

Volume 10, Issue 2 (4-2025)
CJHR 2025, 10(2): 111-120 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
naderi M, amiri A, yazdanpanah M, naderyan I. Barriers to Participation in Physical Activity: The Role of Age and Gender Differences. CJHR 2025; 10 (2) :111-120
URL: http://cjhr.gums.ac.ir/article-1-415-en.html
URL: http://cjhr.gums.ac.ir/article-1-415-en.html


1- Department of Physical Education, Technical and Vocational University (TVU), Tehran, Iran
2- Department of Management Behavior, School of Humanities, Rasht Branch, Islamic Azad University, Rasht, Iran ,aminamiri071@gmail.com
2- Department of Management Behavior, School of Humanities, Rasht Branch, Islamic Azad University, Rasht, Iran ,
Full-Text [PDF 478 kb]
(490 Downloads)
| Abstract (HTML) (628 Views)
Full-Text: (112 Views)
Introduction
Physical activity, as a cornerstone of physical and mental health, plays a critical role in preventing chronic diseases and enhancing quality of life. However, in recent decades, modern lifestyles characterized by urbanization, technological advancements, and the mechanization of daily tasks have significantly reduced physical activity levels among individuals. This sedentary behavior, particularly in urban communities, has been associated with an increased prevalence of conditions such as obesity, type 2 diabetes, and cardiovascular diseases, placing a substantial burden on healthcare systems [1]. The World Health Organization (WHO) reports that over 50% of the global population fails to meet the recommended physical activity levels (at least 150 minutes of moderate aerobic activity per week), highlighting the urgent need for targeted interventions to promote an active lifestyle [2]. In Iran, despite a rich sports culture and historical emphasis on well-being, public participation in physical activity remains below global standards [3]. Rasht, the capital of Gilan Province, exemplifies this paradox. Blessed with a favorable climate and a significant history of sporting achievements, the city nonetheless struggles with suboptimal physical activity levels among its residents. Factors such as infrastructural limitations, socio-cultural conditions, and individual differences may explain this situation, yet a thorough understanding of these barriers requires localized investigation.
Previous studies have demonstrated that barriers to physical activity are influenced by variables such as age and gender. For instance, Rasekh et al., in a study on Iranian women, identified limited access to sports facilities, lack of time, and psychological barriers like fear of injury as primary deterrents [4]. Similarly, Geelen et al., in a comprehensive review, reported environmental barriers (e.g. lack of sports spaces), social influences (e.g. insufficient family support), and personal beliefs as key factors affecting participation in physical activity [5]. However, most of these studies have either been conducted broadly or focused on specific groups (e.g. women or the elderly), with limited attention to age and gender differences within a specific urban context. Research also suggests that overcoming barriers to physical activity can lead to sustainable participation patterns. Vafaee-Najar et al., in their study, highlighted that social factors and structural-cultural barriers operate in a staged manner (individual, familial, and environmental), and individuals’ participation in health programs depends on their ability to manage these factors [6]. This perspective underscores the importance of designing localized programs tailored to the specific needs and constraints of each community. Nevertheless, comprehensive data on the barriers to physical activity in Rasht, considering age and gender differences, remain scarce. This research gap necessitates a focused study to identify these barriers accurately and propose contextually appropriate solutions.
The aim of this study is to investigate the barriers to physical health-related physical activity among Rasht citizens, with an emphasis on age and gender differences. The study seeks to address the following questions: What differences exist in the barriers to physical activity across various age groups in Rasht, and what are the primary barriers to physical activity among Rasht citizens based on gender? The findings of this research can assist policymakers and urban planners in designing targeted interventions to enhance public participation in physical activity and improve community health.
Materials and Methods
This study is a descriptive-analytical, cross-sectional research aimed at identifying barriers to physical health-related physical activity among Rasht citizens. A cross-sectional design was chosen due to its ability to examine variables within a specific timeframe and analyze differences based on age and gender [7].
Study population and sampling
The study population comprised all Rasht residents in 2024, aged 18 to 65 years. The sample size was determined using Cochran’s formula, with a 95% confidence level (z=1.96), a 5% margin of error (d=0.05), and an initial estimate of physical activity participation proportion (P=0.5), yielding a minimum sample size of 384 individuals [8]. Accounting for a 10% dropout rate, the final sample size was increased to 422 participants. Multi-stage cluster sampling was employed. The study population consisted of households covered by Rasht’s comprehensive health centers in 2024, selected as representatives of the city’s urban population. Rasht was divided into five geographical regions, and using the multi-stage cluster sampling method, three regions (60% of the total) were randomly selected in the first stage. Within each region, households were visited in person, and one eligible individual (aged 18–65 and a permanent Rasht resident) per household was chosen as the primary respondent. Selection within each household was conducted via simple random sampling (using a lottery method by the researchers) among eligible individuals. After excluding incomplete data, the final analysis included 408 participants (204 men and 204 women). Inclusion criteria included residency in Rasht for at least one year, the ability to complete the questionnaire, and informed consent to participate. Individuals with severe physical or mental conditions that hindered their ability to respond were excluded.
Research instruments
Data were collected using two primary tools:
Demographic questionnaire
This self-reported questionnaire included variables such as age, gender, marital status, education level, occupation, and monthly income.
Physical activity barriers questionnaire
The primary tool was the exercise benefits/barriers scale (EBBS), designed and developed by Ortenberg et al. (1990). The barriers section comprises 14 questions categorized into the following subscales to identify individual, interpersonal, and structural barriers:
Physical activity environment: 6 questions, score range 6–24 (each question scored 1–4);
Time expenditure: 3 questions, score range 3–12;
Physical exhaustion: 3 questions, score range 3–12;
Lack of family encouragement: 2 questions, score range 2–8.
The total score ranges from 14 to 56, indicating the level of barriers from low to high. The convergent construct validity and internal consistency reliability of this tool were confirmed by Ortenberg et al. (1990) with a Cronbach’s α of 87% [8]. In Iran, Salehzade et alvalidated its convergent construct validity and internal consistency reliability with a similar Cronbach’s α [9].
Data collection method
Data were gathered through in-person interviews at participants’ homes or in open spaces, with questionnaires completed by trained researchers. Prior to the study, the research objectives were explained to participants, and written informed consent was obtained. To ensure data quality, completed questionnaires were reviewed, and incomplete or ambiguous responses were clarified with participants. Data collection occurred over a three-month period.
Data analysis
Data were analyzed using SPSS software, version 26. Descriptive statistics (Mean±SD, frequency, and percentage) were used to describe demographic characteristics and physical activity barriers. Normality of data distribution was assessed using the Shapiro-Wilk test prior to parametric analyses, confirming normal distribution (P>0.05). To examine differences in barriers across age and gender groups, independent t-tests (for gender comparisons) and one-way analysis of variance (ANOVA) (for age group comparisons) were applied. Post-hoc Tukey tests were conducted for pairwise comparisons when ANOVA results indicated significant differences. The significance level for all analyses was set at 0.05.
