larger, well-designed studies in future meta-analyses to strengthen the reliability of the findings.
Another key limitation of this meta-analysis is the high degree of heterogeneity observed across the included studies. This variability likely reflects differences in study design, sample characteristics, and the measurement tools used for rumination and PTG. While we conducted subgroup and moderator analyses to explore potential sources of heterogeneity, as well as sensitivity analyses to ensure the robustness of the findings, the diverse methodologies and populations remain a challenge to the generalizability of the results. Future research should prioritize the use of standardized measurement tools and study designs to reduce variability and improve comparability. Furthermore, longitudinal studies are particularly needed to better provide deeper insights into how these processes evolve over time and contribute to PTG.
Although different populations and trauma types were mentioned in the included papers, the findings may not be generalizable to all populations, as the studies do not cover all demographics or trauma types. For example, despite a considerable number of studies on Chinese populations, there are few studies focusing on African populations. Similarly, while there is substantial research on medical traumas, there are limited studies addressing violence- and abuse-related trauma. This focus on specific demographics and trauma types may limit the applicability of the results to broader contexts. Therefore, future research should aim to expand studies to include other populations and trauma types to enhance generalizability.
These limitations suggest that future research in this area should aim to address these issues and further explore the relationship between rumination and PTG.
Future directions and clinical implications
Our findings hold significant practical implications. It is crucial for therapists to recognize that both IR and DR are common responses to traumatic events. Therefore, implementing training programs that encourage individuals to engage in DR is essential. Notably, designing targeted intervention programs for females to promote DR over IR in the aftermath of trauma may prove particularly beneficial.
These findings have several implications for future research in this field. First, there has been a lack of comprehensive exploration regarding whether and how rumination contributes to positive changes following traumatic events. Most of the existing correlational research focuses on discussing the relationship between rumination and negative posttraumatic outcomes such as PTSD. Thus, future studies are still needed to determine the actual effect that specific aspects of emotion regulation strategies (e.g. rumination) have on PTG.
Future studies should further investigate gender differences in the association between rumination and PTG to better understand the psychological, social, and cultural factors contributing to these variations. Examining how gender influences both intrusive and deliberate rumination, as well as their distinct contributions to PTG, could yield valuable insights. Longitudinal research is particularly needed to determine whether these gender differences persist over time and how factors such as coping strategies, cultural norms, and social support shape the rumination-PTG relationship across genders. Such studies could guide the development of tailored interventions to effectively support trauma survivors. Additionally, future studies should aim to address the limitations of this meta-analysis by increasing the number of studies, improving the quality of trials, and exploring factors that contribute to heterogeneity. Moreover, inter-rater agreement should be considered and evaluated to ensure the reliability of the database.
Ethical Considerations
Compliance with ethical guidelines
This article is review with no human or animal sample. There were no ethical considerations to be considered in this work.
Funding
This research did not receive any specific funding from granting agencies nor commercial or not-for-profit sectors.
Authors' contributions
Methodology: Jafar Hasani; Investigation, data collection, and data curation: Mehrnesa Shahabi; Data analysis: Mehrnesa Shahabi and Jafar Hasani; Writing the original draft: Mehrnesa Shahabi and Majid Asadpour; Review and editing: Majid Asadpour.
Conflict of interest
The authors declared no conflict of interest.
References
understanding the factors contributing to post-traumatic growth (PTG) is essential for creating effective interventions and support systems for trauma survivors. Rumination, involving repetitive and intrusive thoughts about past events, has been linked to both increased distress and growth following trauma. However, the relationship between rumination and PTG remains complex. This study addresses this gap through a systematic review and meta-analysis, examining the association between rumination and PTG across diverse study designs and populations.
Traumatic events are unfortunately prevalent worldwide [1] and people respond differently to them. The available data suggests that at least a minority of people who have experienced trauma, e.g. earthquake, cancer, and traumatic experience reported meaningful levels of personal growth [2-4]. Such that some individuals experience personal growth and positive changes after experiencing trauma [5]. PTG refers to positive changes such as feeling strength and wisdom, increasing value to friends and family, and finding a fresh appreciation for each new day, that result from struggling to cope with a traumatic event [6, 7].
Moreover, it is important to mention that the positive changes or growth are not results of the event itself, but rather results of the struggle to cope with it. In this context, various strategies exist to cope with trauma, yet rumination may significantly influence the process of developing PTG [8]. Rumination is a cognitive process that repetitively and passively focuses on the meaning, causes, and consequences of negative emotions [9, 10].
The PTG model [11] suggests that people may review their personal belief systems and think regularly about traumatic events, which may include two forms of rumination: Intrusive and deliberate. Due to Zhou and colleagues [12] intrusive and deliberate ruminations are two different functional forms that may play different roles in posttraumatic psychology. Intrusive rumination (IR) refers to the negative focus on trauma-related cues or negative mood and has a complex relationship with PTG. While some studies found that IR provides a basis for further cognitive processing of PTG [13-15], others found no significant correlation between IR and PTG [17-19]. Deliberate rumination (DR), on the other hand, may facilitate individuals to reconstruct their understanding of the post-traumatic world and realize PTG [20]. Results have suggested that DR is an important predictive factor for PTG [21-28].
Calhoun and colleagues [29] pointed out that DR refers to one’s deliberate reexamining and contemplation of the traumatic event and traumatic-related DR can help individuals think positively about the meaning associated with trauma, facilitate themselves to reconstruct their understanding about the post-traumatic world and facilitate the realization of PTG [20]. Therefore, however, the relationship between rumination and PTG is complex, with some studies showing positive relationships between DR and IR and PTG [29-38], while others show a negative relationship between IR and PTG [4, 36-38].
This statement highlights the findings of several meta-analyses related to the correlation between positive aspects of emotion regulation strategies and PTG. The studies mentioned suggest that acceptance and reappraisal are positively correlated with PTG, while acceptance coping yielded the smallest effect size. Additionally, the meta-analysis by Prati and Pietrantoni [39] found that religious coping and positive reappraisal coping produced the largest effect sizes. Furthermore, the meta-analysis by Shiyko et al. [40] showed that change in spirituality had a medium to large effect size on PTG. A systematic review and meta-analysis by Gower et al. [41] revealed that downward comparison bias, positive attention bias, and growth beliefs had stronger correlations with perceived PTG than did defensiveness, memory bias, and social desirability bias. However, while meta-analytic data from traumatized individuals suggest that emotion regulation problems are associated with post-traumatic stress disorder (PTSD); this has yet to be studied in the context of PTG.
Allen and colleagues [42] conducted a meta-analysis exploring the profound effects of trauma on core beliefs and the ensuing process of PTG via rumination. Their study investigates the links between event-related IR and DR and PTG while considering moderating factors like age, time elapsed since trauma, and the nature of the traumatic experience. Their analysis revealed a significant association between retrospective DR soon after trauma and PTG. However, IR displayed non-significant and variable associations. These findings emphasize the importance of promoting deliberate cognitive processing among trauma survivors to encourage PTG, highlighting the necessity for longitudinal research into the temporal role of event-related rumination in PTG development. They identified 46 studies up to May 1, 2021, involving 12,048 participants. The study analyzed 46 studies involving 12,048 participants up to May 1, 2021, but lacked details about study design (cross-sectional vs. longitudinal) and gender.
In contrast, our study reviewed 56 studies up to February 10, 2024 encompassing 17,918 participants, while considering both study design and gender differences. The differing focus, methodologies, and outcomes between these two systematic reviews provide novel insights for researchers into the complex relationship between rumination and PTG. Despite the growing number of studies investigating this link, results remain inconsistent, raising critical questions about the factors contributing to these disparities. The primary aim of this paper is to explore the association between rumination and PTG, focusing on the differential impacts, study categories, and potential moderators that shape this relationship.
