

Volume 6, Issue 1 (3-2021)
CJHR 2021, 6(1): 1-8 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Esan A, Adeleye J, Azeez T. Cardiovascular Risk Profile of Apparently Healthy Workers in a Tertiary Hospital in Nigeria. CJHR 2021; 6 (1) :1-8
URL: http://cjhr.gums.ac.ir/article-1-189-en.html
URL: http://cjhr.gums.ac.ir/article-1-189-en.html



1- Department of Medicine, University College Hospital, Ibadan, Nigeria.
2- Department of Medicine, University College Hospital, Ibadan, Nigeria. , adegokegalaxy@yahoo.com
2- Department of Medicine, University College Hospital, Ibadan, Nigeria. , adegokegalaxy@yahoo.com
Full-Text [PDF 804 kb]
(467 Downloads)
| Abstract (HTML) (1325 Views)
Full-Text: (503 Views)
1. Introduction
Cardiovascular disease is ranked top on the list of global health problems by the World Health Organization (WHO) [1]. Risk is defined as the probability of an event occurring over a specific period of time [2]and is a complex phenomenon difficult to evaluate. Therefore, it is often necessary to consider factors associated with a particular risk, otherwise, they are called risk factors. O’Donnell et al. defined risk factors as quantifiable characteristics associated with increased frequency of disease and as an independent predictor of the occurrence of a disease [3].
Payne classified cardiovascular risk factors into classic unmodifiable factors (such as age, gender, and family history), modifiable factors (such as blood pressure, lipid profile, and glucose intolerance), behavioral risk factors (such as smoking, excessive alcohol consumption, and sedentary lifestyle) and novel risk factors (such as C-reactive protein, adipokines, and homocysteine) [1]. It is recommended that cardiovascular disease management should be based on the utilization of objective risk scores, which are often computed from cardiovascular risk factors [4].
The various documented and validated cardiovascular risk scores include Framingham risk score, QRISK score, Systematic Coronary Risk Evaluation (SCORE), Prospective Cardiovascular Munster (PROCAM), and Atherosclerotic Cardiovascular Disease (ASCVD) [5, 6]. The QRISK score is a cardiovascular risk algorithm approved by the United Kingdom’s National Health Services and adopted by the National Institute of Health and Care Excellence (NICE) for primary prevention of cardiovascular disease [7] The updated QRISK 3 is the latest validated edition of the algorithm [8] and classifies the risk as low (<10), intermediate (10-20), and high (>20) [9].
Assessment of cardiovascular risk factors and cardiovascular risk scoring is important because they evaluate the risk of developing cardiovascular disease and guide appropriate preventive and therapeutic strategies [9]. Commencement of statin, for example, for primary prevention is dependent on the cardiovascular risk score. Also, cardiovascular disease is gradually becoming a major cause of morbidity and mortality among adults in Nigeria. Adegoke et al. reported that 51% of out-of-hospital deaths in Lagos, a cosmopolitan city in Nigeria, were due to cardiovascular-related causes [10]. Therefore, in a nation like Nigeria, where there is a limited health workforce, assessing cardiovascular risk is important to steer efforts at preventing cardiovascular disease and death among the personnel. Additionally, the limited health manpower is concentrated in the urban areas where cardiovascular risk tends to be relatively higher [11, 12]. Therefore, the objectives of this study were to identify cardiovascular risk factors among the workers of the University College Hospital, Ibadan, and estimate and stratify their 10-year cardiovascular risk.
Payne classified cardiovascular risk factors into classic unmodifiable factors (such as age, gender, and family history), modifiable factors (such as blood pressure, lipid profile, and glucose intolerance), behavioral risk factors (such as smoking, excessive alcohol consumption, and sedentary lifestyle) and novel risk factors (such as C-reactive protein, adipokines, and homocysteine) [1]. It is recommended that cardiovascular disease management should be based on the utilization of objective risk scores, which are often computed from cardiovascular risk factors [4].
The various documented and validated cardiovascular risk scores include Framingham risk score, QRISK score, Systematic Coronary Risk Evaluation (SCORE), Prospective Cardiovascular Munster (PROCAM), and Atherosclerotic Cardiovascular Disease (ASCVD) [5, 6]. The QRISK score is a cardiovascular risk algorithm approved by the United Kingdom’s National Health Services and adopted by the National Institute of Health and Care Excellence (NICE) for primary prevention of cardiovascular disease [7] The updated QRISK 3 is the latest validated edition of the algorithm [8] and classifies the risk as low (<10), intermediate (10-20), and high (>20) [9].