Results
Demographic characteristics of participants
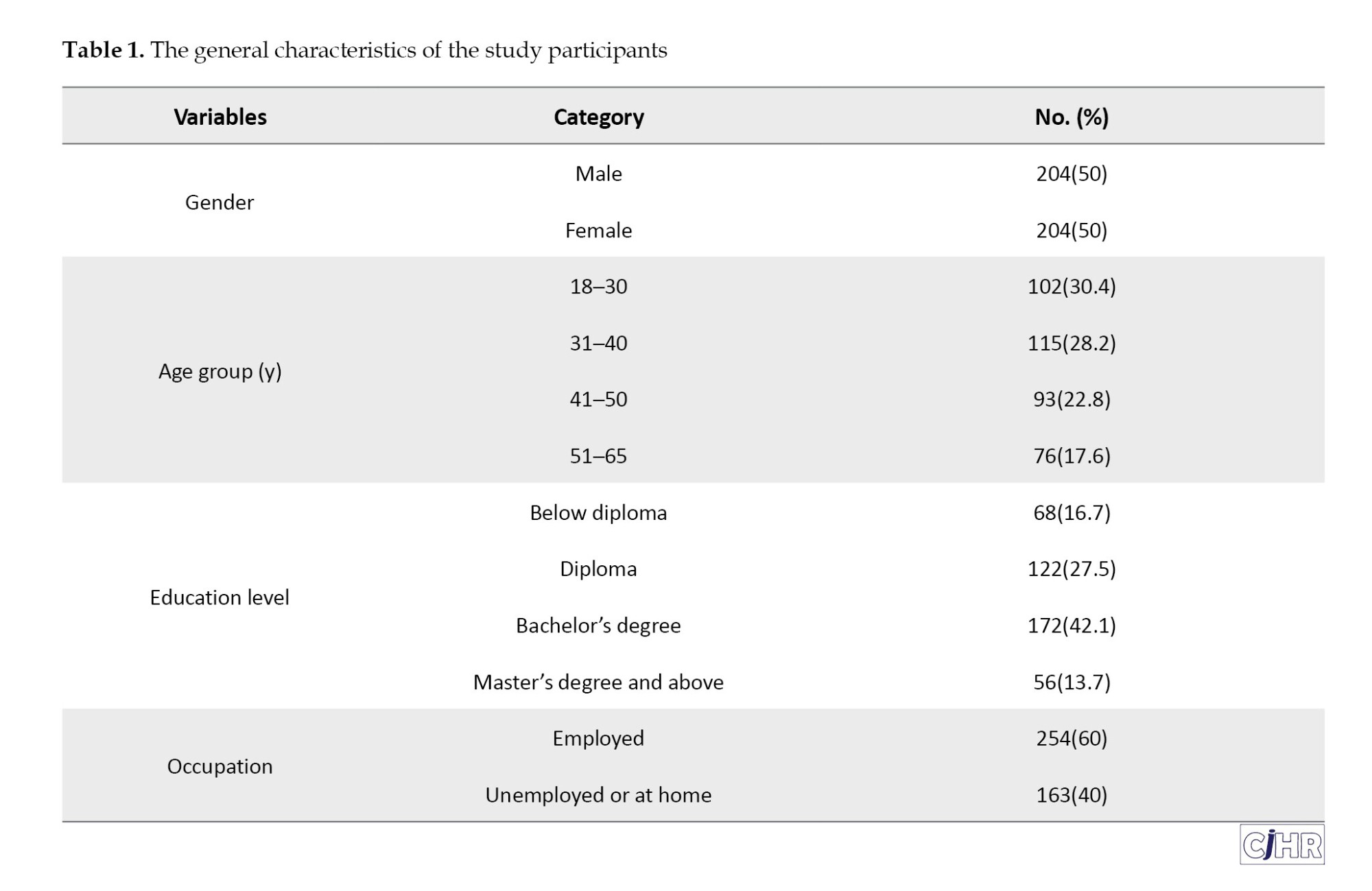
In this study, 422 citizens of Rasht participated; however, after excluding incomplete data, the information from 408 individuals (96.7%) was used for the final analysis. Of these, 204 participants (50%) were female, and 204 (50%) were male. The participants were divided into four age groups: 18–30 years (30.4%, n=124), 31–40 years (28.2%, n=115), 41–50 years (22.8%, n=93), and 51–65 years (18.6%, n=76) (Table 1).
Frequency of study items
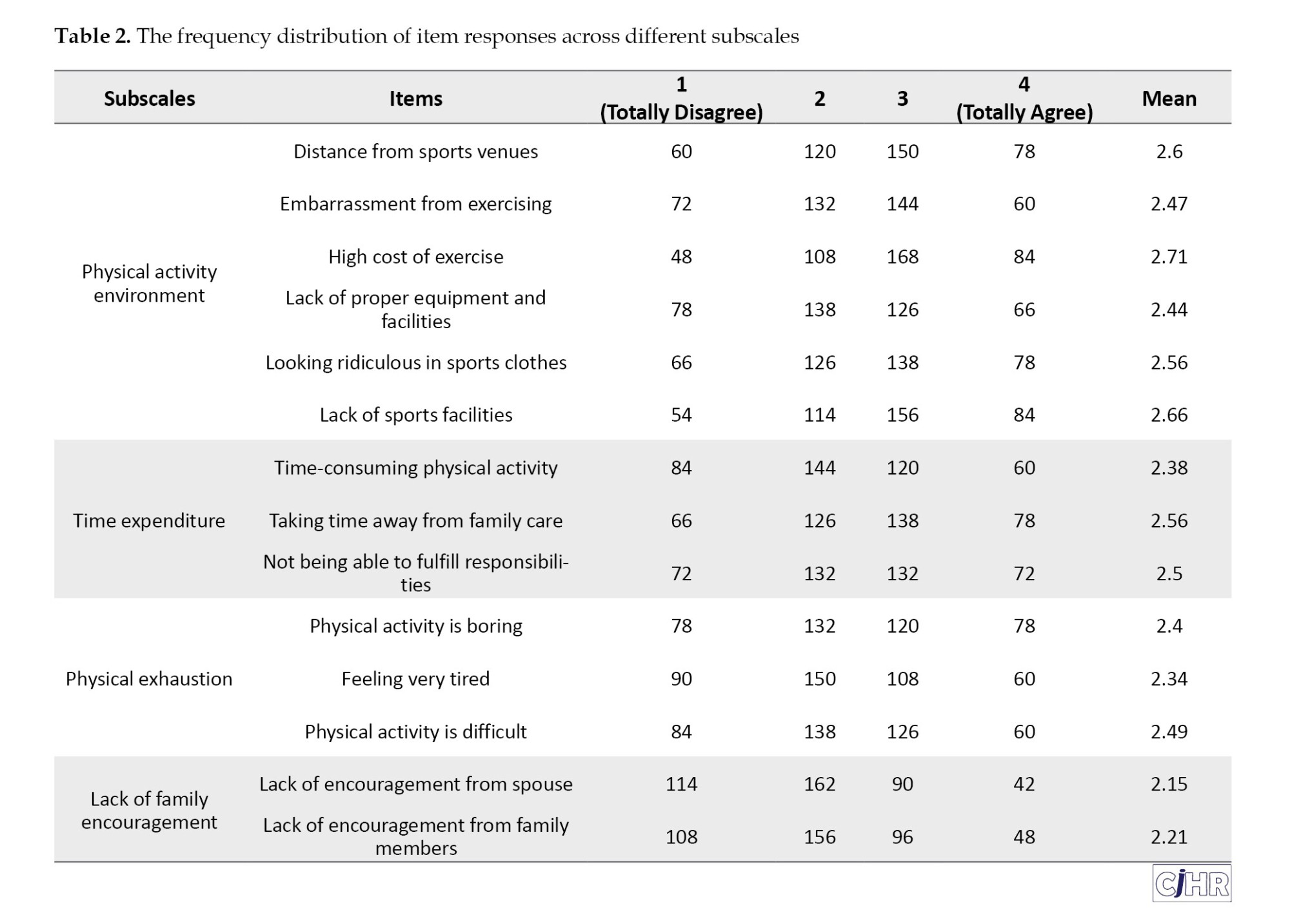
As observed in Table 2, the frequency of participants’ responses to the study questions is presented. The highest mean score was related to the high cost of exercise followed by distance from sports venues.