Materials and Methods
Information sources
Regarding the guidelines of databases, we searched Scopus, PubMed, PsycINFO, ScienceDirect, Web of Sciences, ProQuest, and Google Scholar from January 1, 1996 to February 10, 2024. This time range was chosen because the introductory paper on the posttraumatic growth inventory (PTGI) by Tedeschi and Calhoun [7] was first published in 1996. The database search was conducted between February 10 and 20, 2024.
Search terms
We utilized the MeSH database and related strategies to identify essential synonyms for our keywords. These layers were then combined using the “AND” and “OR” Boolean operators. The search terms included: “PTG” OR “post-traumatic growth” OR “posttraumatic Growth” OR “psychological post-traumatic growth” OR “psychological posttraumatic growth” OR “growth, posttraumatic” OR “post-traumatic growth, psychological” OR “psychological growth, post-traumatic” AND “rumination” OR “deliberate rumination” OR “DR” OR “intrusive rumination” OR “IR”. This comprehensive strategy ensured the inclusion of all relevant studies.
Eligible studies for inclusion
It is important to note that the inclusion and exclusion criteria were established prior to study selection to ensure that the selected studies were of high quality and were relevant to the research question. The criteria included factors such as: 1) Published in English language; 2) Design empirically, based on quantitative statistics and peer-reviewed original research; 3) Sufficient sample size of at least 50 participants; 4) Reporting the family of correlation coefficient (r) of DR, IR, and PTG; 5) Employed a quantitative measure of both PTG and rumination, necessary data such as Cohen’s coefficient, correlation, sample size or standard error or variance have been reported.
Studies that did not meet these criteria were excluded from the review to maintain the rigor and validity of the analysis. Additionally, the authors focused on studies that utilized the event related rumination inventory (ERRI) or a related questionnaire to ensure consistency in the measurement of rumination and PTG. The selection process for the systematic review involved two reviewers independently screening studies based on the inclusion and exclusion criteria and extracting relevant data using standardized forms. Any disagreements or discrepancies between the two reviewers during the selection or data extraction process were resolved through discussion and, if necessary, consultation with a third reviewer to reach a consensus. This approach ensured the reliability and accuracy of the study selection and data extraction process.
Study selection
The present study followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines [43] and used data extraction methods based on Lipsey and Wilson [44]. The following information was extracted from each study: a) Authors and year of publication; b) Study design (cross-sectional or longitudinal); c) Sample size; d) Percentage of female participants; e) Mean age of participants; f) Mean±SD of rumination and PTG; and g) Type of injury experienced (e.g. cancer, earthquake, traumatic experience).
Out of the records screened, 56 studies met the inclusion criteria, with 49 studies being cross-sectional and 7 studies being longitudinal. The samples were composed of individuals who experienced a variety of traumas such as miscarriage, autism, natural disasters, terrorist attacks, amputation, cancer, and interpersonal violence, among others. The participants included parents of children with autism, aid workers, storm survivors, firefighters, natural disaster survivors, terror attack survivors, earthquake survivors, traumatic experience survivors, hemodialysis patients, COVID-19 pandemic survivors, and front line nurses. Figure 1 provides an overview of the screening process, including the reasons for exclusions at each stage.
Methodological quality assessment
To thoroughly and confidently evaluate the methodological quality and risk of bias of the included studies, we utilized two criteria. Firstly, we employed the risk of bias utilized for surveys tool (ROBUST) in this review. This measure was designed to be flexible and accessible, contributing to the standardization of risk-of-bias evaluations and aiding in the interpretation of meta-analytic findings. The items in the tool were adapted to match the exact nature of the research question, and the final score in eight questions was calculated by adding up the numbers across items. A score of 8 points indicates the highest level of confidence in the results (low risk of bias), while 0 indicates the lowest level (high risk of bias). Additionally, to determine the quality and potential for bias in reporting, two reviewers independently assessed the quality of research using the quality of survey studies in psychology tool [45].
Two criteria were used to assess the methodological quality and risk of bias of the included studies.
Second, the standard quality assessment criteria for evaluating primary research papers from a variety of fields [46] with 14 criteria were used to assess the quality of eligible studies. For example, criteria included evaluating whether the study design was evident and appropriate, whether the outcome and exposure measures were well defined and robust against measurement, misclassification bias, and whether the analytic methods were described/justified and appropriate. The overall score for this assessment was 22, after bypassing the three criteria of interventional studies, which were scored as not applicable for correlational studies (items number 5, 6, 7). After calculating the total score, papers that scored lower than the cutoff point of 0.70 were excluded from the meta-analysis by consensus of the authors. The quality of the studies was classified as low risk of bias (a score of 18 or higher) and moderate risk of bias (a score between 16 and 17). Both reviewers assigned the same overall score to the studies.
Data extraction and coding of studies
The data extraction process followed the methodology outlined in Lipsey and Wilson [44]. After ensuring that the inclusion criteria were met, the first author coded the full-text of each study according to the following variables: a) Authors and year of publication; b) Study design (i.e. cross-sectional or longitudinal); c) Sample size; d) Gender (i.e. percentage of females); e) Mean age (in years); f) Mean score of PTG; g) Mean score of rumination; h) Name of trauma; and i) Risk of bias.
Statistical analysis
To calculate the pooled correlation effect measure, we utilized Fisher’s method to transform correlations into Z-scores, which were then pooled under a random-effects model. The random-effects model, an updated version of the DerSimonian and Laird method [47], assumes that different studies estimate different but related effects. All studies included in our analysis had separate samples. We utilized the random-effects model based on the results of the Funnel plot and asymmetry test. Additionally, we investigated heterogeneity using the I-squared statistic, which ranges from 0 to 100% with values of 0 indicating no heterogeneity, 25% indicating low heterogeneity, 50% indicating moderate heterogeneity, and 75% indicating high heterogeneity. We also conducted a meta-regression to examine potential explanations for study variation by adding covariates as predictors of the pooled effect size.
We used the funnel plots and Egger’s test, which examines the likelihood of asymmetry in the final result by testing the Y-intercept=0 from a linear regression of normalized effect estimate (estimate divided by its standard error) against precision (reciprocal of the standard error of the estimate). Additionally, we stratified the data based on covariates to calculate the pooled measure of the association between rumination and PTG by various factors, whenever possible.
We used comprehensive meta-analysis software (CMA) version 3 [48] for all statistical analyses.
Results
Description of relevant studies
The search strategy identified 9926 studies, and the PRISMA flow diagram is presented in Figure 1. outlining the study selection process to ensure the reliability and validity of the study results. Following the removal of duplicate research, 6,282 papers were screened based on their titles, abstracts, and including appreciate measure of PTG or rumination. Deduplication, including the removal of identical records retrieved from multiple databases and identifying multiple articles published from the same dataset, was performed manually by exporting records into an EXCEL file and sorting them alphabetically by title and first author, as well as by date. Out of the 4409 records, those lacking measures for appreciating PTG or rumination were excluded. In this phase, the study focused on studies that utilized the ERERI [21] or a related questionnaire to ensure consistency in the measurement of rumination and PTG. In addition, out of the 1775 records, exclusions were made based on the abstract or the entire article. Of these, 98 studies were identified as potentially eligible for inclusion in the analysis and retrieved for full-text review. 42 papers were excluded due to incomplete data, the use of a different questionnaire, or failure to report the correlation value in the article. Ultimately, we included 56 papers (representing 100 effect sizes) that met our eligibility criteria.
Characteristics of the finally included studies
Table 1 summarizes the key characteristics of the studies included in the analysis.
