

Volume 10, Issue 4 (10-2025)
CJHR 2025, 10(4): 237-246 |
Back to browse issues page


Ethics code: IR.SCU.REC.1404.035
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hashemi A, saadatian A, Siavashi E, Abedanzadeh R. Virtual Physical Activity as An Intervention for Behavioral Regulation in Children With Attention Deficit Hyperactivity Disorder. CJHR 2025; 10 (4) :237-246
URL: http://cjhr.gums.ac.ir/article-1-428-en.html
URL: http://cjhr.gums.ac.ir/article-1-428-en.html


1- Department of Sport Sciences, Faculty of Literature and Humanities, Yasuj University, Yasuj, Iran , a.hashemi@yu.ac.ir
2- Department of Sport Sciences, Faculty of Literature and Humanities, Yasuj University, Yasuj, Iran
3- Department of Sport Sciences, Faculty of Sport Sciences, Shahid Chamran University of Ahvaz, Ahvaz, Iran
2- Department of Sport Sciences, Faculty of Literature and Humanities, Yasuj University, Yasuj, Iran
3- Department of Sport Sciences, Faculty of Sport Sciences, Shahid Chamran University of Ahvaz, Ahvaz, Iran
Keywords: Attention-deficit/hyperactivity disorder (ADHD), Digitally mediated physical activity (PA), Behavioral performance indicators, Neurodevelopmental disorders
Full-Text [PDF 570 kb]
(76 Downloads)
| Abstract (HTML) (512 Views)
Full-Text: (95 Views)
Introduction
Attention deficit hyperactivity disorder (ADHD) is a common neurodevelopmental disorder, affecting approximately 5% of children and adolescents globally [1, 2]. It is marked by persistent inattention, hyperactivity, and impulsivity, which significantly impair academic performance, behavioral regulation, and social functioning [1, 3]. While physical activity (PA) is widely recognized for its cardiovascular, motor and obesity-related benefits [4, 5] , it has also shown promise in supporting neurocognitive function, behavioral control, and overall quality of life in children with ADHD [6-8]. Recent meta-analyses provide compelling support for PA as an effective intervention for ADHD. For instance, Ye et al. [9] and Zhu et al. [8] found medium to large effect sizes for PA interventions in improving executive function, attention, and hyperactivity symptoms in children with ADHD. Moreover, skill-based PA programs—which emphasize coordination, planning, and cognitive engagement—have been shown to produce stronger cognitive benefits than general physical activities [5]. Despite these positive outcomes, traditional PA formats may fail to sustain the attention or interest of children with ADHD, which impacts adherence [5]. Additionally, standard ADHD treatments—such as pharmacotherapy and behavioral therapy—can be burdensome or carry undesirable side effects [10, 11]. These challenges highlight the need for alternative, engaging approaches. One promising avenue is virtual PA (VPA), which blends exercise with interactive technologies to create immersive and adaptive experiences [12, 13]. VPA environments can be tailored to individual needs, accounting for the impulsivity, distractibility, and executive function deficits often present in ADHD. These digital tools can increase engagement and program adherence by offering gamified, feedback-rich, and personally meaningful experiences [14, 15]. However, the literature on the specific effects of VPA on behavioral outcomes in ADHD is still limited. While general benefits of PA are well-documented, few studies directly compare traditional and virtual formats in ADHD populations [16, 17]. Given the complexity of ADHD and its comorbid challenges such as anxiety, depression, and conduct problems, investigating VPA as a targeted intervention is both timely and necessary [9, 18]. The purpose of this study is to evaluate critically how well VPA training to improve behavioral outcomes in children with ADHD. By addressing these research gaps, this study attempts to explore the role of VPA as a practical and useful intervention for managing ADHD symptoms in limited settings. Therefore, we hypothesize that: Children with ADHD participating in a structured VPA program will show significant improvements in behavioral outcomes as measured by the CBCL compared to those in control groups not engaged in such activities. From a societal perspective, the findings of this study have the potential to influence public health policies and educational strategies. Given the high costs of ADHD treatment and the societal burden of managing this disorder, identifying effective and accessible interventions is of paramount importance. Furthermore, the results of this study can provide valuable guidance for educational institutions, healthcare providers, and parents to support children with ADHD to achieve their full potential and provide a framework for future research on the long-term benefits of VPA in the management of ADHD in different settings.
Materials and Methods
Research design
A semi-experimental design was used in this study, and comparison groups participated in pre-, post-, and follow-up assessments. In order to reduce baseline differences between groups, participants were matched on important variables like age, ADHD subtype, and presence of comorbidities after being chosen based on predetermined eligibility criteria. Following the matching process, participants were randomly assigned to one of two groups: The experimental group, which received the VPA intervention, and the control group, which did not receive any intervention but was assessed at the same three time points. Additionally, a third group of usually developing children, designated as the HC group, was added to examine if children with ADHD might obtain equivalent behavioral outcomes following the intervention. Sample size calculations were conducted using G*Power software, version 3.1.9.2, based on a significance level of 5%, an effect size of 0.3, and a statistical power of 80%. The analysis indicated that a minimum of 50 participants would be necessary. To account for potential attrition, the total sample size was increased to 80 participants (40 in each group).
Participants and procedure
The study involved boys aged 7–10 years enrolled in elementary schools in Shiraz, Iran (2025). The focus on boys reflected national regulations requiring male teachers for male students. Inclusion criteria were as follows: 1) age between 7 and 10 years; 2) a clinical diagnosis of ADHD confirmed by a child psychiatrist or developmental psychologist, along with results from the Conner’s parents ratting scale (CPRS) (1979); 3) a formal recommendation from a healthcare provider for participation in the study; and 4) an IQ>80, as measured by the Wechsler intelligence scale for children–fourth edition [19]. Sampling followed a multi-stage design. First, 10 schools were randomly chosen from 40 public boys’ schools. Next, 800 Conners’ parent rating scale (CPRS) (1979) [20] questionnaires were distributed to parents and teachers; 580 were returned. Based on the questionnaires’ scores and follow-up clinical evaluations, 86 children met the inclusion criteria. After six withdrew, 80 children comprised the final ADHD sample. This final step was purposive, guided by predefined eligibility and exclusion criteria. To balance baseline characteristics, participants were matched on age, ADHD subtype, and comorbid conditions. They were then randomly assigned to either the experimental group (VPA) or the control group (no intervention), with 40 children in each. A separate healthy control (HC) group of 40 typically developing (TD) children was randomly recruited from two other schools. Their typical development was confirmed by psychiatric evaluation. Behavioral assessments were conducted at three time points: One week before the intervention (baseline), immediately after the 12-week program (post-test), and 12 weeks later (follow-up). Each session lasted about 60 minutes.
Intervention
Following the pre-test, the experimental group (40 children with ADHD) participated in the designed program for 12 weeks through online sessions, while the control group (40 children with ADHD) continued their daily routines without engaging in any structured PA program or receiving specific medical treatments. The intervention was developed based on established principles of physical education for children [21] and designed using the FITT framework (frequency, intensity, time, and type). The experimental group received the program twice weekly (Saturdays and Tuesdays) for 60 minutes per session. Each session consisted of a 5-minute class preparation, 5 minutes of warm-up, 45 minutes of main exercises, and 5 minutes of cool-down, with warm-up and cool-down delivered in the form of movement-based games. The 45-minute core component was divided into three 15-minute segments, each focusing on a fundamental motor skill domain: Locomotor, manipulative, and stability skills. Activity design was based on movement concepts (body awareness, spatial awareness, movement quality, and relationships), and the level of challenge was adjusted accordingly. Equipment included commonly available items such as hula hoops, cones, and balls, supplemented by household materials. Sessions were delivered via the Zoom videoconferencing platform, allowing real-time interaction between instructors and participants. Children were required to keep their cameras on so that instructors could continuously monitor performance. In addition, a parent was present during each session to provide assistance and ensure safe participation. To monitor adherence and quality of engagement, instructors used standardized checklists for attendance and task performance, and session reports were documented after each class. The program was led by experienced physical education instructors, in collaboration with the study authors, following a pre-established lesson plan.
Measures
Three time points were used to evaluate behavioral disorder indicators: Before the intervention (time 1), just after the 12-week intervention period (time 2), and at a 12-week follow-up (time 3). To reduce bias, all evaluations were carried out by qualified research personnel who were blind to group assignment. Standardized measurement training and comprehensive protocol instructions covering the administration of all evaluations were provided to the research team in order to guarantee data consistency and reliability. To ensure procedural fidelity, a senior researcher oversaw each testing session. Participants were instructed to adhere to consistent dietary practices on the main testing days and were allowed to consume only distilled water prior to testing to reduce confounding variables.