Based on the results of Table 3, the overall mean score of barriers to physical activity, as measured by the EBBS scale (range: 14–56), was 32.4±8.5, indicating a moderate level of barriers among participants. The analysis revealed that the mean score for women (34.1±8.8) was significantly higher than that for men (30.8±8.2) (t406=3.41, P=0.001). Additionally, a significant difference was observed across age groups (F3, 404=8.76, P<0.001). Post-hoc Tukey tests indicated that the 51–65 age group reported significantly more barriers compared to the 18–30 age group (P<0.001). In the “physical activity environment” subscale, the independent t-test revealed a significant difference between men and women (t406=2.58, P=0.01), indicating that women perceived greater environmental barriers. The highest mean score was recorded among women in the 51–65 age group. Analysis of variance (ANOVA) also confirmed a significant difference across age groups (F3, 404=3.45, P=0.02), and the post-hoc Tukey test showed a significant difference between the 18–30 and 51–65 age groups (P<0.001), suggesting that environmental barriers increase with age.
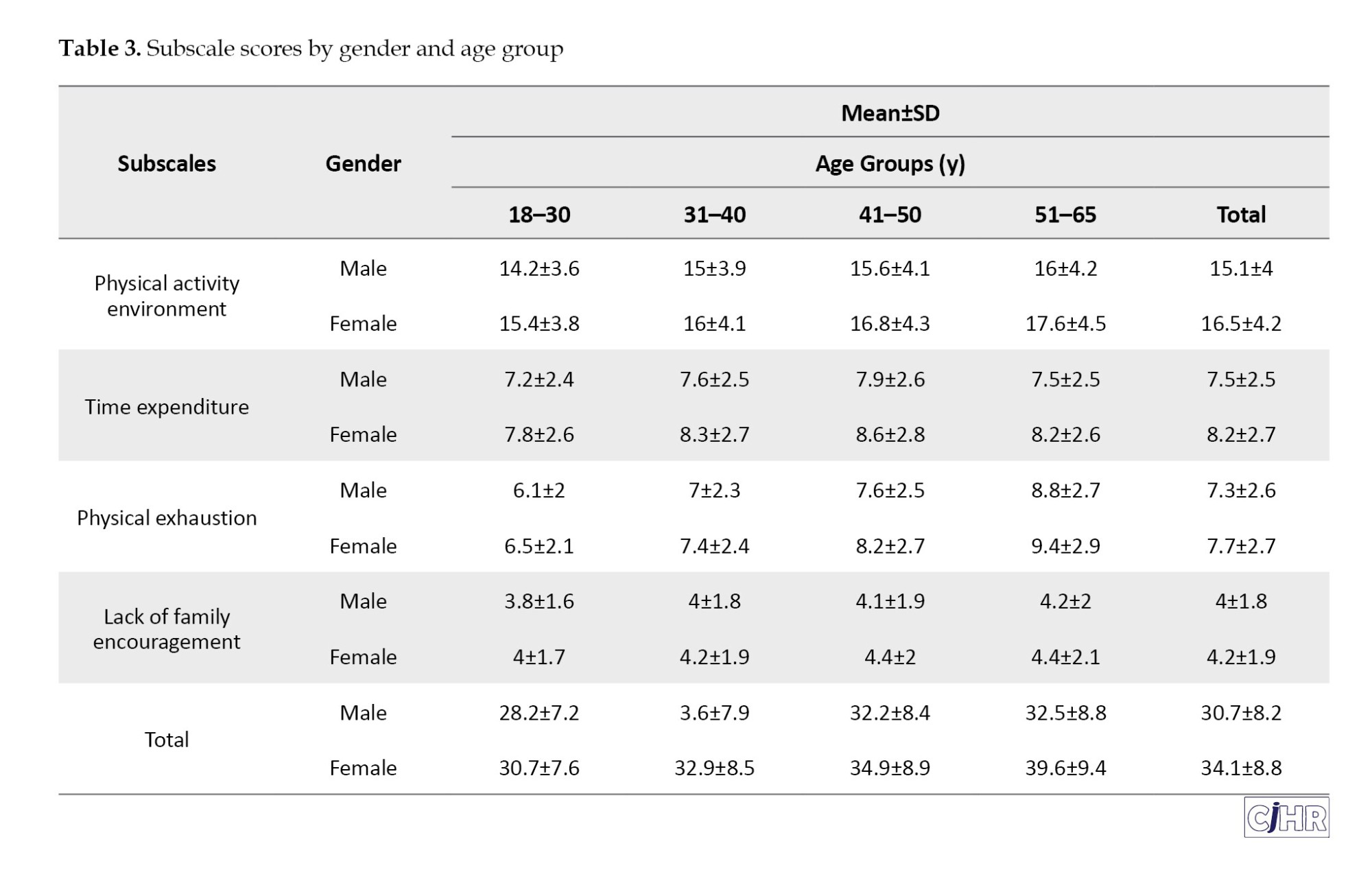
In the “time expenditure” subscale, the independent t-test indicated a significant difference between men and women (t406=2.03, P=0.04), highlighting greater time constraints among women, particularly in the 41–50 age group. However, ANOVA results showed no significant difference across age groups (F3, 404=1.12, P=0.34), as the overall mean scores were similar across all age groups.
In the “physical exhaustion” subscale, the independent t-test showed no significant difference between men and women (t406=1.12, P=0.26), although women in the 51–65 age group had the highest mean score. ANOVA results confirmed a significant difference across age groups (F3, 404=10.23, P<0.001), and the Tukey test identified a significant difference between the 18–30 and 51–65 age groups (P<0.001), indicating that physical exhaustion increases with age.