The studies were classified as either cross-sectional (n=49) or longitudinal (n=7) and were published between 2008 Taku et al. [18] and July 2023 [32, 49-54]. The total number of participants across all studies was 17,918, with 7,967 males and 9,951 females. The age range of the participants was 13.77 to 70.04 years, with a mean age of approximately 32.66.
Quality assessment summary
As presented in additional Table 1, out of 56 papers included in the analysis, 5 articles had a moderate risk of bias due to certain limitations such as small sample size, inadequate description of the methods, or incomplete reporting of the results. The rest of the studies were judged to have high quality and low risk of bias by the authors. The mean study quality rating of the included studies was 19.38±1.69 (range 0 to 22). It is noteworthy that, as explained in detail in Section 1.5, the RoB tool was used for quality assessment. All studies that met the inclusion criteria demonstrated an inter-rater agreement of <0.70, which was set as the cutoff point, between two independent reviewers.
Synthesis of results: The main analysis
As shown in Table 2 and Figure 2 (forest plot) the point estimate of the pooled correlation meta-analysis indicated a significant positive association between rumination and PTG across different categories of studies, including cross-sectional studies (r=0.358; 95%CI, 0.323%, 0.393%; P=0.001) and longitudinal studies (r=0.342; 95%CI, 0.236%, 0.440%; P=0.001).
Furthermore, the association between rumination and PTG remained significant when adjusting for the type of trauma, with a slightly stronger effect size in studies that focused on natural disasters (r=0.375; 95%CI, 0.321%, 0.429%; P=0.001) compared to studies that focused on other types of trauma (r=0.341; 95%CI, 0.302%, 0.380%; P=0.001). The analysis also revealed that the relationship between rumination and PTG was not significantly affected by the risk of bias in the included studies (low risk of bias: r=0.364; 95%CI, 0.327%, 0.401%; P=0.001; moderate risk of bias: r=0.354; 95%CI, 0.260%, 0.439%; P=0.001). Finally, the meta-regression analysis showed that none of the covariates (i.e. sample size, year of publication, mean age, gender, type of trauma, risk of bias) significantly moderated the relationship between rumination and PTG.
Longitudinal versus cross-sectional study design
No significant difference between the two groups in the effect size (Q=2.06, P=0.151). Based on the study design, the point estimate of the effect size (ES) of the relationship between rumination and PTG was calculated. The ES in cross-sectional studies (n=49; participants=15963; mean age=33.05±7.51 years; female=8777; I2=85.35%) was 0.366 (CI, 0.353-0.380). The ES in longitudinal studies (n=7; participants=1955; mean age= 19.94±3.75 years; female=1174; I2=83.28%) was 0.277 (CI, 0.240-0.314). Despite the significant effect size and favorable heterogeneity in both cross-sectional and longitudinal study groups, there was no significant difference between the two groups in the effect size (Q=2.06, P=0.151). To better understand the temporal dynamics of rumination and PTG, future research should prioritize conducting more longitudinal studies. These studies can offer valuable insights into how these processes develop and change over time.
Gender differences
Regarding the gender distribution, the included studies were categorized based on the proportion of males and females, with 1 study consisting entirely of male participants and 8 studies consisting entirely of female participants, while the remaining 47 studies included both genders. Therefore, the focus on these two genders was driven by the availability and distribution of participants across the studies included in the analysis. The effect size was calculated for each group and compared. As shown in Table 2, the effect size for studies including both genders was 0.369 (CI, 0.356-0.382; I2=84.72%), while for studies including only females, it was 0.237 (CI, 0.179-0.294; I2=77.62%). Although both groups showed significant effect sizes with good heterogeneity, there was a significant difference between the two (Q=35.08, P=0.000), with studies including both genders showing a higher effect size than studies including only females.
Sample size and diversity variations
In the subgroup analysis based on age, studies were classified into three groups: Studies conducted on adolescents (n=13), studies conducted on adults (n=41), and studies conducted on mixed age groups (n=4). The results show that the effect size in adolescents (0.307; CI, 0.260-0.354; I2=80.64%) was lower than in adults (0.370; CI, 0.356-0.384; I2=85.09%). Additionally, the effect size in mixed age groups (0.417; CI, 0.351-0.483; I2=91.75%) was higher than in the other two groups.
There was a significant difference between the three groups (Q=17.36, P=0.000).
Reviewing the participants of the included studies reveals diverse cultural populations and countries, such as Japan [15, 18], Turkey [74], the United States [66, 69], the Caucasus [21], China [3, 12], Korea [49], and Egypt [59], among others. Additionally, some studies, such as Taku and colleagues [15], investigated two different populations from Japan and the United States. Similarly, Cann and colleagues [21] included diverse participants, such as Caucasian, African-American, and Asian-American individuals. Moreover, as shown in Table 1, the included studies encompass a variety of trauma types, including cancer [3, 66], earthquakes [12, 27], autism [54, 59], accidental injuries [53, 79], and disabilities [76], among others. These factors enhance the generalizability of the findings and provide a more nuanced understanding of how rumination influences PTG across diverse contexts and populations.
Age differences
The included studies were divided into two groups based on the mean age of the subjects: 1) Over 20 years old (n=44); and 2) under 20 years old (n=14). The results indicated that effect size (ES) in the over 20 years old group (0.366; CI, 0.351-0.380; I2=86.25%) did not differ significantly (Q=0.259, P=0.611) from the under 20 years old group (0.327; CI, 0.301-0.351; I2=83.04%). This suggests that the ES may better represent the true ES among individuals over 20 years old, as it accounts for the possible heterogeneity of the included studies.
Rumination subtype
In the included studies, three subtypes of rumination with 100 effect sizes were used to measure rumination, including DR (n=53), IR (n=44), and general rumination (n=3). Results indicated that the effect size in all three subtypes of studies based on DR (0.375; CI, 0.362 -0.388; I2=80.68%), IR (0.129; CI, 0.113-0.145; I2=92.56%) and general rumination (0.26; CI, 0.17-0.345; I2=91.35%) was significant with good heterogeneity. Moreover, there were significant differences between the effect sizes of the three subtypes of rumination (Q=72.18, P=0.000).
Heterogeneity, risk of publication bias and sensitivity analysis
The results of the publication bias tests indicate that the included studies are unlikely to be affected by publication bias. The funnel plot is the scatterplot used to visually assess the presence of publication bias or heterogeneity by examining the distribution of standard errors across individual studies (Figure 3).
A sensitivity analysis was conducted to assess the robustness of the effect size in the presence of heterogeneity. The one-study removed method was used to identify any possible study that could be responsible for the heterogeneity. The forest plot is a useful graphical display of findings from the meta-analysis and in Figure 4 shows that there are no obvious outliers, indicating that no single study could significantly influence the effect size estimate.
Retrospective power analysis
To ensure the reliability and validity of the current study, we conducted a power analysis using the formula proposed by Valentine et al. [98]. Based on the summary of effect size, the mean number per group, and the number of effect sizes, the power analysis yielded a value of 0.9993, indicating excellent statistical power despite the high heterogeneity of the included studies. Therefore, with a P=0.007, we can confidently conclude that the number of studies included in this meta-analysis is sufficient to establish the statistical significance and meaningfulness of the overall pooled correlation.
Discussion
This systematic review and meta-analysis aimed to investigate the relationship between rumination and posttraumatic growth (PTG). Surprisingly, we found a significant positive effect of rumination on PTG, despite the high degree of heterogeneity observed in the analysis. We conducted several subgroup analyses based on different subtypes of rumination, including DR (n=53), IR (n=44), and rumination (n=3), and found significant effect sizes with good heterogeneity in all three subtypes, with significant differences in heterogeneity between subgroups. These findings are consistent with previous research that has found DR and related constructs to be positively associated with PTG [3, 17]. DR plays an important role in facilitating positive psychological change by helping individuals move away from negative psychological reactions and toward a greater understanding of the post-traumatic world. This study supports the Shattered Assumptions theory [59] and the PTG model [20] and findings of Allen and colleagues [42], suggesting that DR can help individuals find positive meaning in traumatic experiences, leading to the development of PTG [21]. According to shattered assumptions theory, when individuals undergo an event that shatters their worldview (i.e. traumatic experience), they cease to view the world as benevolent and predictable, or perceive themselves as competent and invulnerable.