Conner’s parents ratting scale–revised short form (CPRS- R)
The parent form of the Conners questionnaire was developed by Conners et al. to assess behavioral problems associated with ADHD. The short form of this scale was presented in 1997 by Conners et al. This form has 27 questions in four subscales: Cognitive (inattention deficit; 6 questions), hyperactivity (6 questions), oppositional defiant (6 questions), and index (9 questions), and parents rate the extent and severity of each behavior on a four-point scale, from 0 (not at all true, never or rarely) to 3 (completely true, most of the time or almost always) [22]. Considering the number of questions, the total score of the questionnare ranges from 27 to 108. Obtaining a score of 1.5 or more for any question indicates the presence of ADHD. Cronbach’s α coefficient in these scales has been reported to be 0.91 to 0.93 [23]. the Persian version of CPRS used in this study has been validated for use with Iranian children. Shahim et al. reported strong internal consistency (Cronbach’s α ranging from 0.71 to 0.86) and appropriate construct validity, supporting its use in Iranian clinical settings [24]. It should be noted that this questionnaire was used only as a diagnostic tool and inclusion criterion in the study and was not used in the evaluation of outcomes.
Parent reports of child behavior (CBCL)
Child behavior was assessed using the child behavior checklist, a 113-item parent-report measure rated on a 3-point Likert scale (0=not true, 1=somewhat true, 2=very true) [25]. The CBCL yields scores on eight syndrome subscales: Anxiety/depression (14 items; 0–28), withdrawn (8 items; 0–16), somatic complaints (11 items; 0–22), social problems (11 items; 0–22), thinking problems (15 items; 0–30), attention problems (10 items; 0–20), delinquent behavior (17 items; 0–34), and aggressive behavior (18 items; 0–36). Two broadband dimensions are derived: Internalizing problems (0–66) and externalizing problems (0–70), as well as a total problems score (0–226). T-scores <65 indicate the non-clinical range, 65–69 borderline, and ≥70 clinical. The validity of this test is 0.98 and its reliability is 0.84 [26].The Persian version of the CBCL has been validated by Yazdkhasti & Oreyzi, demonstrating excellent reliability (Cronbach’s α >0.85) and strong convergent validity, making it a culturally appropriate tool for behavioral assessment in Iranian children [27].
Statistical analysis
SPSS software, version 23, was used for all statistical analyses, and P<0.01 was chosen as the significance level. To compare groups, demographic factors such as age, height, weight, body mass index (BMI), and IQ were examined using independent t-tests. Indicators of behavioral disorders, such as anxiety/depression, withdrawn, physical complaints, social problems, cognitive issues, attention issues, delinquent behavior, and violent behavior, were among the dependent variables examined in this study. To assess the effects of the intervention, a series of combined two-way variance analysis (3 [times]×3 [groups]) with repeated measurement applied for behavioral disorders outcomes. If any interaction was considered significant, simple main effects were determined. Effect sizes were reported using η² (eta squared) for analyses of variance (ANOVA), providing an estimate of the proportion of variance explained by the independent variable. For paired t-tests, Cohen’s d was calculated to assess the magnitude of within-group changes over time. Paired t-tests were employed specifically to evaluate the potential maintenance effects of the intervention across different time points. The presuppositions of variance analysis test with repeated measurement (normality, homogeneity, homogeneity of regression slopes, linearity and Mauchly’s sphericity) were checked and confirmed before data analysis.
Results
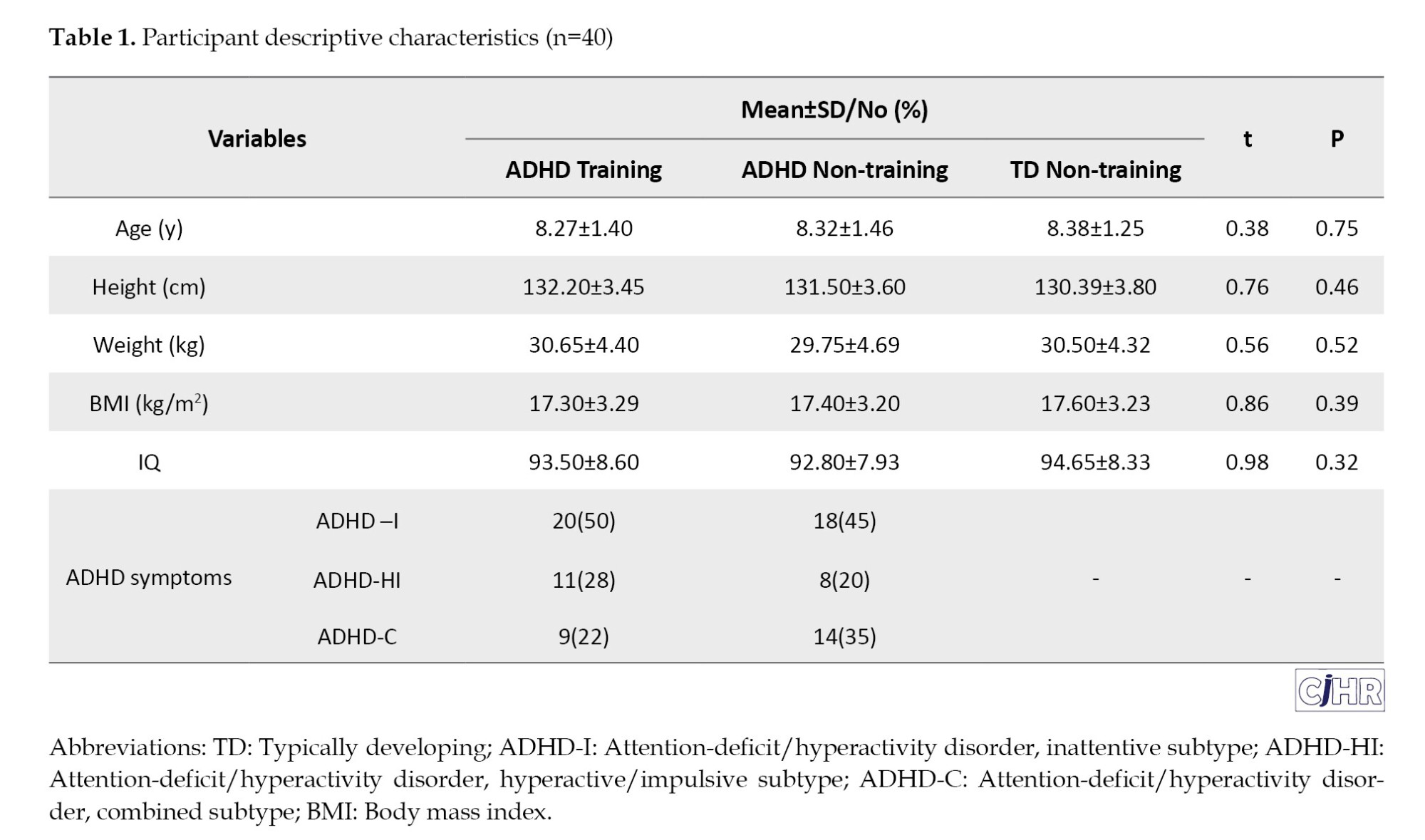
There were no significant differences between the groups on demographic variables at baseline, including age, height, weight, BMI, and IQ (Table 1), indicating successful matching and randomization. It is worth mentioning that one child dropped out of the ADHD training group at time 1. Also, at Time 3, one child from the ADHD training group and 9 children from the ADHD non training group withdrew and did not participate in the research. To check the level of PA (intervention), heart rate and exercise duration were measured. The average duration of training in each session was 53.20±2.80 minutes and the training intensity was 80 heart beats, which indicates moderate to intense PA.