In the “lack of family encouragement” subscale, the independent t-test revealed no significant difference between men and women (t406=0.89, P=0.37). Similarly, ANOVA results showed no significant difference across age groups (F3, 404=1.45, P=0.23), as the overall mean scores were low across all groups, suggesting that this barrier is of minor importance.
Gender and age differences in physical activity barrier factors
The results of comparing the mean scores of barrier factors based on gender and age groups are presented in Table 4.
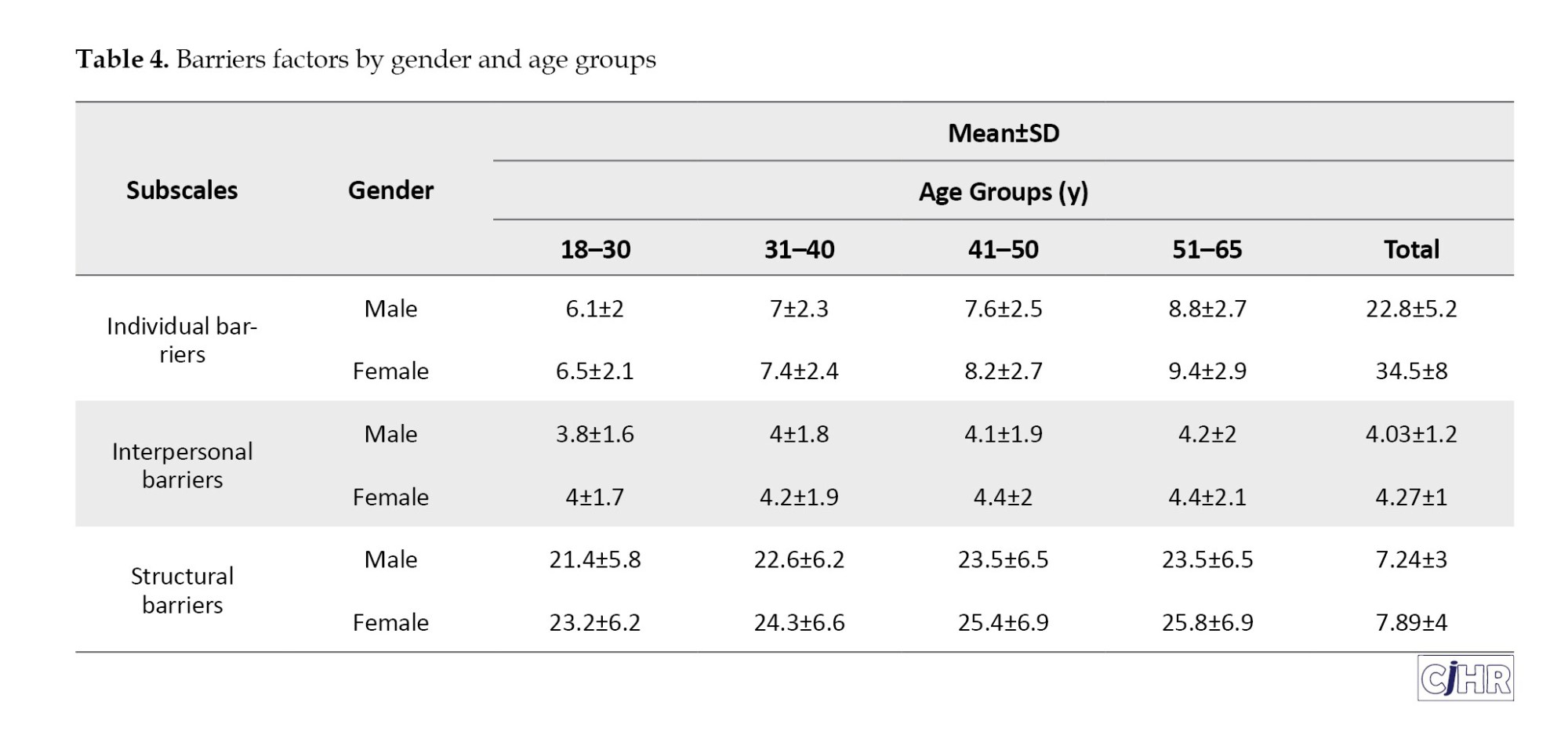
The independent t-test analysis showed that women had significantly higher scores in the “physical activity environment” (Mean±SD=10.2±2.1) and “lack of family encouragement” (Mean±SD=5.1±1.3) subscales compared to men (Mean±SD=9.1±2.0 and 4.3±1.2, respectively) (P<0.01). However, no significant difference was observed in the “lack of facilities and equipment” subscale (P=0.15). In the ANOVA analysis, the 51–65 age group had significantly higher scores across all subscales compared to the 18–30 age group (P<0.05).
Individual barriers (physical exhaustion)
The independent t-test results indicated no significant difference between men (Mean±SD=7.3±2.6) and women (Mean±SD=7.7±2.7) in physical exhaustion (t406=1.12, P=0.26). However, women in the 51–65 age group reported the highest mean score. One-way analysis of variance (ANOVA) confirmed a significant difference across age groups (F3, 404=10.23, P<0.001), and the post-hoc Tukey test revealed a statistically significant difference between the 18–30 age group (mean=6.3) and the 51–65 age group (mean=9.1) (P<0.001). This finding suggests that the intensity of physical exhaustion increases with age.
Interpersonal barriers (lack of family encouragement)
The independent t-test showed no significant difference between men (Mean±SD=4.0±1.8) and women (Mean±SD=4.2±1.9) in lack of family encouragement (t406=0.89, P=0.37). Similarly, ANOVA revealed no significant difference across age groups (F3, 404=1.45, P=0.23). These results indicate that the lack of family encouragement was of minor importance in this study.
Structural barriers (physical activity environment + time expenditure)
The independent t-test confirmed a significant difference between men (Mean±SD=22.6±6.3) and women (Mean±SD=24.7±6.7) in structural barriers (t406=2.75, P=0.006), with women reporting greater structural barriers, peaking in the 51–65 age group with a mean of 25.8. ANOVA also showed a significant difference across age groups (F3, 404=2.95, P=0.03), and the post-hoc Tukey test identified a significant difference between the 18–30 age group (mean=22.3) and the 51–65 age group (mean=24.7) (P=0.02). These findings highlight the greater impact of structural barriers with increasing age.
Discussion
The primary aim of this study was to investigate the barriers to participation in physical activity related to physical health among Rasht citizens, with a focus on analyzing gender and age differences. The results revealed that barriers to physical activity can be categorized into three main domains: Individual barriers (physical exhaustion), interpersonal barriers (lack of family encouragement), and structural barriers (environmental factors and time constraints). These findings align with contemporary ecological frameworks while highlighting the unique characteristics of the Rasht community.