Additionally, studies have shown that DR can also lead to an increase in seeking and receiving perceived social support, which can reduce the negative effects of rumination and promote positive experiences leading to PTG [32, 69]. DR and IR can interact and jointly influence PTGT. On one hand, research suggests that IR may activate DR and also with DR mediating the relationship between IR and PTG [4]. On the other hand, Taku et al. [15] found that while both types of rumination are positively associated with PTG, their effects vary over time: Early IR is positively linked to PTG, whereas recent DR is the strongest predictor of current PTG. This finding suggests that the relationship between rumination and PTG is complex and influenced by various factors, including social support. It highlights the importance of considering these factors in future research and interventions aimed at promoting PTG.
Moreover, it is conceivable that IR serves as a signal, indicating the necessity for engaging in more deliberate and purposeful processing of traumatic events. In this context, experiencing intrusive thoughts might indeed facilitate the transition toward DR and PTG. While many individuals experience IR after traumatic events, some studies have shown a negative relationship between IR and PTG [4, 22, 37, 38, 102] and persistent IR can adversely affect PTG while increasing the likelihood of PTSD [22]. Thus, IR may have a negative relationship with PTG and could contribute to adverse outcomes, such as PTSD. The negative effects of IR may also vary based on contextual factors, such as the type of trauma experienced and individual coping styles. For instance, if the individual is stuck in ongoing IR and uses more avoidance-focused coping, it might lead to more decrease reports of PTG [102]. Additionally, Park and colleagues [102] reviewed studies showing that IR to be negatively associated with various indicators of adjustment and well-being. Specially, IR has been linked to a range of negative outcomes, including poorer psychological adjustment and reduced health-related quality of life for cancer survivors [103]. IR may act as a mechanism through which cancer continues to affect their distress by perpetuating reminders of the illness, either continuously or intermittently [102].
However, it is crucial to acknowledge that the link between IR and PTG is intricate and can be influenced by factors like the severity and nature of the trauma, individual coping strategies, and available social support. Additionally, Allen and colleagues’ study [42] found no significant overall effect in the association between IR and PTG. Consequently, further research is warranted to gain a more comprehensive understanding of the nuanced relationship between IR and PTG.
Different emotional regulation strategies can mediate the relationship between rumination and PTG, providing a broader context for understanding the underlying mechanisms. For example, cognitive reappraisal, as a regulatory strategy, mediates the link between DR and PTG. Higher levels of Dr may promote positive emotional focus and constructive coping, fostering cognitive reappraisal strategies that enhance perspective-taking, positivity, and emotional well-being [104].
In addition, our findings suggest that the relationship between rumination and PTG may not be affected by the timing of the trauma, as there was no significant difference in effect size between cross-sectional and longitudinal study designs. This indicates that rumination may be a useful strategy for promoting PTG both in the short-term and long-term. It is also possible that the degree to which individuals engage in thinking about their emotions and perspectives on their crisis plays a role in the PTG process, regardless of the timing of the study. These results are consistent with previous research that has found a positive relationship between rumination and PTG in both cross-sectional and longitudinal studies [21, 27]. The relationship between rumination and PTG over time is a compelling subject for study. Some research [26] suggests that the predictive effect of DR on PTG fluctuates over time. For instance, Zhou and colleagues [26] found that while DR significantly predicted PTG several years after trauma, this predictive effect was absent in earlier years. This highlights the unstable relationship between DR and PTG at different time points following trauma. These findings underscore the need for more longitudinal research to clarify the dynamic relationship between rumination and PTG over time.
Interestingly, we found a significant difference in the effect sizes between studies based on males and females. Specifically, studies including both sexes had a higher effect size than studies with only female participants. This finding is consistent with previous research suggesting that gender is associated with PTG, with females tending to exhibit higher levels of PTG than males [36, 56, 78, 87]. A meta-analysis by Vishnevsky et al. [55] also revealed a small to moderate gender difference, with women reporting more PTG than men. The findings of Hussain and Bhushan [25] also indicated that females reported significantly higher scores compared with males on traumatic experiences, posttraumatic stress, and PTG.
On the other hand, some studies, such as the meta-analysis by Johnson and Whisman [100], have indicated that females tend to ruminate more than males. Similarly, Rood and colleagues [101] reported in a meta-analysis of child and adolescent literature that girls are more likely to ruminate than boys. Specifically, certain studies [15, 99] have found that both IR and DR are higher among females compared to males. These findings may help in better analyzing the gender differences that arise in the relationship between rumination and PTG.
The higher levels of rumination and PTG reported among females could provide insights into why females exhibit a significantly stronger relationship between rumination and PTG. A possible explanation, as suggested by PTG theorists [11], is that growth requires negative life events and ruminative activity. Since females tend to engage in both IR and DR more than males [15, 99], they may also report higher levels of PTG. Females may have a greater tendency to reflect and ponder over adverse events, which may lead them to discover new possibilities in life, find meaning in the events, re-evaluate their priorities, and experience improvements in relationships and spiritual growth—factors that contribute to PTG [99]. These findings suggest that gender may play an important role in the relationship between rumination and PTG.
Conclusion
In conclusion, our meta-analysis revealed a significant effect of rumination on PTG, contrary to our initial expectation of only finding small pockets of data. Emotion regulation strategies, including rumination, are considered response-focused coping and may be particularly useful in coping with traumatic events that are rooted in the past. However, it is worth noting that previous research has suggested that response-focused emotion regulation strategies may be unhelpful or even harmful in coping with the threatening information brought about by trauma. Our study provides important insights into the potential role of rumination in promoting PTG, and highlights the importance of further research to fully understand the complex relationship between rumination and PTG. However, the significant heterogeneity in the main analyses indicates the need for caution when interpreting the results. Future studies should explore the actual effect that specific aspects of emotion regulation strategies, such as rumination, have on PTG and investigate the influence of gender on rumination and PTG It is important to note that heterogeneity is a common issue in meta analyses of psychological constructs, as these often vary widely across studies.
Limitations
The current meta-analysis has several limitations that should be considered when interpreting the results. The number of studies included in the analysis was adequate but relatively limited, which may have constrained the statistical power of the study to detect treatment efficacy. Additionally, the sample sizes in some studies were relatively small, further limiting the robustness and generalizability of the conclusions. Furthermore, the quality of the trials was suboptimal, with the majority of the included studies classified as high-risk according to the Cochrane RoB assessment.
Moreover, potential biases may have influenced the findings and to address these biases, it is important to interpret the findings with caution. For example, the inter-rater agreement could not be computed due to the database being built over several years, involving multiple raters in the screening and selection process. This variability in the screening process may have introduced inconsistencies in study inclusion. Additionally, the possibility of reporting bias cannot be entirely ruled out, as studies with significant results are more likely to be published, potentially skewing the overall findings. While the sensitivity and meta-regression analyses indicate that these biases did not significantly influence the overall results, the presence of moderate bias in a subset of studies and variability in the screening process highlight the need for standardized methods in future research. Furthermore, the potential impact of small sample sizes on the robustness of conclusions underscores the importance of including larger, well-designed studies in future meta-analyses to strengthen the reliability of the findings.