Assessment of cardiovascular risk factors and cardiovascular risk scoring is important because they evaluate the risk of developing cardiovascular disease and guide appropriate preventive and therapeutic strategies [9]. Commencement of statin, for example, for primary prevention is dependent on the cardiovascular risk score. Also, cardiovascular disease is gradually becoming a major cause of morbidity and mortality among adults in Nigeria. Adegoke et al. reported that 51% of out-of-hospital deaths in Lagos, a cosmopolitan city in Nigeria, were due to cardiovascular-related causes [10]. Therefore, in a nation like Nigeria, where there is a limited health workforce, assessing cardiovascular risk is important to steer efforts at preventing cardiovascular disease and death among the personnel. Additionally, the limited health manpower is concentrated in the urban areas where cardiovascular risk tends to be relatively higher [11, 12]. Therefore, the objectives of this study were to identify cardiovascular risk factors among the workers of the University College Hospital, Ibadan, and estimate and stratify their 10-year cardiovascular risk.
2. Materials and Methods
In this cross-sectional study, 52 apparently healthy workers of a tertiary hospital in Nigeria were studied after obtaining informed consent. The workers were divided into two categories: clinical workers (doctors, nurses, physiotherapists, and pharmacists) and nonclinical workers (administrative and security personnel).
Inclusion criteria for the participants
Apparently healthy members of staff of a tertiary hospital in Nigeria who gave consent to participate in the study were included.
Exclusion criteria for the participants
Apparently healthy hospital workers who refused to consent and/or who an acute illness or an acute decompensation of a chronic illness were excluded from the study. Also, pregnant women and individuals who had been admitted for an illness in the preceding 3 months as well as workers already diagnosed with a stroke, myocardial infarction, heart failure, or peripheral artery disease were exempted from the study.
Data collection and analysis
Structured and pre-tested questionnaires were administered to the participants to obtain the sociodemographic data. Weight was measured in Kilograms (to the nearest 0.1 kg) using a D-339 Detecto Eye-level Physician Beam Scale (made in the USA). Height was measured in meters (to the nearest 0.01 m) using a portable stadiometer. Body Mass Index (BMI) was calculated using the Formula 1 [13]:
1. BMI= Weight (kg)/Height2 (m2).
BMI of 18.5-24.9 kg/m2 was considered normal and 25-29.9 kg/m2 and greater than or equal to 30 kg/m2 were considered as overweight and obese, respectively [14]. Waist circumference was measured in centimeters (to the nearest 0.1 cm) using a standard technique as described by the WHO in the technical report on obesity with a flexible inelastic tape measure [15]. Values greater than or equal to 94 cm in males and greater than or equal to 80 cm in females were considered as truncal obesity [15].
Blood pressure was measured after the patient sat for about 5 minutes with a mercury sphygmomanometer (Accoson brand, made in England) following a standard technique as described by the European Society of Hypertension [16]. Three readings were taken and the average of the last two readings was recorded. Hypertension was taken as systolic blood pressure ≥ 140mmHg and/or diastolic blood pressure ≥ 90mmHg or being on treatment for hypertension [17].
Participants had a blood sample collected following an overnight fast of about 8 – 12 hours. Fasting plasma glucose was determined by glucose oxidase enzymatic method using Dialab glucose assay kit. Total cholesterol, total Triglyceride (TG), and High-Density Lipoprotein cholesterol (HDL-C ) was determined using the enzymatic method with the Dialab Kit. Low-Density Lipoprotein-Cholesterol (LDL-C) was calculated using the Friedewald equation provided that the TG was not more than 400mg/dl Formula 2 [18].
Total cholesterol greater than 200 mg/dl and/or total TG greater than 150 mg/dl and/or HDL-Cholesterol less than 40 mgldl in males or less than 50 mg/dl in females is considered as dyslipidemia. HbA1c was determined using the ion-exchange high-performance liquid chromatography method.