Group comparability
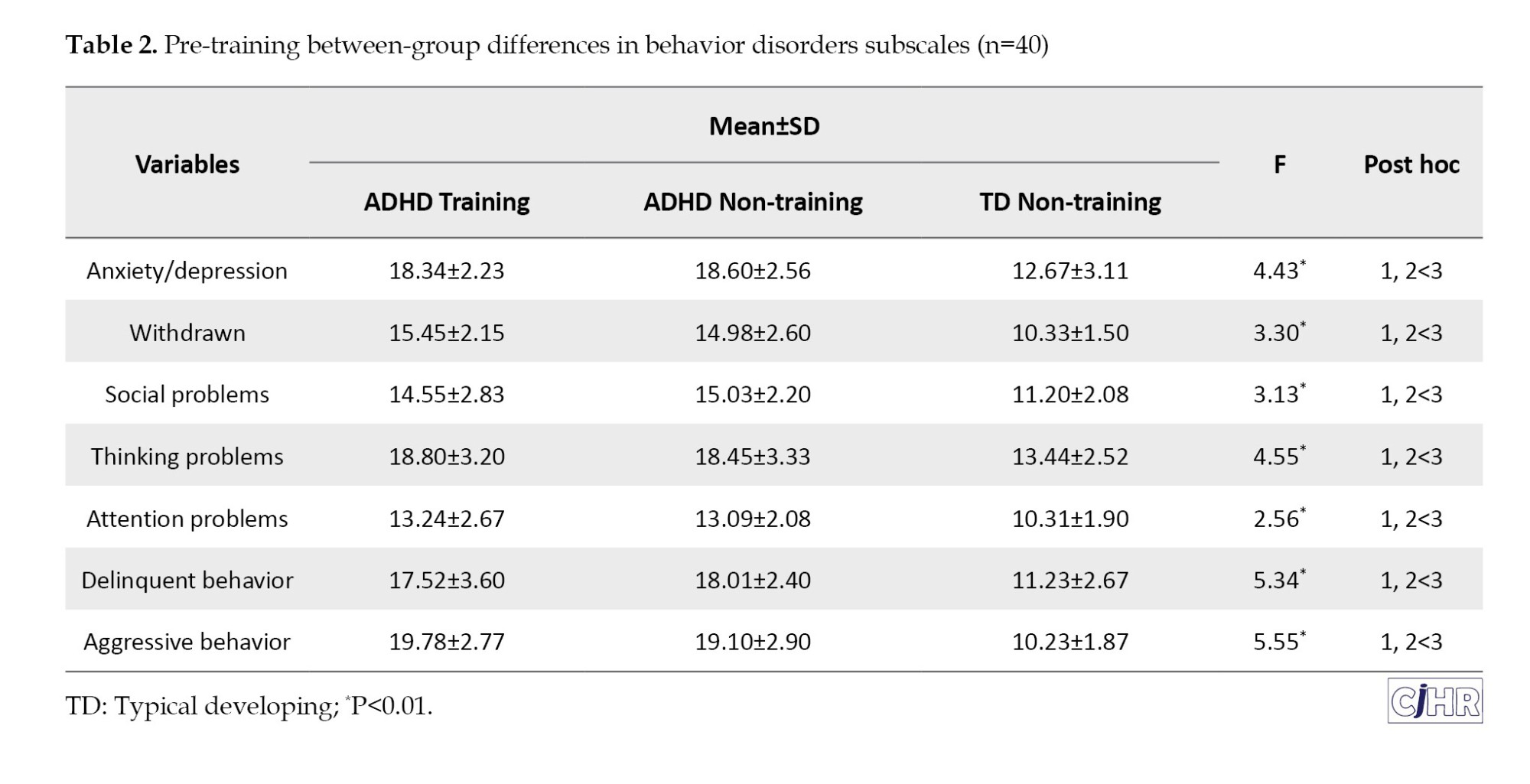
Pre training: Table 2 displays the results according to the behavioral disorders subscales. The behavioral disorder subscales, which include anxiety/depression, withdrawn, social problems, thought problems, attention problems, delinquent behavior, and violent behavior, showed significant group differences, according to the results. Both ADHD subgroups significantly underperformed the normally developing (TD) group on all behavioral problem subscales, according to post hoc pairwise comparisons. But there was no significant difference between two ADHD subgroups.
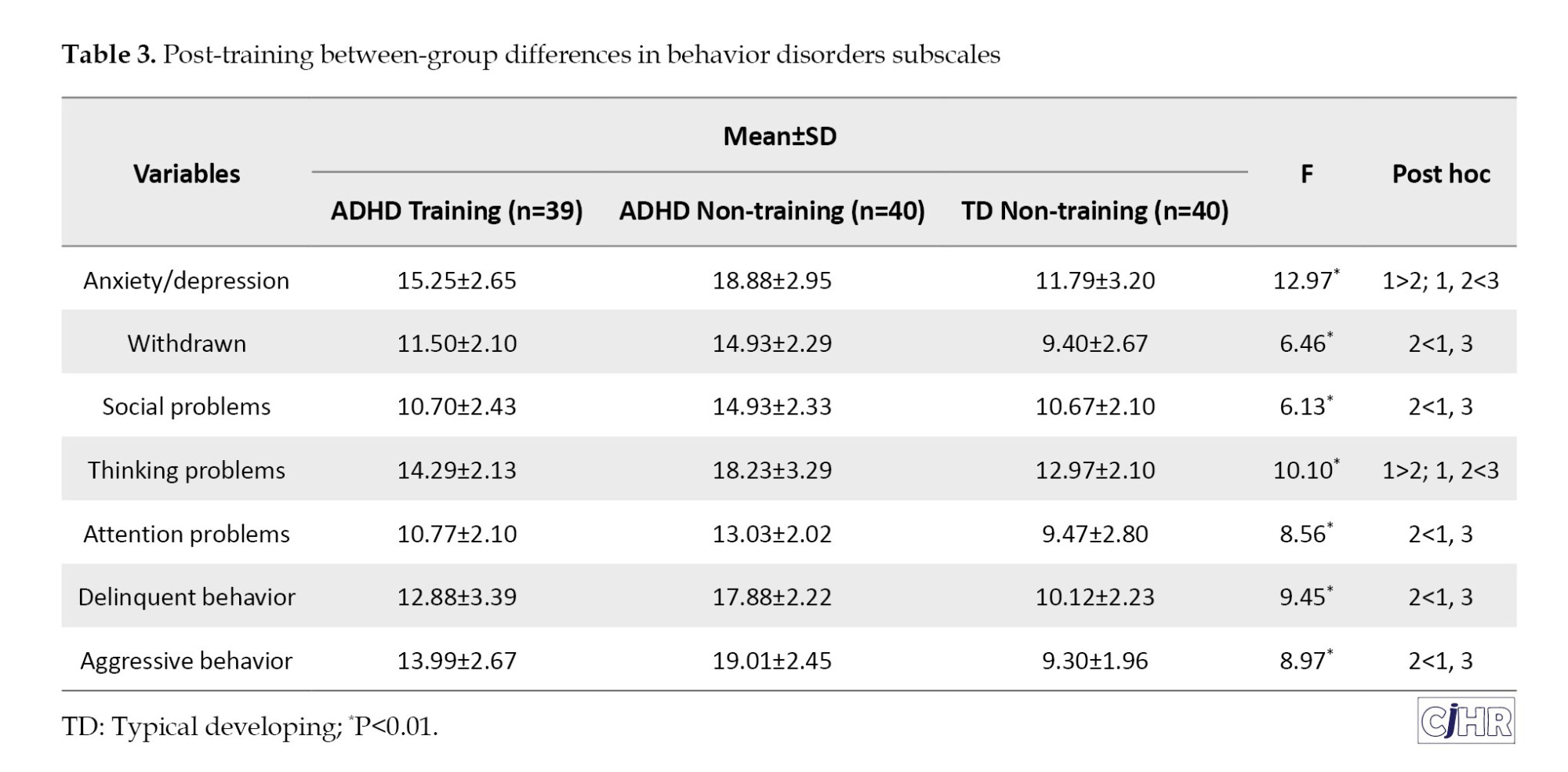
Post training: The outcomes of the post-training behavioral disorders’ subscales are compiled in Table 3. Significant group differences were seen in a number of behavioral disorder subscales after adjusting for pre-training differences. In particular, both ADHD groups outperformed the TD group on post-training scores for anxiety/depression (partial η²=0.47) and thinking problems (partial η²=0.43), with the ADHD non-training group performing noticeably worse than the ADHD training group. Significant differences were also observed in the following areas: Attention issues (partial η²=0.36), delinquent conduct (partial η²=0.41), withdrawn (partial η²=0.25), social problems (partial η²=0.23), and violent behavior (partial η²=0.38). In these subscales, the ADHD non-training group demonstrated worse performance compared to the TD group.