Another key limitation of this meta-analysis is the high degree of heterogeneity observed across the included studies. This variability likely reflects differences in study design, sample characteristics, and the measurement tools used for rumination and PTG. While we conducted subgroup and moderator analyses to explore potential sources of heterogeneity, as well as sensitivity analyses to ensure the robustness of the findings, the diverse methodologies and populations remain a challenge to the generalizability of the results. Future research should prioritize the use of standardized measurement tools and study designs to reduce variability and improve comparability. Furthermore, longitudinal studies are particularly needed to better provide deeper insights into how these processes evolve over time and contribute to PTG.
Although different populations and trauma types were mentioned in the included papers, the findings may not be generalizable to all populations, as the studies do not cover all demographics or trauma types. For example, despite a considerable number of studies on Chinese populations, there are few studies focusing on African populations. Similarly, while there is substantial research on medical traumas, there are limited studies addressing violence- and abuse-related trauma. This focus on specific demographics and trauma types may limit the applicability of the results to broader contexts. Therefore, future research should aim to expand studies to include other populations and trauma types to enhance generalizability.
These limitations suggest that future research in this area should aim to address these issues and further explore the relationship between rumination and PTG.
Future directions and clinical implications
Our findings hold significant practical implications. It is crucial for therapists to recognize that both IR and DR are common responses to traumatic events. Therefore, implementing training programs that encourage individuals to engage in DR is essential. Notably, designing targeted intervention programs for females to promote DR over IR in the aftermath of trauma may prove particularly beneficial.
These findings have several implications for future research in this field. First, there has been a lack of comprehensive exploration regarding whether and how rumination contributes to positive changes following traumatic events. Most of the existing correlational research focuses on discussing the relationship between rumination and negative posttraumatic outcomes such as PTSD. Thus, future studies are still needed to determine the actual effect that specific aspects of emotion regulation strategies (e.g. rumination) have on PTG.
Future studies should further investigate gender differences in the association between rumination and PTG to better understand the psychological, social, and cultural factors contributing to these variations. Examining how gender influences both intrusive and deliberate rumination, as well as their distinct contributions to PTG, could yield valuable insights. Longitudinal research is particularly needed to determine whether these gender differences persist over time and how factors such as coping strategies, cultural norms, and social support shape the rumination-PTG relationship across genders. Such studies could guide the development of tailored interventions to effectively support trauma survivors. Additionally, future studies should aim to address the limitations of this meta-analysis by increasing the number of studies, improving the quality of trials, and exploring factors that contribute to heterogeneity. Moreover, inter-rater agreement should be considered and evaluated to ensure the reliability of the database.
Ethical Considerations
Compliance with ethical guidelines
This article is review with no human or animal sample. There were no ethical considerations to be considered in this work.
Funding
This research did not receive any specific funding from granting agencies nor commercial or not-for-profit sectors.
Authors' contributions
Methodology: Jafar Hasani; Investigation, data collection, and data curation: Mehrnesa Shahabi; Data analysis: Mehrnesa Shahabi and Jafar Hasani; Writing the original draft: Mehrnesa Shahabi and Majid Asadpour; Review and editing: Majid Asadpour.
Conflict of interest
The authors declared no conflict of interest.
References
- Norris FH, Slone LB. The epidemiology of trauma and PTSD. In: Friedman MJ, Keane TM, Resick PA, editors. Handbook of PTSD: Science and practice. New York: Guilford Press; 2007. [Link]
- Wang W, Wu X, Lan X. Rumination mediates the relationships of fear and guilt to posttraumatic stress disorder and posttraumatic growth among adolescents after the Ya’an earthquake. Eur J Psychotraumatol. 2020; 11(1):1704993. [DOI:10.1080/20008198.2019.1704993] [PMID]
- Lianchao A, Tingting M. Mindfulness, rumination and post-traumatic growth in a Chinese cancer sample. Psychol Health Med. 2020; 25(1):37-44. [DOI:10.1080/13548506.2019.1612079] [PMID]
- Kim E, Bae S. Gratitude moderates the mediating effect of deliberate rumination on the relationship between intrusive rumination and post-traumatic growth. Front Psychol. 2019; 10:2665. [DOI:10.3389/fpsyg.2019.02665] [PMID]
- Sultana Eliav A, Lahav Y. Posttraumatic growth, dissociation and identification with the aggressor among childhood abuse survivors. J Trauma Dissociation. 2023; 24(3):410-25. [DOI:10.1080/15299732.2023.2181478] [PMID]
- Tedeschi RG, Calhoun LG. Trauma and transformation. California: Sage; 1995. [Link]
- Tedeschi RG, Calhoun LG. The posttraumatic growth inventory: Measuring the positive legacy of trauma. J Trauma Stress. 1996; 9(3):455-71. [DOI:10.1002/jts.2490090305]
- Janoff-Bulman R, Sheikh S. From national trauma to moralizing nation. Basic Appl Soc Psych. 2006; 28(4):325-32. [DOI:10.1207/s15324834basp2804_5]
- Nolen-Hoeksema S, Morrow J. A prospective study of depression and posttraumatic stress symptoms after a natural disaster: The 1989 Loma Prieta Earthquake. J Pers Soc Psychol. 1991; 61(1):115-21. [DOI:10.1037/0022-3514.61.1.115] [PMID]
- Nolen-Hoeksema S, Wisco BE, Lyubomirsky S. Rethinking rumination. Perspect Psychol Sci. 2008; 3(5):400-24.[DOI:10.1111/j.1745-6924.2008.00088.x] [PMID]
- Calhoun LG, Tedeschi RG. The foundations of posttraumatic growth: An expanded framework. In: Calhoun LG, Tedeschi RG, editors. Handbook of posttraumatic growth: Research & practice. London: Routledge; 2006. [Link]
- Zhou X, Wu X. Longitudinal relationships between gratitude, deliberate rumination, and posttraumatic growth in adolescents following the Wenchuan earthquake in China. Scand J Psychol. 2015; 56(5):567-72. [DOI:10.1111/sjop.12237] [PMID]
- Dunn MJ, Rodriguez EM, Barnwell AS, Grossenbacher JC, Vannatta K, Gerhardt CA, et al. Posttraumatic stress symptoms in parents of children with cancer within six months of diagnosis. Health Psychol. 2012; 31(2):176-85. [DOI:10.1037/a0025545] [PMID]