QRISK3 score was calculated using the appropriate online calculator [19]. The 10-year cardiovascular risk is considered low, intermediate, and high when the QRISK3 score is <10%, 10-20%, and > 20%, respectively [20].
The data collected was scrutinized for errors as soon as collected. They were coded and entered into Microsoft Excel datasheet before they were transferred to the program for data analysis. Data analysis was carried out using the Statistical Package for Social Sciences software (SPSS) version 22. Quantitative variables were presented as Mean±Standard Deviation or median (where deemed appropriate). Categorical variables were presented as frequencies or proportions. A comparison of the mean values was done using the Student’s t-test. A P-value less than 0.05 was considered to be statistically significant.
Definition of terms
Clinical health workers: Health workers that interact directly with patients and patients’ care, such as doctors, nurses, physiotherapists, dentists, and pharmacists.
Non-clinical workers: Health workers who do not interact directly with patients and patients’ care, such as administrative staff members and security operatives.
Glucose intolerance: Glycated haemoglobin ≥5.7% - 6.4% [21].
Dyslipidaemia: Fasting total cholesterol >200mgldl and/or fasting TG >150 mg/dl and/or LDL-C >130 mg/dl and or HDL-C <40 mg/dl (in males) or 50mgldl (in females) [22].
Hypertension: Systolic blood pressure ≥140 ng/dl and/or diastolic blood pressure ≥90 mg/dl or being on anti-hypertensives [23].
Obesity: Body mass index ≥30 kg/m2 [24].
Overweight: Body mass index of 25-29.9 kg/m2 [24].
Central obesity: Waist circumference ≥94 cm in males or 80 cm in females [25].