Individual barriers: Physical exhaustion
The analysis indicated that physical exhaustion, as an individual barrier, significantly intensifies with age, particularly among older individuals, while no significant gender differences were observed. This finding supports the hypothesis that age influences individual barriers but rejects the hypothesis of gender differences in this domain. The greater intensity of exhaustion in older age groups, especially among older women, aligns with recent global evidence. For instance, Salmi et al. found that barriers to physical activity in adults include factors such as low mood, lack of time, health problems, and a lack of companionship… These barriers are particularly pronounced in individuals with a non-native language, single parents, those aged 30-44 years, and those with low household incomes. These barriers are particularly pronounced in individuals with a non-native language, single parents, those aged 30-44 years, and those with low household incomes [10]. Similarly, Uddin et al. (2018) argued that the subjective experience of exhaustion in older adults is tied to physiological changes, reducing their inclination toward physical activity [11]. Additionally, Ansari and Loor (2009) noted that in cities with high humidity and frequent rainfall, such as Rasht, the perception of exhaustion may be intensified, particularly among older individuals with lower resilience to environmental factors [12]. The absence of gender differences in this study contrasts with findings by Dėdelė et al. (2022), who reported that women in Europe experience greater exhaustion due to social roles and lower physical fitness levels [13]. The rejection of the gender difference hypothesis in Rasht may be linked to uniform urban lifestyle pressures on both genders, such as limited opportunities for regular exercise or similar occupational demands. This suggests that while age-related physiological decline is a universal factor, localized factors in Rasht may have homogenized gender experiences, warranting further investigation. In contrast, Pelletier et al. (2021) emphasized that women globally face greater exhaustion barriers due to domestic responsibilities, a pattern not strongly observed in this study. The acceptance of age effects can be attributed to the combined impact of reduced physical capacity and environmental challenges, while the rejection of gender differences highlights the need to consider cultural and lifestyle uniformity in this community [7].
Interpersonal barriers: Lack of family encouragement
Interpersonal barriers, measured by lack of family encouragement, identified as the least significant factor in this study, with no significant gender or age differences. This result rejects both hypotheses regarding the influence of gender and age on interpersonal barriers. This finding contrasts with extensive literature that identifies social support as a facilitator of physical activity. For example, Bantham et al. (2021) found that in developing countries, family support significantly enhances women’s participation, particularly in young and middle adulthood [14]. Similarly, Kamarudin and Omar-Fauzee (200) highlighted the role of family encouragement in collectivist Asian cultures, arguing that social networks reinforce health behaviors [15]. However, the current results align with Mirheidari et al. (2013), who found that in urban areas of Iran, physical activity is often perceived as an individual responsibility rather than a behavior dependent on social support [16]. Salehzadeh et al. (2014) also emphasized that environmental factors often overshadow interpersonal barriers [9]. Conversely, Mathews et al. (2010) observed that in societies with individualistic tendencies or poor physical activity infrastructure, social support becomes less significant, a pattern also observed in Rasht [17]. The rejection of gender and age hypotheses may indicate a cultural shift toward autonomy in health-related decision-making, potentially reinforced by urbanization and modernity, which have diminished the traditional role of family encouragement in physical activity.
Structural barriers: Physical activity environment and time expenditure
Structural barriers, encompassing environmental factors and time constraints, identified as the most significant barriers in this study, with significant gender and age differences. Women reported greater barriers, and these barriers intensified with age, confirming the hypotheses regarding the influence of gender and age. These results are consistent with global studies. For instance, Salmi et al. noted that the lack of sports infrastructure and time constraints is particularly significant barriers for women and older individuals [10]. Additionally, Akpinar et al. (2020) stated that unfavorable environmental conditions, such as adverse weather, lack of equipment, and insufficient facilities, reduce participation in physical activity [18]. Locally, Rasht’s humidity and rainfall pose significant barriers, especially for women and older adults who lack access to indoor spaces. Based on Vafaee et al.’s findings, women in Iran face greater structural barriers due to familial roles and limited access to facilities [6]. The acceptance of the gender hypothesis can be attributed to social inequalities and women’s limited access to sports spaces, while the increase in barriers with age reflects reduced mobility and greater dependence on environmental conditions. This pattern differs from studies in communities with better infrastructure, which report fewer barriers, underscoring the influence of Rasht’s local conditions.
Conclusion
Overall, the results of this study indicate that structural barriers, including environmental factors and time constraints, are the primary obstacles to participation in physical activity in Rasht, while individual barriers such as physical exhaustion intensify with age, and interpersonal barriers like lack of family encouragement are of minor importance. Gender and age differences were confirmed for structural barriers but were limited or absent for individual and interpersonal barriers, respectively. This pattern supports the hypothesis of multi-level influences on physical activity and aligns with the well-established ecological model, which, in recent updates, emphasizes the importance of environmental factors. These findings highlight the need for designing localized and targeted programs to enhance the physical health of citizens. Based on recent scientific evidence, overcoming these barriers will not only increase participation in physical activity but also reduce the burden of chronic diseases and improve quality of life in this city.
Limitations
This study had several limitations. First, the use of self-reported questionnaires may have been subject to response bias. Second, the cross-sectional design did not allow for the examination of changes in barriers over time. Third, the focus on Rasht limits the generalizability of the findings to other cities, particularly given Iran’s climatic and cultural diversity. Future longitudinal and multi-regional studies are recommended.
Ethical Considerations
Compliance with ethical guidelines
This study adhered to ethical principles and received approval from the Ethics Committee of the Sport Sciences Research Institute, Tehran, Iran (Code: SSRI.REC-2309-2449). Participant information was kept confidential and used solely for research purposes. Participants were free to withdraw from the study at any stage.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
Thanks to the Ministry of Sports and Youth of Guilan Province for providing the necessary cooperation with the research team during the research.
References
Physical activity, as a cornerstone of physical and mental health, plays a critical role in preventing chronic diseases and enhancing quality of life. However, in recent decades, modern lifestyles characterized by urbanization, technological advancements, and the mechanization of daily tasks have significantly reduced physical activity levels among individuals. This sedentary behavior, particularly in urban communities, has been associated with an increased prevalence of conditions such as obesity, type 2 diabetes, and cardiovascular diseases, placing a substantial burden on healthcare systems [1]. The World Health Organization (WHO) reports that over 50% of the global population fails to meet the recommended physical activity levels (at least 150 minutes of moderate aerobic activity per week), highlighting the urgent need for targeted interventions to promote an active lifestyle [2]. In Iran, despite a rich sports culture and historical emphasis on well-being, public participation in physical activity remains below global standards [3]. Rasht, the capital of Gilan Province, exemplifies this paradox. Blessed with a favorable climate and a significant history of sporting achievements, the city nonetheless struggles with suboptimal physical activity levels among its residents. Factors such as infrastructural limitations, socio-cultural conditions, and individual differences may explain this situation, yet a thorough understanding of these barriers requires localized investigation.