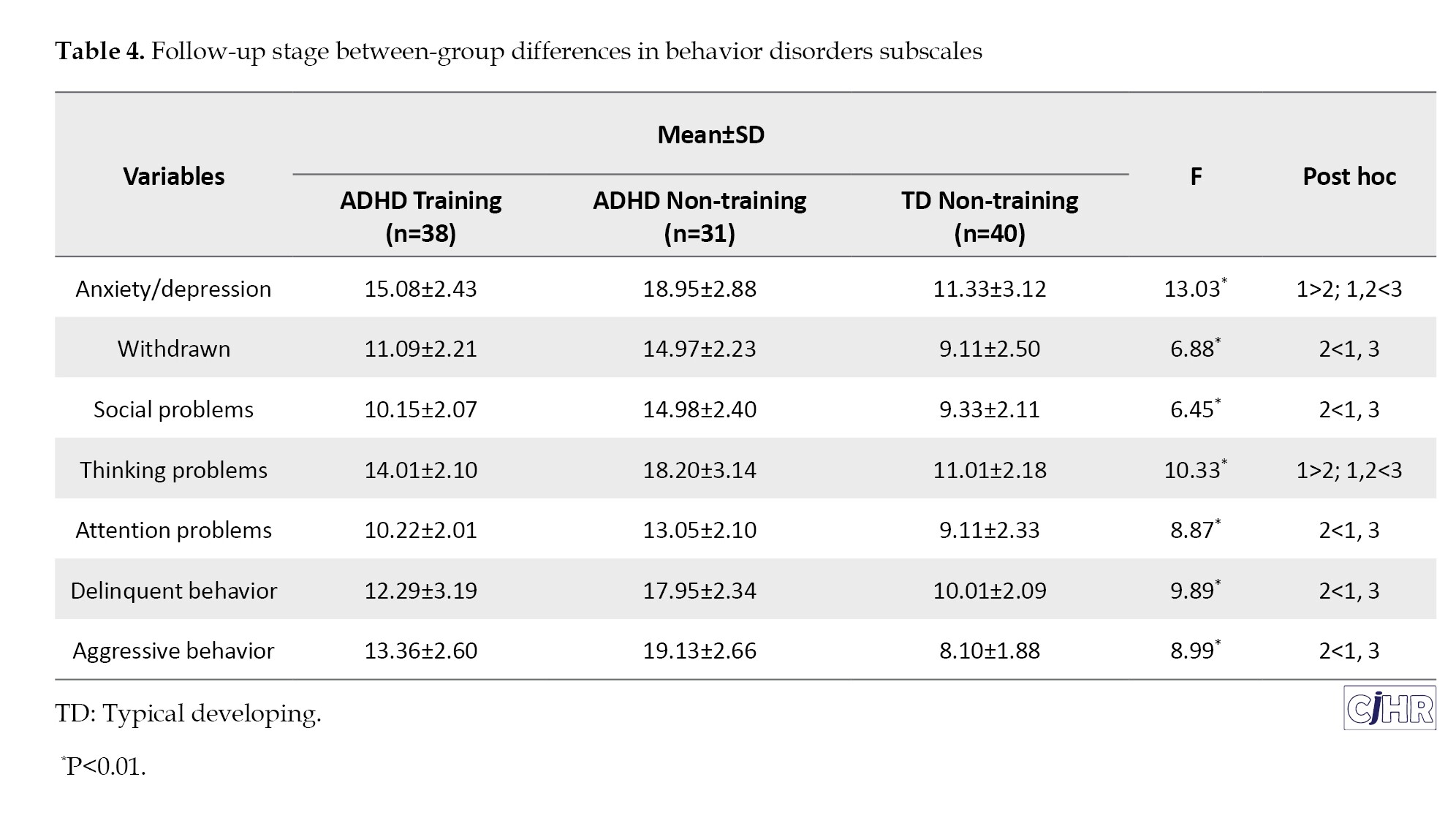
Follow-up stage: The outcomes of the behavioral disorders subscales’ follow-up training are compiled in Table 4. The results showed significant group differences in the post-training anxiety/depression (partial η2=48) and thinking problem (partial η2=44) after adjusting for baseline differences. Both ADHD groups performed significantly worse than the TD group, with the ADHD non-training group showing noticeably worse outcomes than the ADHD training group. Significant group differences were also noted in the following areas: Attention issues (partial η²=0.37), delinquent conduct (partial η²=0.42), withdrawn (partial η²=0.26), social problems (partial η²=0.24), and violent behavior (partial η²=0.39).In these subscales, the ADHD non-training group showed worse performance relative to the TD group.
Within-group differences between pre- and post-training
Table 5 displays Cohen’s d values for within-group comparisons between pre- and post-training outcomes.
ADHD training group: Following instruction, The ADHD training group’s behavioral problem subscales showed a notable improvement. All four of the behavioral disorder factors—social issues, aggressive conduct, delinquent behavior, and withdrawn—showed significant effect sizes. For the ADHD training group, anxiety/depression and concentration issues produced medium impact sizes. ADHD non-training group: Neither behavioral disorder measure showed any appreciable improvements in the ADHD non-training group. TD non-training group: Delinquent behavior scores showed medium effect sizes after the intervention. The scores for aggressive behavior, attention issues, withdrawn, and anxiety/depression showed small impact sizes.
Discussion
The effectiveness of a 12-week virtual PA intervention for lowering behavioral disorders in kids with ADHD was evaluated in this study. Although there were no discernible variations in behavioral disorder parameters between the two ADHD groups according to baseline assessments, both groups performed noticeably worse than the normally developing (TD) group on all behavioral disorder subscales. Although the ADHD training group shown notable improvements in comparison to the ADHD non-training group, both ADHD groups continued to perform worse than the TD group in terms of behavioral outcomes after the intervention. These gains persisted throughout the period of follow-up retention. These results are consistent with other research showing that children with ADHD have more behavioral issues [28-31] and are less physically active and mobile [32-35] than children with TD. these findings are in line with previous meta-analyses supporting the role of structured PA in reducing ADHD symptoms. For example, Zhu et al. [8] and Ye et al. [9] reported that PA interventions have medium-to-large effect sizes on executive function and behavioral regulation in children with ADHD. Specifically, skill-based and cognitively engaging programs, such as the one used in this study, were found to yield greater benefits than generic PA alone. The improvements observed here also mirror outcomes from RCTs on structured exercise programs targeting neurocognitive and emotional regulation, such as those by Cerrillo-Urbina et al. [36] and Liang et al. [37], which demonstrated reductions in hyperactivity and externalizing behaviors. Regarding sustainability, the improvements were maintained at 12-week follow-up, supporting the long-term potential of VPA interventions. This durability aligns with findings from trials such as Svedell et al. [31] and Verret et al. [38], which reported lasting effects of PA on attention and behavior in ADHD populations up to several months post-intervention. The retention of gains in our study may be due to the interactive and motivating format of VPA, which facilitates continued cognitive and emotional engagement even after formal sessions end. Children with ADHD typically exhibit significantly lower motor abilities than expected for their age and cognitive functioning level [30, 39, 40]. Engaging in structured sports training not only enhances physical conditioning but also provides positive stimuli that help divert attention away from anxiety-provoking or stressful situations [19, 28, 37]. Furthermore, PA stimulates the vestibular nervous system and enhances higher-order brain functions, such as motor skills and sensorimotor integration. These improvements foster increased self-confidence and a sense of self-efficacy, which in turn can alleviate ADHD symptoms [36, 39].
In explaining the effect of virtual movement activities on behavioral disorders, it can be stated that ADHD is a neurological disorder, and problems in the frontal lobe and the executive functions of the brain are among its main causes; Therefore, the implementation of some exercises can reduce the severity of the disorder and the problems associated with it [40]. Movement-based interventions improve cognitive functions such as processing speed, working memory, planning, and problem-solving, which in turn help reduce behavioral problems in children with ADHD [29]. In fact, the results of studies have shown that a structured exercise program can have a clinical and therapeutic relationship in the adjustment of children suffering from ADHD and raises the brain’s dopamine and norepinephrine levels, which leads to mental peace and emotional stability and focus on movements and ultimately, reducing their behavioral problems [36, 41]. Finally, providing opportunities for practice is a crucial component in enriching the developmental environment for children’s growth and learning [42]. The results of studies in the field of children with developmental disorders have come to the conclusion that these children are limited in terms of play space and PA at home, and these restrictions can have harmful effects on all-round growth factors [28, 38, 43]. In addition, the lack of suitable and effective supplies and equipment, especially the structure and educational program for PA or movement experience, affects their movement and behavioral development [36, 37, 41]; Therefore, the types of special physical exercises that were used in this research Improvement the behavioral factors of ADHD children.
Conclusion
According to the findings of this study, movement-based exercises can successfully improve behavioral abnormalities in children with ADHD. Consequently, parents and schools should actively support and encourage these children’s participation in structured group and individual physical activities. However, this study has limitations such as lack of blinding of outcome assessors, potential expectation bias due to the online nature of the intervention, lack of accurate tracking of virtual sessions, lack of control for economic and nutritional variables, and limited sample size to male gender. future research is recommended to compare the effects of virtual movement activities with other intervention programs that target fitness and behavioral symptoms in children with ADHD. In addition, it is recommended that clinicians and therapists include virtual movement activity programs as part of comprehensive treatment strategies for managing behavioral disorders in children with ADHD.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Shahid Chamran University, Ahvaz, Iran (Code: IR.SCU.REC.1404.035) and All procedures complied with the Declaration of Helsinki (1975). Parents provided written informed consent, and confidentiality of all data was ensured.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Data analysis and drafting the manuscript: Ayoub Hashemi and Elahe Siavashi; Critical revisions and intellectual input: Abouzar saadatian and Rasoul Abedanzadeh; Study design, data collection, data analysis, manuscript preparation and final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgements
The authors would like to express their gratitude to each and every participant for their invaluable assistance in gathering the study’s data.