3. Results
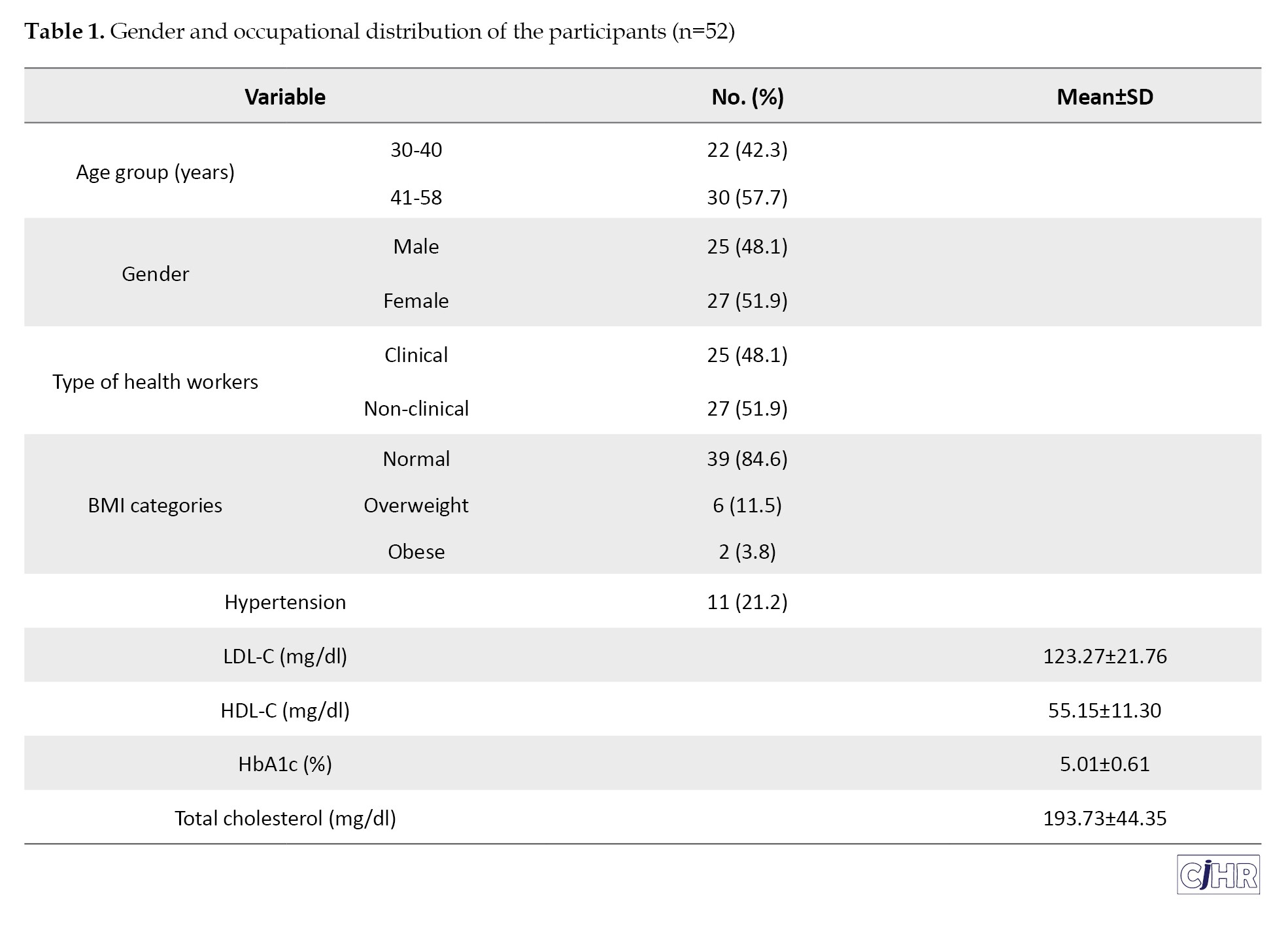
Fifty-two apparently health workers were recruited into the study who met the eligibility criteria. The age range was 30-58 years while the Mean±SD age was 44.9±8.1 years. Table 1 indicates the gender and occupational distribution of the participants and Figure 1 shows the frequency of cardiovascular risk factors among this cohort.
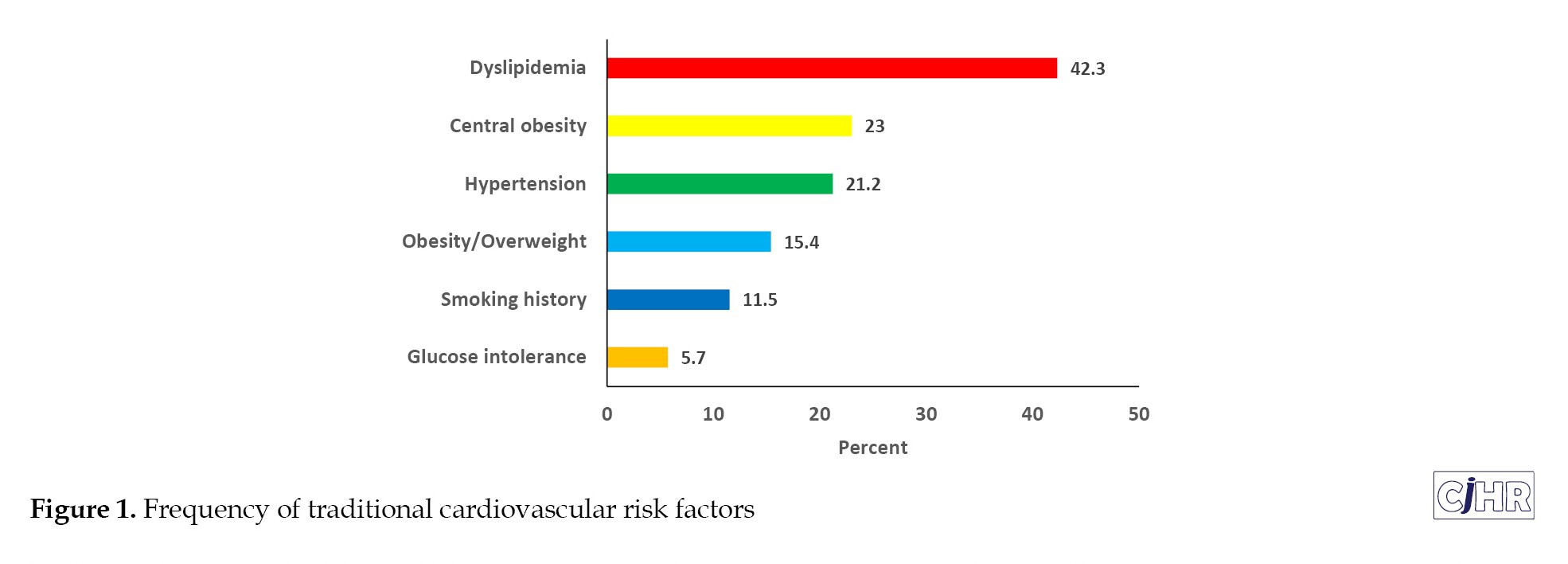
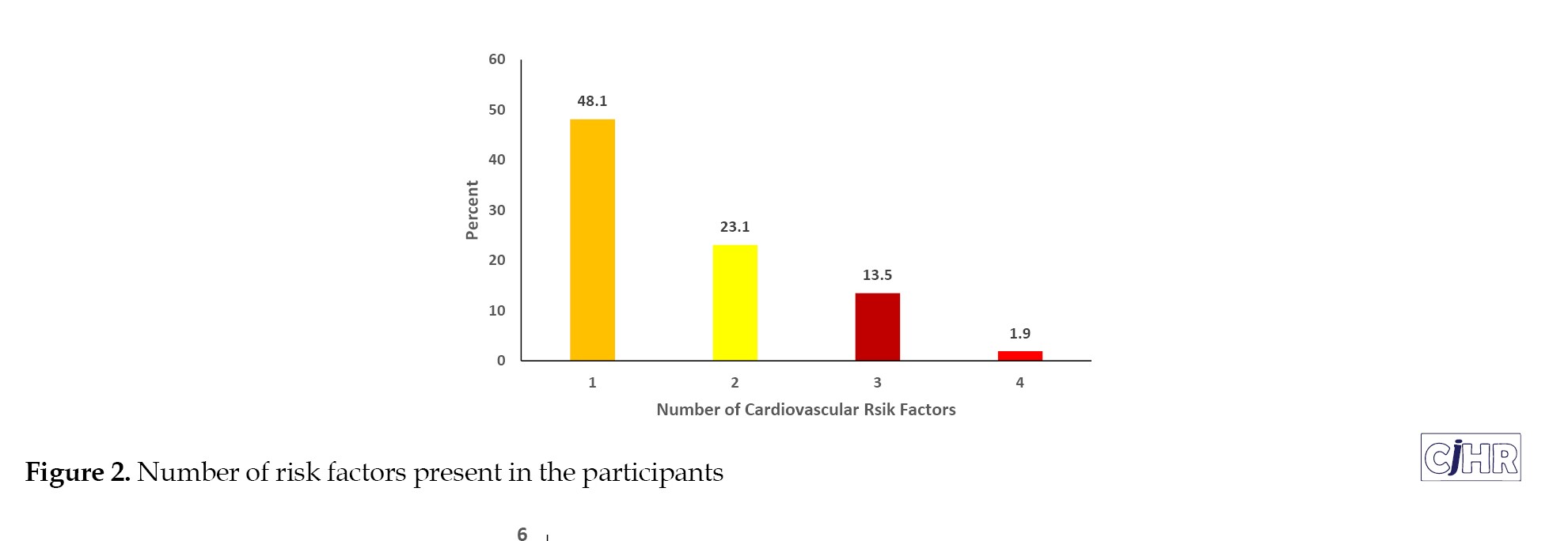
Dyslipidaemia was the most common risk factor among apparently healthy healthcare workers, while glucose intolerance was the least common. Figure 2 shows the number of risk factors present in the participants. Almost half of the participants had at least one cardiovascular risk factor and 15.4% of the participants had 3 or more cardiovascular risk factors.