Previous studies have demonstrated that barriers to physical activity are influenced by variables such as age and gender. For instance, Rasekh et al., in a study on Iranian women, identified limited access to sports facilities, lack of time, and psychological barriers like fear of injury as primary deterrents [4]. Similarly, Geelen et al., in a comprehensive review, reported environmental barriers (e.g. lack of sports spaces), social influences (e.g. insufficient family support), and personal beliefs as key factors affecting participation in physical activity [5]. However, most of these studies have either been conducted broadly or focused on specific groups (e.g. women or the elderly), with limited attention to age and gender differences within a specific urban context. Research also suggests that overcoming barriers to physical activity can lead to sustainable participation patterns. Vafaee-Najar et al., in their study, highlighted that social factors and structural-cultural barriers operate in a staged manner (individual, familial, and environmental), and individuals’ participation in health programs depends on their ability to manage these factors [6]. This perspective underscores the importance of designing localized programs tailored to the specific needs and constraints of each community. Nevertheless, comprehensive data on the barriers to physical activity in Rasht, considering age and gender differences, remain scarce. This research gap necessitates a focused study to identify these barriers accurately and propose contextually appropriate solutions.
The aim of this study is to investigate the barriers to physical health-related physical activity among Rasht citizens, with an emphasis on age and gender differences. The study seeks to address the following questions: What differences exist in the barriers to physical activity across various age groups in Rasht, and what are the primary barriers to physical activity among Rasht citizens based on gender? The findings of this research can assist policymakers and urban planners in designing targeted interventions to enhance public participation in physical activity and improve community health.
Materials and Methods
This study is a descriptive-analytical, cross-sectional research aimed at identifying barriers to physical health-related physical activity among Rasht citizens. A cross-sectional design was chosen due to its ability to examine variables within a specific timeframe and analyze differences based on age and gender [7].
Study population and sampling
The study population comprised all Rasht residents in 2024, aged 18 to 65 years. The sample size was determined using Cochran’s formula, with a 95% confidence level (z=1.96), a 5% margin of error (d=0.05), and an initial estimate of physical activity participation proportion (P=0.5), yielding a minimum sample size of 384 individuals [8]. Accounting for a 10% dropout rate, the final sample size was increased to 422 participants. Multi-stage cluster sampling was employed. The study population consisted of households covered by Rasht’s comprehensive health centers in 2024, selected as representatives of the city’s urban population. Rasht was divided into five geographical regions, and using the multi-stage cluster sampling method, three regions (60% of the total) were randomly selected in the first stage. Within each region, households were visited in person, and one eligible individual (aged 18–65 and a permanent Rasht resident) per household was chosen as the primary respondent. Selection within each household was conducted via simple random sampling (using a lottery method by the researchers) among eligible individuals. After excluding incomplete data, the final analysis included 408 participants (204 men and 204 women). Inclusion criteria included residency in Rasht for at least one year, the ability to complete the questionnaire, and informed consent to participate. Individuals with severe physical or mental conditions that hindered their ability to respond were excluded.
Research instruments
Data were collected using two primary tools:
Demographic questionnaire
This self-reported questionnaire included variables such as age, gender, marital status, education level, occupation, and monthly income.
Physical activity barriers questionnaire
The primary tool was the exercise benefits/barriers scale (EBBS), designed and developed by Ortenberg et al. (1990). The barriers section comprises 14 questions categorized into the following subscales to identify individual, interpersonal, and structural barriers:
Physical activity environment: 6 questions, score range 6–24 (each question scored 1–4);
Time expenditure: 3 questions, score range 3–12;
Physical exhaustion: 3 questions, score range 3–12;
Lack of family encouragement: 2 questions, score range 2–8.
The total score ranges from 14 to 56, indicating the level of barriers from low to high. The convergent construct validity and internal consistency reliability of this tool were confirmed by Ortenberg et al. (1990) with a Cronbach’s α of 87% [8]. In Iran, Salehzade et alvalidated its convergent construct validity and internal consistency reliability with a similar Cronbach’s α [9].
Data collection method
Data were gathered through in-person interviews at participants’ homes or in open spaces, with questionnaires completed by trained researchers. Prior to the study, the research objectives were explained to participants, and written informed consent was obtained. To ensure data quality, completed questionnaires were reviewed, and incomplete or ambiguous responses were clarified with participants. Data collection occurred over a three-month period.
Data analysis
Data were analyzed using SPSS software, version 26. Descriptive statistics (Mean±SD, frequency, and percentage) were used to describe demographic characteristics and physical activity barriers. Normality of data distribution was assessed using the Shapiro-Wilk test prior to parametric analyses, confirming normal distribution (P>0.05). To examine differences in barriers across age and gender groups, independent t-tests (for gender comparisons) and one-way analysis of variance (ANOVA) (for age group comparisons) were applied. Post-hoc Tukey tests were conducted for pairwise comparisons when ANOVA results indicated significant differences. The significance level for all analyses was set at 0.05.
Results
Demographic characteristics of participants
In this study, 422 citizens of Rasht participated; however, after excluding incomplete data, the information from 408 individuals (96.7%) was used for the final analysis. Of these, 204 participants (50%) were female, and 204 (50%) were male. The participants were divided into four age groups: 18–30 years (30.4%, n=124), 31–40 years (28.2%, n=115), 41–50 years (22.8%, n=93), and 51–65 years (18.6%, n=76) (Table 1).
Frequency of study items
As observed in Table 2, the frequency of participants’ responses to the study questions is presented. The highest mean score was related to the high cost of exercise followed by distance from sports venues.
Based on the results of Table 3, the overall mean score of barriers to physical activity, as measured by the EBBS scale (range: 14–56), was 32.4±8.5, indicating a moderate level of barriers among participants. The analysis revealed that the mean score for women (34.1±8.8) was significantly higher than that for men (30.8±8.2) (t406=3.41, P=0.001). Additionally, a significant difference was observed across age groups (F3, 404=8.76, P<0.001). Post-hoc Tukey tests indicated that the 51–65 age group reported significantly more barriers compared to the 18–30 age group (P<0.001). In the “physical activity environment” subscale, the independent t-test revealed a significant difference between men and women (t406=2.58, P=0.01), indicating that women perceived greater environmental barriers. The highest mean score was recorded among women in the 51–65 age group. Analysis of variance (ANOVA) also confirmed a significant difference across age groups (F3, 404=3.45, P=0.02), and the post-hoc Tukey test showed a significant difference between the 18–30 and 51–65 age groups (P<0.001), suggesting that environmental barriers increase with age.
In the “time expenditure” subscale, the independent t-test indicated a significant difference between men and women (t406=2.03, P=0.04), highlighting greater time constraints among women, particularly in the 41–50 age group. However, ANOVA results showed no significant difference across age groups (F3, 404=1.12, P=0.34), as the overall mean scores were similar across all age groups.