- Park CL, Fenster JR. Stress-related growth: Predictors of occurrence and correlates with psychological adjustment. J Soc Clin Psychol. 2004; 23(2):195-215. [DOI:10.1521/jscp.23.2.195.31019]
- Taku K, Cann A, Tedeschi RG, Calhoun LG. Intrusive versus deliberate rumination in posttraumatic growth across US and Japanese samples. Anxiety Stress Coping. 2009; 22(2):129-36. [DOI:10.1080/10615800802317841] [PMID]
- Cordova MJ, Giese-Davis J, Golant M, Kronenwetter C, Chang V, Spiegel D. Breast cancer as trauma: Posttraumatic stress and posttraumatic growth. J Clin Psychol Med Settings. 2007; 14:308-19. [DOI:10.1007/s10880-007-9083-6]
- Morris BA, Shakespeare-Finch J. Rumination, post-traumatic growth, and distress: Structural equation modelling with cancer survivors. Psychooncology. 2011; 20(11):1176-83. [DOI:10.1002/pon.1827] [PMID]
- Taku K, Calhoun LG, Cann A, Tedeschi RG. The role of rumination in the coexistence of distress and posttraumatic growth among bereaved Japanese university students. Death Stud. 2008; 32(5):428-44. [DOI:10.1080/07481180801974745] [PMID]
- Taku K, Kilmer RP, Cann A, Tedeschi RG, Calhoun LG. Exploring posttraumatic growth in Japanese youth. Psychol Trauma Theory Res Pract Policy. 2012; 4(4):411-9. [DOI:10.1037/a0024363]
- Tedeschi RG, Calhoun LG. Posttraumatic growth: Conceptual foundations and empirical evidence. Psychol Inq. 2004; 15(1):1-18. [DOI:10.1207/s15327965pli1501_01]
- Cann A, Calhoun LG, Tedeschi RG, Triplett KN, Vishnevsky T, Lindstrom CM. Assessing posttraumatic cognitive processes: the event related rumination inventory. Anxiety Stress Coping. 2011; 24(2):137-56. [DOI:10.1080/10615806.2010.529901] [PMID]
- Triplett KN, Tedeschi RG, Cann A, Calhoun LG, Reeve CL. Posttraumatic growth, meaning in life, and life satisfaction in response to trauma. Psychol Trauma Theory Res Pract Policy. 2012; 4(4):400-10. [DOI:10.1037/a0024204]
- Affleck G, Tennen H. Construing benefits from adversity: Adaptational significance and dispositional underpinnings. J Pers. 1996; 64(4):899-922. [DOI:10.1111/j.1467-6494.1996.tb00948.x] [PMID]
- Cann A, Calhoun LG, Tedeschi RG, Solomon DT. Posttraumatic growth and depreciation as independent experiences and predictors of well-being. J Loss Trauma. 2010; 15(3):151-66. [DOI:10.1080/15325020903375826]
- Hussain D, Bhushan B. Posttraumatic stress and growth among Tibetan refugees: The mediating role of cognitive‐emotional regulation strategies.J Clin Psychol. 2011; 67(7):720-35. [DOI:10.1002/jclp.20801] [PMID]
- Zhou X, Wu X, An Y, Chen J. The roles of rumination and social support in the associations between core belief challenge and post-traumatic growth among adolescent survivors after the Wenchuan earthquake. Acta Psychol Sin. 2014; 46(10):1509-20. [DOI:10.3724/SP.J.1041.2014.01509]
- Wang N, Chung MC, Wang Y. The relationship between posttraumatic stress disorder, trauma centrality, posttraumatic growth and psychiatric co-morbidity among Chinese adolescents. Asian J Psychiatr. 2020; 49:101940. [DOI:10.1016/j.ajp.2020.101940] [PMID]
- Romeo A, Castelli L, Zara G, Di Tella M. Posttraumatic growth and posttraumatic depreciation: associations with core beliefs and rumination. Int J Environ Res Public Health. 2022; 19(23):15938. [DOI:10.3390/ijerph192315938] [PMID]
- Calhoun LG, Cann A, Tedeschi RG, McMillan J. A correlational test of the relationship between posttraumatic growth, religion, and cognitive processing. J Trauma Stress. 2000; 13(3):521-7. [DOI:10.1023/A:1007745627077] [PMID]
- Hallam W, Morris R. Post-traumatic growth in stroke careers: A comparison of theories. Br J Health Psychol. 2014; 19(3):619-35. [DOI:10.1111/bjhp.12064] [PMID]
- Brooks M, Graham-Kevan N, Lowe M, Robinson S. Rumination, event centrality, and perceived control as predictors of post-traumatic growth and distress: The Cognitive Growth and Stress model. Br J Clin Psychol. 2017; 56(3):286-302. [DOI:10.1111/bjc.12138] [PMID]
- Xu W, Feng C, Tang W, Yang Y. Rumination, posttraumatic stress disorder symptoms, and posttraumatic growth among Wenchuan earthquake adult survivors: A developmental perspective. Front Public Health. 2022; 9:764127. [DOI:10.3389/fpubh.2021.764127] [PMID]
- Zięba M, Wiecheć K, Wójcik NE, Zięba MJ. Prioritizing positivity, styles of rumination, coping strategies, and posttraumatic growth: Examining their patterns and correlations in a prospective study. Front Psychol. 2022; 13:842979. [DOI:10.3389/fpsyg.2022.842979] [PMID]
- Liu J, Wei S, Qiu G, Li N, Wang D, Wu X, et al. Relationship between rumination and post-traumatic growth in mobile cabin hospital nurses: The mediating role of psychological resilience. Prev Med Rep. 2023; 34:102266. [DOI:10.1016/j.pmedr.2023.102266] [PMID]
- Platte S, Wiesmann U, Tedeschi RG, Kehl D. Coping and rumination as predictors of posttraumatic growth and depreciation. Chin J Traumatol. 2022; 25(5):264-71. [DOI:10.1016/j.cjtee.2022.02.001] [PMID]
- Nik Jaafar NR, Abd Hamid N, Hamdan NA, Rajandram RK, Mahadevan R, Mohamad Yunus MR, et al. Posttraumatic growth, positive psychology, perceived spousal support, and psychological complications in head and neck cancer: Evaluating their association in a longitudinal study. Front Psychol. 2022; 13:920691. [DOI:10.3389/fpsyg.2022.920691] [PMID]
- Hammer C, Podlog L, Wadey R, Galli N, Forber-Pratt AJ, Newton M. Cognitive processing following acquired disability for para sport athletes: A serial mediation model. Disabil Rehabil. 2020; 42(17):2492-500. [DOI:10.1080/09638288.2018.1563639] [PMID]
- Kiełb K, Bargiel-Matusiewicz KM, Pisula E. Posttraumatic stress symptoms and posttraumatic growth in mothers of children with intellectual disability - the role of intrusive and deliberate ruminations: A preliminary report. Front Psychol. 2019; 10:2011. [DOI:10.3389/fpsyg.2019.02011] [PMID]
- Prati G, Pietrantoni L. Optimism, social support, and coping strategies as factors contributing to posttraumatic growth: A meta-analysis. J Loss Trauma. 2009; 14(5):364-88. [DOI:10.1080/15325020902724271]
- Shiyko MP, Hallinan S, Naito T. Effects of mindfulness training on posttraumatic growth: A systematic review and meta-analysis. Mindfulness. 2017; 8:848-58. [DOI:10.1007/s12671-017-0684-3]
- Gower T, Pham J, Jouriles EN, Rosenfield D, Bowen HJ. Cognitive biases in perceptions of posttraumatic growth: A systematic review and meta-analysis. Clin Psychol Rev. 2022; 94:102159. [DOI:10.1016/j.cpr.2022.102159] [PMID]
- Allen N, Hevey D, Cogley C, O’Keeffe F. A meta-analysis of the association between event-related rumination and posttraumatic growth: The event-related rumination inventory and the posttraumatic growth inventory. J Trauma Stress. 2022; 35(6):1575-85. [DOI:10.1002/jts.22875] [PMID]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int J Surg. 2021; 88:105906. [DOI:10.1016/j.ijsu.2021.105906] [PMID]
- Lipsey MW, Wilson DB. Practical meta-analysis. California: SAGE Publications Inc; 2001. [Link]