References
Attention deficit hyperactivity disorder (ADHD) is a common neurodevelopmental disorder, affecting approximately 5% of children and adolescents globally [1, 2]. It is marked by persistent inattention, hyperactivity, and impulsivity, which significantly impair academic performance, behavioral regulation, and social functioning [1, 3]. While physical activity (PA) is widely recognized for its cardiovascular, motor and obesity-related benefits [4, 5] , it has also shown promise in supporting neurocognitive function, behavioral control, and overall quality of life in children with ADHD [6-8]. Recent meta-analyses provide compelling support for PA as an effective intervention for ADHD. For instance, Ye et al. [9] and Zhu et al. [8] found medium to large effect sizes for PA interventions in improving executive function, attention, and hyperactivity symptoms in children with ADHD. Moreover, skill-based PA programs—which emphasize coordination, planning, and cognitive engagement—have been shown to produce stronger cognitive benefits than general physical activities [5]. Despite these positive outcomes, traditional PA formats may fail to sustain the attention or interest of children with ADHD, which impacts adherence [5]. Additionally, standard ADHD treatments—such as pharmacotherapy and behavioral therapy—can be burdensome or carry undesirable side effects [10, 11]. These challenges highlight the need for alternative, engaging approaches. One promising avenue is virtual PA (VPA), which blends exercise with interactive technologies to create immersive and adaptive experiences [12, 13]. VPA environments can be tailored to individual needs, accounting for the impulsivity, distractibility, and executive function deficits often present in ADHD. These digital tools can increase engagement and program adherence by offering gamified, feedback-rich, and personally meaningful experiences [14, 15]. However, the literature on the specific effects of VPA on behavioral outcomes in ADHD is still limited. While general benefits of PA are well-documented, few studies directly compare traditional and virtual formats in ADHD populations [16, 17]. Given the complexity of ADHD and its comorbid challenges such as anxiety, depression, and conduct problems, investigating VPA as a targeted intervention is both timely and necessary [9, 18]. The purpose of this study is to evaluate critically how well VPA training to improve behavioral outcomes in children with ADHD. By addressing these research gaps, this study attempts to explore the role of VPA as a practical and useful intervention for managing ADHD symptoms in limited settings. Therefore, we hypothesize that: Children with ADHD participating in a structured VPA program will show significant improvements in behavioral outcomes as measured by the CBCL compared to those in control groups not engaged in such activities. From a societal perspective, the findings of this study have the potential to influence public health policies and educational strategies. Given the high costs of ADHD treatment and the societal burden of managing this disorder, identifying effective and accessible interventions is of paramount importance. Furthermore, the results of this study can provide valuable guidance for educational institutions, healthcare providers, and parents to support children with ADHD to achieve their full potential and provide a framework for future research on the long-term benefits of VPA in the management of ADHD in different settings.
Materials and Methods
Research design
A semi-experimental design was used in this study, and comparison groups participated in pre-, post-, and follow-up assessments. In order to reduce baseline differences between groups, participants were matched on important variables like age, ADHD subtype, and presence of comorbidities after being chosen based on predetermined eligibility criteria. Following the matching process, participants were randomly assigned to one of two groups: The experimental group, which received the VPA intervention, and the control group, which did not receive any intervention but was assessed at the same three time points. Additionally, a third group of usually developing children, designated as the HC group, was added to examine if children with ADHD might obtain equivalent behavioral outcomes following the intervention. Sample size calculations were conducted using G*Power software, version 3.1.9.2, based on a significance level of 5%, an effect size of 0.3, and a statistical power of 80%. The analysis indicated that a minimum of 50 participants would be necessary. To account for potential attrition, the total sample size was increased to 80 participants (40 in each group).
Participants and procedure
The study involved boys aged 7–10 years enrolled in elementary schools in Shiraz, Iran (2025). The focus on boys reflected national regulations requiring male teachers for male students. Inclusion criteria were as follows: 1) age between 7 and 10 years; 2) a clinical diagnosis of ADHD confirmed by a child psychiatrist or developmental psychologist, along with results from the Conner’s parents ratting scale (CPRS) (1979); 3) a formal recommendation from a healthcare provider for participation in the study; and 4) an IQ>80, as measured by the Wechsler intelligence scale for children–fourth edition [19]. Sampling followed a multi-stage design. First, 10 schools were randomly chosen from 40 public boys’ schools. Next, 800 Conners’ parent rating scale (CPRS) (1979) [20] questionnaires were distributed to parents and teachers; 580 were returned. Based on the questionnaires’ scores and follow-up clinical evaluations, 86 children met the inclusion criteria. After six withdrew, 80 children comprised the final ADHD sample. This final step was purposive, guided by predefined eligibility and exclusion criteria. To balance baseline characteristics, participants were matched on age, ADHD subtype, and comorbid conditions. They were then randomly assigned to either the experimental group (VPA) or the control group (no intervention), with 40 children in each. A separate healthy control (HC) group of 40 typically developing (TD) children was randomly recruited from two other schools. Their typical development was confirmed by psychiatric evaluation. Behavioral assessments were conducted at three time points: One week before the intervention (baseline), immediately after the 12-week program (post-test), and 12 weeks later (follow-up). Each session lasted about 60 minutes.
Intervention
Following the pre-test, the experimental group (40 children with ADHD) participated in the designed program for 12 weeks through online sessions, while the control group (40 children with ADHD) continued their daily routines without engaging in any structured PA program or receiving specific medical treatments. The intervention was developed based on established principles of physical education for children [21] and designed using the FITT framework (frequency, intensity, time, and type). The experimental group received the program twice weekly (Saturdays and Tuesdays) for 60 minutes per session. Each session consisted of a 5-minute class preparation, 5 minutes of warm-up, 45 minutes of main exercises, and 5 minutes of cool-down, with warm-up and cool-down delivered in the form of movement-based games. The 45-minute core component was divided into three 15-minute segments, each focusing on a fundamental motor skill domain: Locomotor, manipulative, and stability skills. Activity design was based on movement concepts (body awareness, spatial awareness, movement quality, and relationships), and the level of challenge was adjusted accordingly. Equipment included commonly available items such as hula hoops, cones, and balls, supplemented by household materials. Sessions were delivered via the Zoom videoconferencing platform, allowing real-time interaction between instructors and participants. Children were required to keep their cameras on so that instructors could continuously monitor performance. In addition, a parent was present during each session to provide assistance and ensure safe participation. To monitor adherence and quality of engagement, instructors used standardized checklists for attendance and task performance, and session reports were documented after each class. The program was led by experienced physical education instructors, in collaboration with the study authors, following a pre-established lesson plan.
Measures
Three time points were used to evaluate behavioral disorder indicators: Before the intervention (time 1), just after the 12-week intervention period (time 2), and at a 12-week follow-up (time 3). To reduce bias, all evaluations were carried out by qualified research personnel who were blind to group assignment. Standardized measurement training and comprehensive protocol instructions covering the administration of all evaluations were provided to the research team in order to guarantee data consistency and reliability. To ensure procedural fidelity, a senior researcher oversaw each testing session. Participants were instructed to adhere to consistent dietary practices on the main testing days and were allowed to consume only distilled water prior to testing to reduce confounding variables.
Conner’s parents ratting scale–revised short form (CPRS- R)
The parent form of the Conners questionnaire was developed by Conners et al. to assess behavioral problems associated with ADHD. The short form of this scale was presented in 1997 by Conners et al. This form has 27 questions in four subscales: Cognitive (inattention deficit; 6 questions), hyperactivity (6 questions), oppositional defiant (6 questions), and index (9 questions), and parents rate the extent and severity of each behavior on a four-point scale, from 0 (not at all true, never or rarely) to 3 (completely true, most of the time or almost always) [22]. Considering the number of questions, the total score of the questionnare ranges from 27 to 108. Obtaining a score of 1.5 or more for any question indicates the presence of ADHD. Cronbach’s α coefficient in these scales has been reported to be 0.91 to 0.93 [23]. the Persian version of CPRS used in this study has been validated for use with Iranian children. Shahim et al. reported strong internal consistency (Cronbach’s α ranging from 0.71 to 0.86) and appropriate construct validity, supporting its use in Iranian clinical settings [24]. It should be noted that this questionnaire was used only as a diagnostic tool and inclusion criterion in the study and was not used in the evaluation of outcomes.