In the “physical exhaustion” subscale, the independent t-test showed no significant difference between men and women (t406=1.12, P=0.26), although women in the 51–65 age group had the highest mean score. ANOVA results confirmed a significant difference across age groups (F3, 404=10.23, P<0.001), and the Tukey test identified a significant difference between the 18–30 and 51–65 age groups (P<0.001), indicating that physical exhaustion increases with age.
In the “lack of family encouragement” subscale, the independent t-test revealed no significant difference between men and women (t406=0.89, P=0.37). Similarly, ANOVA results showed no significant difference across age groups (F3, 404=1.45, P=0.23), as the overall mean scores were low across all groups, suggesting that this barrier is of minor importance.
Gender and age differences in physical activity barrier factors
The results of comparing the mean scores of barrier factors based on gender and age groups are presented in Table 4.
The independent t-test analysis showed that women had significantly higher scores in the “physical activity environment” (Mean±SD=10.2±2.1) and “lack of family encouragement” (Mean±SD=5.1±1.3) subscales compared to men (Mean±SD=9.1±2.0 and 4.3±1.2, respectively) (P<0.01). However, no significant difference was observed in the “lack of facilities and equipment” subscale (P=0.15). In the ANOVA analysis, the 51–65 age group had significantly higher scores across all subscales compared to the 18–30 age group (P<0.05).
Individual barriers (physical exhaustion)
The independent t-test results indicated no significant difference between men (Mean±SD=7.3±2.6) and women (Mean±SD=7.7±2.7) in physical exhaustion (t406=1.12, P=0.26). However, women in the 51–65 age group reported the highest mean score. One-way analysis of variance (ANOVA) confirmed a significant difference across age groups (F3, 404=10.23, P<0.001), and the post-hoc Tukey test revealed a statistically significant difference between the 18–30 age group (mean=6.3) and the 51–65 age group (mean=9.1) (P<0.001). This finding suggests that the intensity of physical exhaustion increases with age.
Interpersonal barriers (lack of family encouragement)
The independent t-test showed no significant difference between men (Mean±SD=4.0±1.8) and women (Mean±SD=4.2±1.9) in lack of family encouragement (t406=0.89, P=0.37). Similarly, ANOVA revealed no significant difference across age groups (F3, 404=1.45, P=0.23). These results indicate that the lack of family encouragement was of minor importance in this study.
Structural barriers (physical activity environment + time expenditure)
The independent t-test confirmed a significant difference between men (Mean±SD=22.6±6.3) and women (Mean±SD=24.7±6.7) in structural barriers (t406=2.75, P=0.006), with women reporting greater structural barriers, peaking in the 51–65 age group with a mean of 25.8. ANOVA also showed a significant difference across age groups (F3, 404=2.95, P=0.03), and the post-hoc Tukey test identified a significant difference between the 18–30 age group (mean=22.3) and the 51–65 age group (mean=24.7) (P=0.02). These findings highlight the greater impact of structural barriers with increasing age.
Discussion
The primary aim of this study was to investigate the barriers to participation in physical activity related to physical health among Rasht citizens, with a focus on analyzing gender and age differences. The results revealed that barriers to physical activity can be categorized into three main domains: Individual barriers (physical exhaustion), interpersonal barriers (lack of family encouragement), and structural barriers (environmental factors and time constraints). These findings align with contemporary ecological frameworks while highlighting the unique characteristics of the Rasht community.
Individual barriers: Physical exhaustion
The analysis indicated that physical exhaustion, as an individual barrier, significantly intensifies with age, particularly among older individuals, while no significant gender differences were observed. This finding supports the hypothesis that age influences individual barriers but rejects the hypothesis of gender differences in this domain. The greater intensity of exhaustion in older age groups, especially among older women, aligns with recent global evidence. For instance, Salmi et al. found that barriers to physical activity in adults include factors such as low mood, lack of time, health problems, and a lack of companionship… These barriers are particularly pronounced in individuals with a non-native language, single parents, those aged 30-44 years, and those with low household incomes. These barriers are particularly pronounced in individuals with a non-native language, single parents, those aged 30-44 years, and those with low household incomes [10]. Similarly, Uddin et al. (2018) argued that the subjective experience of exhaustion in older adults is tied to physiological changes, reducing their inclination toward physical activity [11]. Additionally, Ansari and Loor (2009) noted that in cities with high humidity and frequent rainfall, such as Rasht, the perception of exhaustion may be intensified, particularly among older individuals with lower resilience to environmental factors [12]. The absence of gender differences in this study contrasts with findings by Dėdelė et al. (2022), who reported that women in Europe experience greater exhaustion due to social roles and lower physical fitness levels [13]. The rejection of the gender difference hypothesis in Rasht may be linked to uniform urban lifestyle pressures on both genders, such as limited opportunities for regular exercise or similar occupational demands. This suggests that while age-related physiological decline is a universal factor, localized factors in Rasht may have homogenized gender experiences, warranting further investigation. In contrast, Pelletier et al. (2021) emphasized that women globally face greater exhaustion barriers due to domestic responsibilities, a pattern not strongly observed in this study. The acceptance of age effects can be attributed to the combined impact of reduced physical capacity and environmental challenges, while the rejection of gender differences highlights the need to consider cultural and lifestyle uniformity in this community [7].
Interpersonal barriers: Lack of family encouragement
Interpersonal barriers, measured by lack of family encouragement, identified as the least significant factor in this study, with no significant gender or age differences. This result rejects both hypotheses regarding the influence of gender and age on interpersonal barriers. This finding contrasts with extensive literature that identifies social support as a facilitator of physical activity. For example, Bantham et al. (2021) found that in developing countries, family support significantly enhances women’s participation, particularly in young and middle adulthood [14]. Similarly, Kamarudin and Omar-Fauzee (200) highlighted the role of family encouragement in collectivist Asian cultures, arguing that social networks reinforce health behaviors [15]. However, the current results align with Mirheidari et al. (2013), who found that in urban areas of Iran, physical activity is often perceived as an individual responsibility rather than a behavior dependent on social support [16]. Salehzadeh et al. (2014) also emphasized that environmental factors often overshadow interpersonal barriers [9]. Conversely, Mathews et al. (2010) observed that in societies with individualistic tendencies or poor physical activity infrastructure, social support becomes less significant, a pattern also observed in Rasht [17]. The rejection of gender and age hypotheses may indicate a cultural shift toward autonomy in health-related decision-making, potentially reinforced by urbanization and modernity, which have diminished the traditional role of family encouragement in physical activity.
Structural barriers: Physical activity environment and time expenditure
Structural barriers, encompassing environmental factors and time constraints, identified as the most significant barriers in this study, with significant gender and age differences. Women reported greater barriers, and these barriers intensified with age, confirming the hypotheses regarding the influence of gender and age. These results are consistent with global studies. For instance, Salmi et al. noted that the lack of sports infrastructure and time constraints is particularly significant barriers for women and older individuals [10]. Additionally, Akpinar et al. (2020) stated that unfavorable environmental conditions, such as adverse weather, lack of equipment, and insufficient facilities, reduce participation in physical activity [18]. Locally, Rasht’s humidity and rainfall pose significant barriers, especially for women and older adults who lack access to indoor spaces. Based on Vafaee et al.’s findings, women in Iran face greater structural barriers due to familial roles and limited access to facilities [6]. The acceptance of the gender hypothesis can be attributed to social inequalities and women’s limited access to sports spaces, while the increase in barriers with age reflects reduced mobility and greater dependence on environmental conditions. This pattern differs from studies in communities with better infrastructure, which report fewer barriers, underscoring the influence of Rasht’s local conditions.