- Protogerou C, Hagger MS. A checklist to assess the quality of survey studies in psychology. Methods Psychol. 2020; 3:100031. [DOI:10.1016/j.metip.2020.100031]
- Kmet LM, Cook LS, Lee RC. Standard quality assessment criteria for evaluating primary research papers from a variety of fields. Alberta: Alberta Heritage Foundation for Medical Research; 2004. [Link]
- DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986; 7(3):177-88. [DOI:10.1016/0197-2456(86)90046-2] [PMID]
- Borenstein M, Higgins JP. Meta-analysis and subgroups. Prev Sci. 2013; 14:134-43. [DOI:10.1007/s11121-013-0377-7] [PMID]
- Ryu JH, Suh KH. Self-disclosure and post-traumatic growth in Korean adults: A multiple mediating model of deliberate rumination, positive social responses, and meaning of life. Front Psychol. 2022; 13:878531. [DOI:10.3389/fpsyg.2022.878531] [PMID]
- Luu TT. Family support and posttraumatic growth among tourism workers during the COVID-19 shutdown: The role of positive stress mindset. Tour Manag. 2022; 88:104399.[DOI:10.1016/j.tourman.2021.104399] [PMID]
- Eames C, O’Connor D. The role of repetitive thinking and spirituality in the development of posttraumatic growth and symptoms of posttraumatic stress disorder. Plos One. 2022; 17(8):e0272036. [DOI:10.1371/journal.pone.0272036] [PMID]
- David G, Shakespeare-Finch J, Krosch D. Testing theoretical predictors of posttraumatic growth and posttraumatic stress symptoms. Psychol Trauma. 2022; 14(3):399-409. [DOI:10.1037/tra0000777] [PMID]
- Pan Y, Zhao H, Xu H, Huang Y, Dong C. Post accidental injury: Mediating roles of emotional expressivity, rumination, and posttraumatic growth. Nurs Health Sci. 2022; 24(1):236-44. [DOI:10.1111/nhs.12919] [PMID]
- Feng Y, Chen K, Zou Y, Zhou X, Liu Q, Zhong D, et al. Posttraumatic growth and rumination among parents of children with autism spectrum disorder: The mediating role of social support. J Psychiatr Res. 2022; 154:11-8. [DOI:10.1016/j.jpsychires.2022.07.024] [PMID]
- Vishnevsky T, Cann A, Calhoun LG, Tedeschi RG, Demakis GJ. Gender differences in self-reported posttraumatic growth: A meta-analysis. Psychol Women Q. 2010; 34(1):110-20. [DOI:10.1111/j.1471-6402.2009.01546.x]
- Leong Abdullah MFI, Hami R, Appalanaido GK, Azman N, Mohd Shariff N, Md Sharif SS. Diagnosis of cancer is not a death sentence: Examining posttraumatic growth and its associated factors in cancer patients. J Psychosoc Oncol. 2019; 37(5):636-51. [DOI:10.1080/07347332.2019.1574946] [PMID]
- Cui PP, Wang PP, Wang K, Ping Z, Wang P, Chen C. Post-traumatic growth and influencing factors among frontline nurses fighting against COVID-19. Occup Environ Med. 2021; 78(2):129-35. [DOI:10.1136/oemed-2020-106540] [PMID]
- Janoff-Bulman R. Assumptive worlds and the stress of traumatic events: Applications of the schema construct. Soc Cogn. 1989; 7(2):113-36. [DOI:10.1521/soco.1989.7.2.113]
- Mohamed Elkayal M, Mohamed Taha S. Influence of rumination and coping on post-traumatic growth among mothers of children with autism. Egypt J Health Care. 2020; 11(2):890-1003. [DOI:10.21608/ejhc.2020.226066]
- Zhang W, Yan TT, Du YS, Liu XH. Relationship between coping, rumination and posttraumatic growth in mothers of children with autism spectrum disorders. Res Autism Spectr Disord. 2013; 7(10):1204-10. [DOI:10.1016/j.rasd.2013.07.008]
- Zeng W, Zeng Y, Xu Y, Huang D, Shao J, Wu J, et al. The influence of post-traumatic growth on college students’ creativity during the COVID-19 pandemic: The mediating role of general self-efficacy and the moderating role of deliberate rumination. Front Psychol. 2021; 12:665973. [DOI:10.3389/fpsyg.2021.665973]
- Li T, Liu T, Han J, Zhang M, Li Z, Zhu Q, Wang A. The relationship among resilience, rumination and posttraumatic growth in hemodialysis patients in North China. Psychol Health Med. 2018; 23(4):442-53. [DOI:10.1080/13548506.2017.1384553] [PMID]
- Ramos C, Leal I, Costa PA, Tapadinhas AR, Tedeschi RG. An item-level analysis of the posttraumatic stress disorder checklist and the posttraumatic growth inventory and its associations with challenge to core beliefs and rumination. Front Psychol. 2018; 9:2346. [DOI:10.3389/fpsyg.2018.02346] [PMID]
- Cuijpers P, Noma H, Karyotaki E, Vinkers CH, Cipriani A, Furukawa TA. A network meta-analysis of the effects of psychotherapies, pharmacotherapies and their combination in the treatment of adult depression. World Psychiatry. 2020; 19(1):92-107. [DOI:10.1002/wps.20701] [PMID]
- Choi S, In H. Paths from core belief disruption to post-traumatic stress symptoms and post-traumatic growth among Korean undergraduates: The mediating role of rumination. Int J Psychol. 2020; 55(2):215-23. [DOI:10.1002/ijop.12578] [PMID]
- Rider Mundey K, Nicholas D, Kruczek T, Tschopp M, Bolin J. Posttraumatic growth following cancer: the influence of emotional intelligence, management of intrusive rumination, and goal disengagement as mediated by deliberate rumination. J Psychosoc Oncol. 2019; 37(4):456-77. [DOI:10.1080/07347332.2018.1514449] [PMID]
- Hirooka K, Fukahori H, Taku K, Togari T, Ogawa A. Quality of death, rumination, and posttraumatic growth among bereaved family members of cancer patients in home palliative care. Psychooncology. 2017; 26(12):2168-74. [DOI:10.1002/pon.4446] [PMID]
- Wu K, Zhang Y, Liu Z, Zhou P, Wei C. Coexistence and different determinants of posttraumatic stress disorder and posttraumatic growth among Chinese survivors after earthquake: Role of resilience and rumination. Front Psychol. 2015; 6:1043. [DOI:10.3389/fpsyg.2015.01043]
- Xu W, Jiang H, Zhou Y, Zhou L, Fu H. Intrusive rumination, deliberate rumination, and posttraumatic growth among adolescents after a tornado: The role of social support. J Nerv Ment Dis. 2019; 207(3):152-6. [DOI:10.1097/NMD.0000000000000926] [PMID]
- Wozniak JD, Caudle HE, Harding K, Vieselmeyer J, Mezulis AH. The effect of trauma proximity and ruminative response styles on posttraumatic stress and posttraumatic growth following a university shooting. Psychol Trauma. 2020; 12(3):227-34. [DOI:10.1037/tra0000505] [PMID]
- Zhang Y, Xu W, Yuan G, An Y. The relationship between posttraumatic cognitive change, posttraumatic stress disorder, and posttraumatic growth among Chinese adolescents after the Yancheng tornado: The mediating effect of rumination. Front Psychol. 2018; 9:474. [DOI:10.3389/fpsyg.2018.00474] [PMID]
- Taku K, Cann A, Tedeschi RG, Calhoun LG. Core beliefs shaken by an earthquake correlate with posttraumatic growth. Psychol Trauma. 2015; 7(6):563-9. [DOI:10.1037/tra0000054] [PMID]
- Su YJ, Chen SH. Emerging posttraumatic growth: A prospective study with pre-and posttraumatic psychological predictors. Psychol Trauma. 2015; 7(2):103-11. [DOI:10.1037/tra0000008] [PMID]
- Gul E, Karanci AN. What determines posttraumatic stress and growth following various traumatic events? A study in a Turkish community sample. J Trauma Stress. 2017; 30(1):54-62. [DOI:10.1002/jts.22161] [PMID]