Parent reports of child behavior (CBCL)
Child behavior was assessed using the child behavior checklist, a 113-item parent-report measure rated on a 3-point Likert scale (0=not true, 1=somewhat true, 2=very true) [25]. The CBCL yields scores on eight syndrome subscales: Anxiety/depression (14 items; 0–28), withdrawn (8 items; 0–16), somatic complaints (11 items; 0–22), social problems (11 items; 0–22), thinking problems (15 items; 0–30), attention problems (10 items; 0–20), delinquent behavior (17 items; 0–34), and aggressive behavior (18 items; 0–36). Two broadband dimensions are derived: Internalizing problems (0–66) and externalizing problems (0–70), as well as a total problems score (0–226). T-scores <65 indicate the non-clinical range, 65–69 borderline, and ≥70 clinical. The validity of this test is 0.98 and its reliability is 0.84 [26].The Persian version of the CBCL has been validated by Yazdkhasti & Oreyzi, demonstrating excellent reliability (Cronbach’s α >0.85) and strong convergent validity, making it a culturally appropriate tool for behavioral assessment in Iranian children [27].
Statistical analysis
SPSS software, version 23, was used for all statistical analyses, and P<0.01 was chosen as the significance level. To compare groups, demographic factors such as age, height, weight, body mass index (BMI), and IQ were examined using independent t-tests. Indicators of behavioral disorders, such as anxiety/depression, withdrawn, physical complaints, social problems, cognitive issues, attention issues, delinquent behavior, and violent behavior, were among the dependent variables examined in this study. To assess the effects of the intervention, a series of combined two-way variance analysis (3 [times]×3 [groups]) with repeated measurement applied for behavioral disorders outcomes. If any interaction was considered significant, simple main effects were determined. Effect sizes were reported using η² (eta squared) for analyses of variance (ANOVA), providing an estimate of the proportion of variance explained by the independent variable. For paired t-tests, Cohen’s d was calculated to assess the magnitude of within-group changes over time. Paired t-tests were employed specifically to evaluate the potential maintenance effects of the intervention across different time points. The presuppositions of variance analysis test with repeated measurement (normality, homogeneity, homogeneity of regression slopes, linearity and Mauchly’s sphericity) were checked and confirmed before data analysis.
Results
There were no significant differences between the groups on demographic variables at baseline, including age, height, weight, BMI, and IQ (Table 1), indicating successful matching and randomization. It is worth mentioning that one child dropped out of the ADHD training group at time 1. Also, at Time 3, one child from the ADHD training group and 9 children from the ADHD non training group withdrew and did not participate in the research. To check the level of PA (intervention), heart rate and exercise duration were measured. The average duration of training in each session was 53.20±2.80 minutes and the training intensity was 80 heart beats, which indicates moderate to intense PA.
Group comparability
Pre training: Table 2 displays the results according to the behavioral disorders subscales. The behavioral disorder subscales, which include anxiety/depression, withdrawn, social problems, thought problems, attention problems, delinquent behavior, and violent behavior, showed significant group differences, according to the results. Both ADHD subgroups significantly underperformed the normally developing (TD) group on all behavioral problem subscales, according to post hoc pairwise comparisons. But there was no significant difference between two ADHD subgroups.
Post training: The outcomes of the post-training behavioral disorders’ subscales are compiled in Table 3. Significant group differences were seen in a number of behavioral disorder subscales after adjusting for pre-training differences. In particular, both ADHD groups outperformed the TD group on post-training scores for anxiety/depression (partial η²=0.47) and thinking problems (partial η²=0.43), with the ADHD non-training group performing noticeably worse than the ADHD training group. Significant differences were also observed in the following areas: Attention issues (partial η²=0.36), delinquent conduct (partial η²=0.41), withdrawn (partial η²=0.25), social problems (partial η²=0.23), and violent behavior (partial η²=0.38). In these subscales, the ADHD non-training group demonstrated worse performance compared to the TD group.
Follow-up stage: The outcomes of the behavioral disorders subscales’ follow-up training are compiled in Table 4. The results showed significant group differences in the post-training anxiety/depression (partial η2=48) and thinking problem (partial η2=44) after adjusting for baseline differences. Both ADHD groups performed significantly worse than the TD group, with the ADHD non-training group showing noticeably worse outcomes than the ADHD training group. Significant group differences were also noted in the following areas: Attention issues (partial η²=0.37), delinquent conduct (partial η²=0.42), withdrawn (partial η²=0.26), social problems (partial η²=0.24), and violent behavior (partial η²=0.39).In these subscales, the ADHD non-training group showed worse performance relative to the TD group.
Within-group differences between pre- and post-training
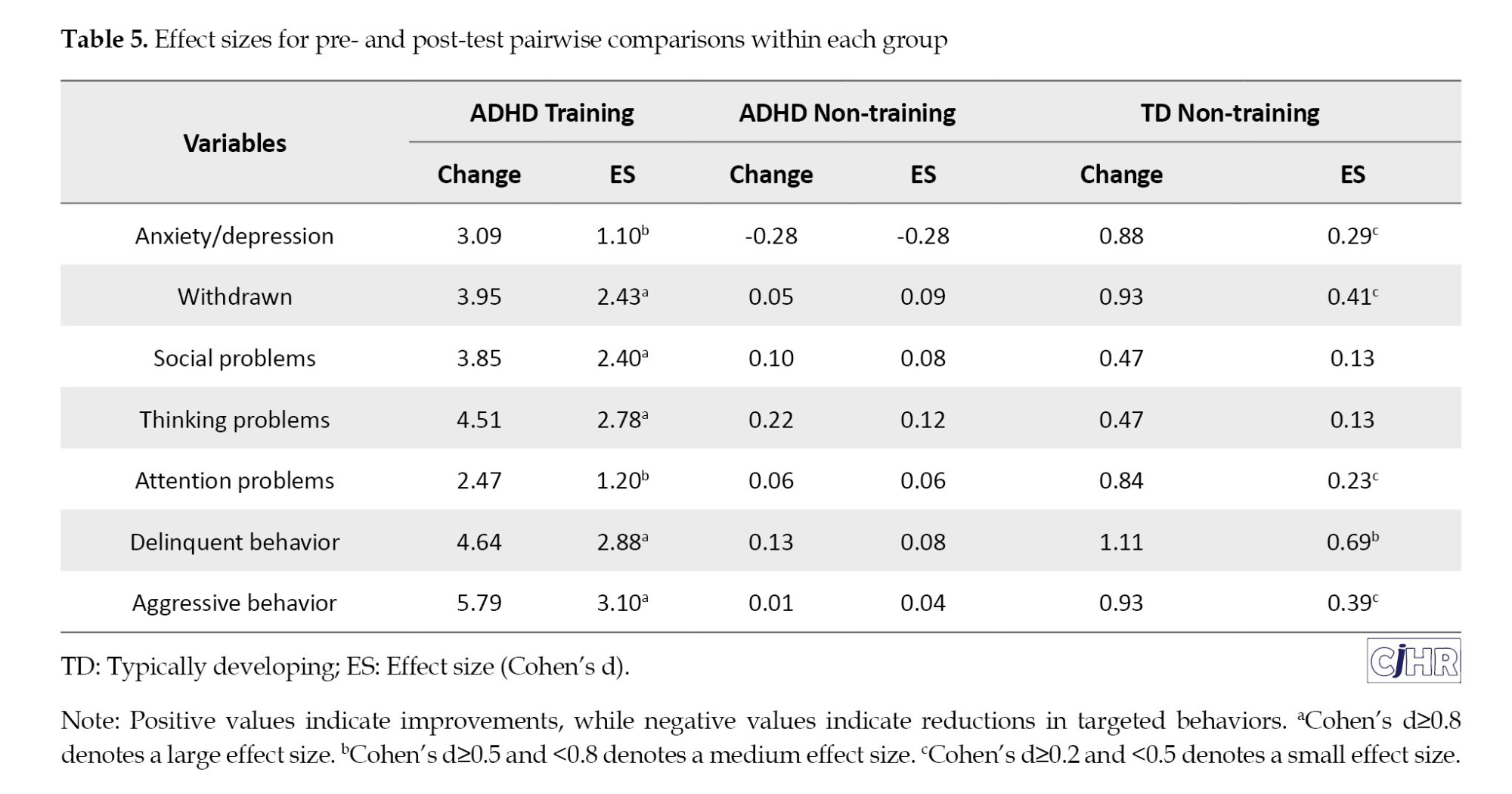
Table 5 displays Cohen’s d values for within-group comparisons between pre- and post-training outcomes.