Conclusion
Overall, the results of this study indicate that structural barriers, including environmental factors and time constraints, are the primary obstacles to participation in physical activity in Rasht, while individual barriers such as physical exhaustion intensify with age, and interpersonal barriers like lack of family encouragement are of minor importance. Gender and age differences were confirmed for structural barriers but were limited or absent for individual and interpersonal barriers, respectively. This pattern supports the hypothesis of multi-level influences on physical activity and aligns with the well-established ecological model, which, in recent updates, emphasizes the importance of environmental factors. These findings highlight the need for designing localized and targeted programs to enhance the physical health of citizens. Based on recent scientific evidence, overcoming these barriers will not only increase participation in physical activity but also reduce the burden of chronic diseases and improve quality of life in this city.
Limitations
This study had several limitations. First, the use of self-reported questionnaires may have been subject to response bias. Second, the cross-sectional design did not allow for the examination of changes in barriers over time. Third, the focus on Rasht limits the generalizability of the findings to other cities, particularly given Iran’s climatic and cultural diversity. Future longitudinal and multi-regional studies are recommended.
Ethical Considerations
Compliance with ethical guidelines
This study adhered to ethical principles and received approval from the Ethics Committee of the Sport Sciences Research Institute, Tehran, Iran (Code: SSRI.REC-2309-2449). Participant information was kept confidential and used solely for research purposes. Participants were free to withdraw from the study at any stage.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
Thanks to the Ministry of Sports and Youth of Guilan Province for providing the necessary cooperation with the research team during the research.
References
- Mirza Rah Kooshki MH, Zarei A, Khodayari A. Designing health development strategies with a physical and sport activities approach. Sport Manage J. 2019; 11(4):787-807. [DOI:10.22059/jsm.2019.262121.2117]
- Jackson EL, Crawford DW, Godbey G. Negotiation of leisure constraints. Leisure Sci. 1993; 15(1):1.[DOI:10.1080/01490409309513182]
- Mohammad Kazemi R, Ajorloo F, Ghadimi B. [Identifying and develop a model of practical contextual factors for the position of women’s sports in improving development indicators (Prsian)]. Cult Soc Stud Olympic. 2020; 1(2):67-82. [Link]
- Rasekh N, Zareian H, Ghasemi H, Rezaie Z. Championship sports for Iranian women: Challenges, opportunities and solutions. New Approaches Exerc Physiol. 2019; 1(1):99-116. [DOI:10.22054/nass.2018.9861]
- Geelen SJ, van Dijk-Huisman HC, de Bie RA, Veenhof C, Engelbert R, van der Schaaf M, et al. Barriers and enablers to physical activity in patients during hospital stay: A scoping review. Syst Rev. 2021; 10(1):1-3. [DOI:10.1186/s13643-021-01843-x]
- Vafaee-Najar A, Ebrahimipour H, Behzad F, Tehrani H. [Relationship of Perceived Benefits and Perceived Barriers with Regular Physical Activity among Employees of Mashhad University of Medical Sciences (Persian)]. Iran J Health Educ Health Promot. 2017; 5 (1):58-64. [DOI:10.18869/acadpub.ihepsaj.5.1.58]
- Pelletier CA, White N, Duchesne A, Sluggett L. Barriers to physical activity for adults in rural and urban Canada: A cross-sectional comparison. SSM Popul Health. 2021; 16:100964. [DOI:10.1016/j.ssmph.2021.100964] [PMID]
- Ortabag T, Ceylan S, Akyuz A, Bebis H. The validity and reliability of the exercise benefits/barriers scale for Turkish Military nursing students. Afr J Res Sport Phys Educ Recreat. 2010; 32(2):55-70. [DOI:10.4314/sajrs.v32i2.59297]
- Salehzade K, Zamani Sani SH, Fathi Rezaie Z. [Validity and reliability of exercise benefits/barriers scale in Iranian elderly (Persian)]. Welfare Rehab Sci Univ. 2011; 3(1):1-16. [Link]
- Salmi L, Hasanen E, Simula M, Virmasalo I, Muukkonen P. Perceived barriers to physical activity in the social spaces of low socioeconomic status suburbs. Wellbeing Space Soc. 2023; 5:100164. [DOI:10.1016/j.wss.2023.100164]
- Uddin R, Burton NW, Khan A. Perceived environmental barriers to physical activity in young adults in Dhaka City, Bangladesh-does gender matter? Int Health. 2018; 10(1):40-6. [DOI:10.1093/inthealth/ihx057] [PMID]
- El Ansari W, Lovell G. Barriers to exercise in younger and older non-exercising adult women: A cross sectional study in London, United Kingdom. Int J Environ Res Public Health. 2009; 6(4):1443-55. [DOI:10.3390/ijerph6041443] [PMID]
- Dėdelė A, Chebotarova Y, Miškinytė A. Motivations and barriers towards optimal physical activity level: A community-based assessment of 28 EU countries. Prev Med. 2022; 164:107336. [DOI:10.1016/j.ypmed.2022.107336] [PMID]
- Bantham A, Taverno Ross SE, Sebastião E, Hall G. Overcoming barriers to physical activity in underserved populations. Prog Cardiovasc Dis. 2021; 64:64-71. [DOI:10.1016/j.pcad.2020.11.002] [PMID]
- Kamarudin K, Omar-Fauzee MS. Attitudes toward physical activities among college students. Pak J Psychol Res. 2007; 22(1):43-54. [Link]
- Mirheidari L, Bashiri M. [Leisure time physical activities and their relationship with demographic characteristics of the people of Tabriz (Persian)]. Physiol Manage Res Sports. 2013; 13:75-92. [Link]
- Mathews AE, Laditka SB, Laditka JN, Wilcox S, Corwin SJ, Liu R, et al. Older adults' perceived physical activity enablers and barriers: A multicultural perspective. J Aging Phys Act. 2010; 18(2):119-40. [DOI:10.1123/japa.18.2.119] [PMID]
- Akpınar, A. (2020). Investigating the barriers preventing adolescents from physical activities in urban green spaces. Urban For Urban Green. 53:126724. [DOI:10.1016/j.ufug.2020.126724]
Article Type: Original Contributions |
Subject:
Health Education and Promotion
Received: 2025/01/15 | Accepted: 2025/02/20 | Published: 2025/04/21
Received: 2025/01/15 | Accepted: 2025/02/20 | Published: 2025/04/21
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