- Benetato BB. Posttraumatic growth among operation enduring freedom and operation Iraqi freedom amputees. J Nurs Scholarsh. 2011; 43(4):412-20. [DOI:10.1111/j.1547-5069.2011.01421.x] [PMID]
- Hammer C, Podlog L, Wadey R, Galli N, Forber-Pratt AJ, Newton M. From core belief challenge to posttraumatic growth in para sport athletes: moderated mediation by needs satisfaction and deliberate rumination. Disabil Rehabil. 2019; 41(20):2403-11. [DOI:10.1080/09638288.2018.1466203] [PMID]
- Wilson B, Morris BA, Chambers S. A structural equation model of posttraumatic growth after prostate cancer. Psychooncology. 2014; 23(11):1212-9. [DOI:10.1002/pon.3546] [PMID]
- Sharp L, Redfearn D, Timmons A, Balfe M, Patterson J. Posttraumatic growth in head and neck cancer survivors: Is it possible and what are the correlates? Psychooncology. 2018; 27(6):1517-23. [DOI:10.1002/pon.4682] [PMID]
- Dong C, Gong S, Jiang L, Deng G, Liu X. Posttraumatic growth within the first three months after accidental injury in China: The role of self-disclosure, cognitive processing, and psychosocial resources. Psychol Health Med. 2015; 20(2):154-64. [DOI:10.1080/13548506.2014.913795] [PMID]
- Zhou X, Wu X, Fu F, An Y. Core belief challenge and rumination as predictors of PTSD and PTG among adolescent survivors of the Wenchuan earthquake. Psychol Trauma. 2015; 7(4):391-7. [DOI:10.1037/tra0000031] [PMID]
- Zhou X, Wu X. The relationship between rumination, posttraumatic stress disorder, and posttraumatic growth among Chinese adolescents after earthquake: A longitudinal study. J Affect Disord. 2016; 193:242-8. [DOI:10.1016/j.jad.2015.12.076] [PMID]
- Lindstrom CM, Cann A, Calhoun LG, Tedeschi RG. The relationship of core belief challenge, rumination, disclosure, and sociocultural elements to posttraumatic growth. Psychol Trauma Theory Res Pract Policy. 2013; 5(1):50-5. [DOI:10.1037/a0022030]
- Wu X, Zhou X, Wu Y, An Y. The role of rumination in posttraumatic stress disorder and posttraumatic growth among adolescents after the Wenchuan earthquake. Front Psychol. 2015; 6:1335. [PMID]
- Liu A, Wang W, Wu X. The mediating role of rumination in the relation between self-compassion, posttraumatic stress disorder, and posttraumatic growth among adolescents after the Jiuzhaigou earthquake. Curr Psychol. 2021; 42:3846–59.[DOI:10.1007/s12144-021-01643-5]
- Eze JE, Ifeagwazi CM, Chukwuorji JC. Core beliefs challenge and posttraumatic growth: Mediating role of rumination among internally displaced survivors of terror attacks. J Happiness Stud. 2020; 21(2):659-76. [DOI:10.1007/s10902-019-00105-x]
- García FE, Cova F, Rincón P, Vázquez C. Trauma or growth after a natural disaster? The mediating role of rumination processes. Eur J Psychotraumatol. 2015; 6:26557. [DOI:10.3402/ejpt.v6.26557] [PMID]
- Shand LK, Cowlishaw S, Brooker JE, Burney S, Ricciardelli LA. Correlates of post-traumatic stress symptoms and growth in cancer patients: A systematic review and meta-analysis. Psychooncology. 2015; 24(6):624-34. [DOI:10.1002/pon.3719] [PMID]
- Allbaugh LJ, Wright MOD, Folger SF. The role of repetitive thought in determining posttraumatic growth and distress following interpersonal trauma. Anxiety Stress Coping. 2016; 29(1):21-37. [DOI:10.1080/10615806.2015.1015422] [PMID]
- Yang SK, Ha Y. Predicting posttraumatic growth among firefighters: The role of deliberate rumination and problem-focused coping. Int J Environ Res Public Health. 2019; 16(20):3879. [DOI:10.3390/ijerph16203879] [PMID]
- Bosson JV, Kelley ML, Jones GN. Deliberate cognitive processing mediates the relation between positive religious coping and posttraumatic growth. J Loss Trauma. 2012; 17(5):439-51. [DOI:10.1080/15325024.2011.650131]
- Wen X, An Y, Zhou Y, Du J, Xu W. Mindfulness, posttraumatic stress symptoms, and posttraumatic growth in aid workers: The role of self-acceptance and rumination. J Nerv Ment Dis. 2021; 209(3):159-65. [DOI:10.1097/NMD.0000000000001275] [PMID]
- García FE, Duque A, Cova F. The four faces of rumination to stressful events: A psychometric analysis. Psychol Trauma. 2017; 9(6):758-65. [DOI:10.1037/tra0000289] [PMID]
- Hill EM, Watkins K. Women with ovarian cancer: Examining the role of social support and rumination in posttraumatic growth, psychological distress, and psychological well-being. J Clin Psychol Med Settings. 2017; 24(1):47-58. [DOI:10.1007/s10880-016-9482-7] [PMID]
- Freedle A, Oliveira E. The relationship between disclosure, social reactions, rumination and posttraumatic growth following miscarriage. Traumatology. 2022; 28(4):445-57. [DOI:10.1037/trm0000360]
- Lafarge C, Usher L, Mitchell K, Fox P. The role of rumination in adjusting to termination of pregnancy for fetal abnormality: rumination as a predictor and mediator of posttraumatic growth. Psychol Trauma. 2020; 12(1):101-9. [DOI:10.1037/tra0000440] [PMID]
- Kramer LB, Whiteman SE, Witte TK, Silverstein MW, Weathers FW. From trauma to growth: the roles of event centrality, posttraumatic stress symptoms, and deliberate rumination. Traumatology. 2020; 26(2):152-9. [DOI:10.1037/trm0000214]
- Aricioglu A. The mediating role of adaptive cognitive emotion regulation in the effect of deliberate rumination upon posttraumatic growth. World J Educ. 2021; 11(5):61-70. [DOI:10.5430/wje.v11n5p61]
- Valentine JC, Pigott TD, Rothstein HR. How many studies do you need? A primer on statistical power for meta-analysis. J Educ Behav Stat. 2010; 35(2):215-47. [DOI:10.3102/1076998609346961]
- Aslam N, Kamal A. Gender difference in distress responses, rumination patterns, perceived social support and posttraumatic growth among flood affected individuals. J PakPsychiatr Soc. 2013; 10(02):86-90. [Link]
- Johnson DP, Whisman MA. Gender differences in rumination: A meta-analysis. Pers Individ Dif. 2013; 55(4):367-74. [DOI:10.1016/j.paid.2013.03.019] [PMID]
- Rood L, Roelofs J, Bogels SM, Nolen-Hoeksema S, Schouten E. The influence of emotion-focused rumination and distraction on depressive symptoms in non-clinical youth: A meta-analytic review. Clin Psychol Rev. 2009; 29(7):607-16. [DOI:10.1016/j.cpr.2009.07.001] [PMID]
- Park CL, Chmielewski J, Blank TO. Post-traumatic growth: finding positive meaning in cancer survivorship moderates the impact of intrusive thoughts on adjustment in younger adults. Psychooncology. 2010; 19(11):1139-47. [DOI:10.1002/pon.1680] [PMID]
- Baider L, Kaplan De-Nour A. Psychological distress and intrusive thoughts in cancer patients. J Nerv Ment Dis. 1997; 185(5):346-8. [DOI:10.1097/00005053-199705000-00010] [PMID]
- Zhou C, Ning L, Li H. Purposeful rumination on childhood trauma and post-traumatic growth among college students: A moderated mediation model. J Psychol Afr. 2024; 34(3):308-15. [DOI:10.1080/14330237.2024.2363702]
Article Type: Systematic Review |
Subject:
Health Education and Promotion
Received: 2024/10/25 | Accepted: 2024/11/20 | Published: 2025/01/29
Received: 2024/10/25 | Accepted: 2024/11/20 | Published: 2025/01/29
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