ADHD training group: Following instruction, The ADHD training group’s behavioral problem subscales showed a notable improvement. All four of the behavioral disorder factors—social issues, aggressive conduct, delinquent behavior, and withdrawn—showed significant effect sizes. For the ADHD training group, anxiety/depression and concentration issues produced medium impact sizes. ADHD non-training group: Neither behavioral disorder measure showed any appreciable improvements in the ADHD non-training group. TD non-training group: Delinquent behavior scores showed medium effect sizes after the intervention. The scores for aggressive behavior, attention issues, withdrawn, and anxiety/depression showed small impact sizes.
Discussion
The effectiveness of a 12-week virtual PA intervention for lowering behavioral disorders in kids with ADHD was evaluated in this study. Although there were no discernible variations in behavioral disorder parameters between the two ADHD groups according to baseline assessments, both groups performed noticeably worse than the normally developing (TD) group on all behavioral disorder subscales. Although the ADHD training group shown notable improvements in comparison to the ADHD non-training group, both ADHD groups continued to perform worse than the TD group in terms of behavioral outcomes after the intervention. These gains persisted throughout the period of follow-up retention. These results are consistent with other research showing that children with ADHD have more behavioral issues [28-31] and are less physically active and mobile [32-35] than children with TD. these findings are in line with previous meta-analyses supporting the role of structured PA in reducing ADHD symptoms. For example, Zhu et al. [8] and Ye et al. [9] reported that PA interventions have medium-to-large effect sizes on executive function and behavioral regulation in children with ADHD. Specifically, skill-based and cognitively engaging programs, such as the one used in this study, were found to yield greater benefits than generic PA alone. The improvements observed here also mirror outcomes from RCTs on structured exercise programs targeting neurocognitive and emotional regulation, such as those by Cerrillo-Urbina et al. [36] and Liang et al. [37], which demonstrated reductions in hyperactivity and externalizing behaviors. Regarding sustainability, the improvements were maintained at 12-week follow-up, supporting the long-term potential of VPA interventions. This durability aligns with findings from trials such as Svedell et al. [31] and Verret et al. [38], which reported lasting effects of PA on attention and behavior in ADHD populations up to several months post-intervention. The retention of gains in our study may be due to the interactive and motivating format of VPA, which facilitates continued cognitive and emotional engagement even after formal sessions end. Children with ADHD typically exhibit significantly lower motor abilities than expected for their age and cognitive functioning level [30, 39, 40]. Engaging in structured sports training not only enhances physical conditioning but also provides positive stimuli that help divert attention away from anxiety-provoking or stressful situations [19, 28, 37]. Furthermore, PA stimulates the vestibular nervous system and enhances higher-order brain functions, such as motor skills and sensorimotor integration. These improvements foster increased self-confidence and a sense of self-efficacy, which in turn can alleviate ADHD symptoms [36, 39].
In explaining the effect of virtual movement activities on behavioral disorders, it can be stated that ADHD is a neurological disorder, and problems in the frontal lobe and the executive functions of the brain are among its main causes; Therefore, the implementation of some exercises can reduce the severity of the disorder and the problems associated with it [40]. Movement-based interventions improve cognitive functions such as processing speed, working memory, planning, and problem-solving, which in turn help reduce behavioral problems in children with ADHD [29]. In fact, the results of studies have shown that a structured exercise program can have a clinical and therapeutic relationship in the adjustment of children suffering from ADHD and raises the brain’s dopamine and norepinephrine levels, which leads to mental peace and emotional stability and focus on movements and ultimately, reducing their behavioral problems [36, 41]. Finally, providing opportunities for practice is a crucial component in enriching the developmental environment for children’s growth and learning [42]. The results of studies in the field of children with developmental disorders have come to the conclusion that these children are limited in terms of play space and PA at home, and these restrictions can have harmful effects on all-round growth factors [28, 38, 43]. In addition, the lack of suitable and effective supplies and equipment, especially the structure and educational program for PA or movement experience, affects their movement and behavioral development [36, 37, 41]; Therefore, the types of special physical exercises that were used in this research Improvement the behavioral factors of ADHD children.
Conclusion
According to the findings of this study, movement-based exercises can successfully improve behavioral abnormalities in children with ADHD. Consequently, parents and schools should actively support and encourage these children’s participation in structured group and individual physical activities. However, this study has limitations such as lack of blinding of outcome assessors, potential expectation bias due to the online nature of the intervention, lack of accurate tracking of virtual sessions, lack of control for economic and nutritional variables, and limited sample size to male gender. future research is recommended to compare the effects of virtual movement activities with other intervention programs that target fitness and behavioral symptoms in children with ADHD. In addition, it is recommended that clinicians and therapists include virtual movement activity programs as part of comprehensive treatment strategies for managing behavioral disorders in children with ADHD.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Shahid Chamran University, Ahvaz, Iran (Code: IR.SCU.REC.1404.035) and All procedures complied with the Declaration of Helsinki (1975). Parents provided written informed consent, and confidentiality of all data was ensured.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Data analysis and drafting the manuscript: Ayoub Hashemi and Elahe Siavashi; Critical revisions and intellectual input: Abouzar saadatian and Rasoul Abedanzadeh; Study design, data collection, data analysis, manuscript preparation and final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgements
The authors would like to express their gratitude to each and every participant for their invaluable assistance in gathering the study’s data.
References
- McDonald NH. ADHD parenting guide for boys: Step-by-step strategies, behavior management, and tools for emotional support, academic success, and social skills development in boys with ADHD. London: Gaius Quill Publishing; 2024. [Link]
- Kocsis RN. Book review: Diagnostic and statistical manual of mental disorders: Fifth edition (DSM-5). Int J Offender Ther Comparative Crim. 2013; 57(12):1546-8. [DOI:10.1177/0306624X13511040]
- Koutsoklenis A, Honkasilta J. ADHD in the DSM-5-TR: What has changed and what has not. Front Psychiatry. 2023; 13:1064141. [DOI:10.3389/fpsyt.2022.1064141] [PMID]
- Isath A, Koziol KJ, Martinez MW, Garber CE, Martinez MN, Emery MS, et al. Exercise and cardiovascular health: A state-of-the-art review. Prog Cardiovasc Dis. 2023; 79:44-52. [DOI:10.1016/j.pcad.2023.04.008] [PMID]
- Manninen M, Magrum E, Campbell S, Belton S. The effect of game-based approaches on decision-making, knowledge, and motor skill: A systematic review and a multilevel meta-analysis. Eur Phys Educ Rev. 2025; 31(1):18-32. [DOI:10.1177/1356336X241245305]
- Bores-García D, Palacios-Ceña D, Jiménez-Antona C, Marconnot R. The meaning of physical education practice in students with attention-deficit hyperactivity disorder (ADHD). Res Q Exerc Sport. 2024; 95(3):656-63. [DOI:10.1080/02701367.2023.2294097] [PMID]
- Ganjeh P, Hagmayer Y, Meyer T, Kuhnert R, Ravens-Sieberer U, von Steinbuechel N, et al. Physical activity and the development of general mental health problems or attention-deficit hyperactivity disorder (ADHD) symptoms in children and adolescents: A cross-lagged panel analysis of long-term follow-up epidemiological data. Front Behav Neurosci. 2022; 16:933139. [DOI:10.3389/fnbeh.2022.933139] [PMID]
- Zhu F, Zhu X, Bi X, Kuang D, Liu B, Zhou J, et al. Comparative effectiveness of various physical exercise interventions on executive functions and related symptoms in children and adolescents with attention deficit hyperactivity disorder: A systematic review and network meta-analysis. Front Public Health. 2023; 11:1133727. [DOI:10.3389/fpubh.2023.1133727] [PMID]
- Ye Y, Ning K, Wan B, Shangguan C. The effects of the exercise intervention on fundamental movement skills in children with attention deficit hyperactivity disorder and/or autism spectrum disorder: A meta-analysis. Sustainability. 2023; 15(6):5206. [DOI:10.3390/su15065206]
- Groom MJ, Cortese S. Current Pharmacological treatments for ADHD. Curr Top Behav Neurosci. 2022; 57:19-50.[DOI:10.1007/7854_2022_330] [PMID]
- Lu SV, Leung BMY, Bruton AM, Millington E, Alexander E, Camden K, et al. Parents' priorities and preferences for treatment of children with ADHD: Qualitative inquiry in the MADDY study. Child Care Health Dev. 2022; 48(5):852-61. [DOI:10.1111/cch.12995] [PMID]
- Sarai G, Jayaraman PP, Tirosh O, Wickramasinghe N. Exploring virtual reality and exercise simulator interventions in patients with attention deficit hyperactivity disorder: Comprehensive literature review. JMIR Serious Games. 2025; 13:e57297. [DOI:10.2196/57297] [PMID]
- Sergis N, Troussas C, Krouska A, Tzortzi C, Bardis G, Sgouropoulou C. ADHD dog: A virtual reality intervention incorporating behavioral and sociocultural theories with gamification for enhanced regulation in individuals with attention deficit hyperactivity disorder. Computers. 2024; 13(2):46. [DOI:10.3390/computers13020046]
- Corrigan N, Păsărelu CR, Voinescu A. Immersive virtual reality for improving cognitive deficits in children with ADHD: A systematic review and meta-analysis. Virtual Real. 2023; 1-20. [DOI:10.1007/s10055-023-00768-1] [PMID]
- Wiebe A, Kannen K, Li M, Aslan B, Anders D, Selaskowski B, et al. Multimodal virtual reality-based assessment of adult ADHD: A feasibility study in healthy subjects. Assessment. 2023; 30(5):1435-53. [DOI:10.1177/10731911221089193] [PMID]
- DuPaul GJ, Eckert TL, Vilardo B. The effects of school-based interventions for attention deficit hyperactivity disorder: A meta-analysis 1996-2010. School Psychol Rev. 2012; 41(4):387-412. [DOI:10.1080/02796015.2012.12087496]
- Nolin P, Stipanicic A, Henry M, Lachapelle Y, Lussier-Desrochers D, Allain P. ClinicaVR: Classroom-CPT: A virtual reality tool for assessing attention and inhibition in children and adolescents. Comp Human Behav. 2016; 59:327-33. [DOI:10.1016/j.chb.2016.02.023]
- Achenbach TM. Child behavior checklist. In: Kreutzer, JS, DeLuca J, Caplan B, editors. Encyclopedia of clinical neuropsychology. New York: Springer; 2011. [DOI:10.1007/978-0-387-79948-3_1529]
- Yang P, Cheng CP, Chang CL, Liu TL, Hsu HY, Yen CF. Wechsler Intelligence Scale for Children 4th edition-Chinese version index scores in Taiwanese children with attention-deficit/hyperactivity disorder. Psychiatry Clin Neurosci. 2013; 67(2):83-91. [DOI:10.1111/pcn.12014] [PMID]
- Conners CK. (Conners 3) conners, Third edition. Los Angeles: Western Psychological Services; 2008. [Link]
- Donnelly FC, Mueller SS, Gallahue DL. Developmental physical education for all children: theory into practice. Champaign: Human Kinetics; 2016. [DOI:10.5040/9781718210400]
- Conners CK. Symptom patterns in hyperkinetic, neurotic, and normal children. Child Dev. 1970; 41(30:667-82. [DOI:10.1111/j.1467-8624.1970.tb01022.x]
- Conners CK, Sitarenios G, Parker JD, Epstein JN. The revised conners' parent rating scale (CPRS-R): Factor structure, reliability, and criterion validity. J Abnorm Child Psychol. 1998; 26(4):257-68. [DOI:10.1023/A:1022602400621]
- Shahim S, Yousefi F, Shahaeian A. Standardization and psycbometric characteristics of the conners’teacher rating scale. J Educ Psychol. 2007; 14(1-2):1-26. [Link]
- Achenbach TM. Manual for the teacher’s report form and 1991 profile. Burlington: Dept. of Psychiatry, University of Vermont; 1991. [Link]
- Achenbach TM, Dumenci L, Rescorla LA. Ratings of relations between DSM-IV diagnostic categories and items of the CBCL/6-18, TRF, and YSR. Burlington: University of Vermont; 2001. [Link]
- Yazdkhasti F, Oreyzi H. [Standardization of child, parent and teacher’s forms of child behavior checklist in the city of Isfahan (Pesian)]. Iran J Psychiatry Clin Psychol. 2011; 17(1):60-70. [Link]
- Chan YS, Jang JT, Ho CS. Effects of physical exercise on children with attention deficit hyperactivity disorder. Biomed J. 2022; 45(2):265-70. [DOI:10.1016/j.bj.2021.11.011] [PMID]
- Mayer JS, Hees K, Medda J, Grimm O, Asherson P, Bellina M, et al. Bright light therapy versus physical exercise to prevent co-morbid depression and obesity in adolescents and young adults with attention-deficit/hyperactivity disorder: study protocol for a randomized controlled trial. Trials. 2018; 19(1):140. [DOI:10.1186/s13063-017-2426-1] [PMID]
- Pan CY, Chang YK, Tsai CL, Chu CH, Cheng YW, Sung MC. Effects of physical activity intervention on motor proficiency and physical fitness in children with ADHD: An exploratory study. J Atten Disord. 2017; 21(9):783-95. [DOI:10.1177/1087054714533192] [PMID]
- Svedell LA, Holmqvist KL, Lindvall MA, Cao Y, Msghina M. Feasibility and tolerability of moderate intensity regular physical exercise as treatment for core symptoms of attention deficit hyperactivity disorder: A randomized pilot study. Front Sports Act Living. 2023; 5:1133256. [DOI:10.3389/fspor.2023.1133256] [PMID]
- Asarian F, Salehi M, Zalbagi Darestani M, Asadi A, Heidari MM, Rahimi H. The effect of mindful parenting-based telepsychology on behavioral symptoms of ADHD children during covid-19 outbreak. Int J Pediatr. 2024; 12(1):18461-73. [Link]
- Laguna GG, Ribeiro DB, Tavares BR, Cazé AB, Santos AC, Souza LG, et al. Behavior changes in children/adolescents with attention deficit hyperactivity disorder during the COVID-19 pandemic: A systematic review. Rev Bras Saude Mater Infant. 2023; 23:e20220353. [DOI:10.1590/1806-9304202300000353-en]
- Seal E, Vu J, Winfield A, Fenesi B. Impact of COVID-19 on physical activity in families managing ADHD and the cyclical effect on worsening mental health. Brain Sci. 2023; 13(6):887. [DOI:10.3390/brainsci13060887] [PMID]
- Swansburg R, Hai T, MacMaster FP, Lemay JF. Impact of COVID-19 on lifestyle habits and mental health symptoms in children with attention-deficit/hyperactivity disorder in Canada. Paediatr Child Health. 2021; 26(5):e199-207. [DOI:10.1093/pch/pxab030] [PMID]
- Cerrillo-Urbina AJ, García-Hermoso A, Sánchez-López M, Pardo-Guijarro MJ, Santos Gómez JL, Martínez-Vizcaíno V. The effects of physical exercise in children with attention deficit hyperactivity disorder: A systematic review and meta-analysis of randomized control trials. Child Care Health Dev. 2015; 41(6):779-88. [DOI:10.1111/cch.12255] [PMID]
- Liang X, Qiu H, Wang P, Sit CHP. The impacts of a combined exercise on executive function in children with ADHD: A randomized controlled trial. Scand J Med Sci Sports. 2022; 32(8):1297-312. [DOI:10.1111/sms.14192] [PMID]
- Verret C, Guay MC, Berthiaume C, Gardiner P, Béliveau L. A physical activity program improves behavior and cognitive functions in children with ADHD: an exploratory study. J Atten Disord. 2012; 16(1):71-80. [DOI:10.1177/1087054710379735] [PMID]
- S J, Arumugam N, Parasher RK. Effect of physical exercises on attention, motor skill and physical fitness in children with attention deficit hyperactivity disorder: A systematic review. Atten Defic Hyperact Disord. 2019; 11(2):125-37. [DOI:10.1007/s12402-018-0270-0] [PMID]
- Bruchhage MMK, Bucci MP, Becker EBE. Cerebellar involvement in autism and ADHD. Handb Clin Neurol. 2018; 155:61-72. [DOI:10.1016/B978-0-444-64189-2.00004-4] [PMID]
- Jeyanthi S, Arumugam N, Parasher RK. Effectiveness of structured exercises on motor skills, physical fitness and attention in children with ADHD compared to typically developing children-A pilot study. eNeurologicalSci. 2021; 24:100357. [DOI:10.1016/j.ensci.2021.100357] [PMID]
- Guan H, Okely AD, Aguilar-Farias N, Del Pozo Cruz B, Draper CE, El Hamdouchi A, et al. Promoting healthy movement behaviours among children during the COVID-19 pandemic. Lancet Child Adolesc Health. 2020; 4(6):416-8. [DOI:10.1016/S2352-4642(20)30131-0] [PMID]
- Mckenzie G, Willis C, Shields N. Barriers and facilitators of physical activity participation for young people and adults with childhood-onset physical disability: A mixed methods systematic review. Dev Med Child Neurol. 2021; 63(8):914-24. [DOI:10.1111/dmcn.14830] [PMID]
Article Type: Original Contributions |
Subject:
Public Health
Received: 2025/06/28 | Accepted: 2025/08/3 | Published: 2025/10/1
Received: 2025/06/28 | Accepted: 2025/08/3 | Published: 2025/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