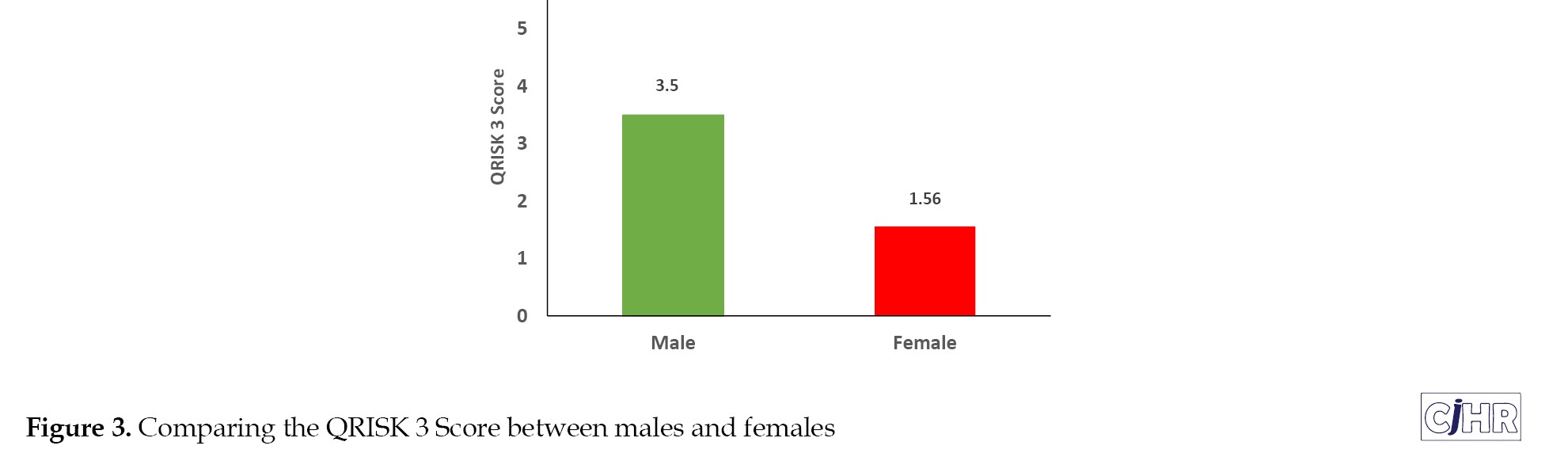
In terms of 10-year cardiovascular risk using QRISK3 score, none of the participants had high risk, 3.8% had moderate risk, while the rest had low risk. There was no statistically significant difference in the 10-year cardiovascular risk score between the clinical and non-clinical health workers (P=0.313; t=0.819). However, male participants had a significantly higher 10-year cardiovascular risk score compared with the females (3.50 vs. 1.56; P<0.001; t=3.741) (Figure 3).
Inclusion criteria for the participants
Apparently healthy members of staff of a tertiary hospital in Nigeria who gave consent to participate in the study were included.
Exclusion criteria for the participants
Apparently healthy hospital workers who refused to consent and/or who an acute illness or an acute decompensation of a chronic illness were excluded from the study. Also, pregnant women and individuals who had been admitted for an illness in the preceding 3 months as well as workers already diagnosed with a stroke, myocardial infarction, heart failure, or peripheral artery disease were exempted from the study.
Data collection and analysis
Structured and pre-tested questionnaires were administered to the participants to obtain the sociodemographic data. Weight was measured in Kilograms (to the nearest 0.1 kg) using a D-339 Detecto Eye-level Physician Beam Scale (made in the USA). Height was measured in meters (to the nearest 0.01 m) using a portable stadiometer. Body Mass Index (BMI) was calculated using the Formula 1 [13]:
1. BMI= Weight (kg)/Height2 (m2).
BMI of 18.5-24.9 kg/m2 was considered normal and 25-29.9 kg/m2 and greater than or equal to 30 kg/m2 were considered as overweight and obese, respectively [14]. Waist circumference was measured in centimeters (to the nearest 0.1 cm) using a standard technique as described by the WHO in the technical report on obesity with a flexible inelastic tape measure [15]. Values greater than or equal to 94 cm in males and greater than or equal to 80 cm in females were considered as truncal obesity [15].
Blood pressure was measured after the patient sat for about 5 minutes with a mercury sphygmomanometer (Accoson brand, made in England) following a standard technique as described by the European Society of Hypertension [16]. Three readings were taken and the average of the last two readings was recorded. Hypertension was taken as systolic blood pressure ≥ 140mmHg and/or diastolic blood pressure ≥ 90mmHg or being on treatment for hypertension [17].
Participants had a blood sample collected following an overnight fast of about 8 – 12 hours. Fasting plasma glucose was determined by glucose oxidase enzymatic method using Dialab glucose assay kit. Total cholesterol, total Triglyceride (TG), and High-Density Lipoprotein cholesterol (HDL-C ) was determined using the enzymatic method with the Dialab Kit. Low-Density Lipoprotein-Cholesterol (LDL-C) was calculated using the Friedewald equation provided that the TG was not more than 400mg/dl Formula 2 [18].
Total cholesterol greater than 200 mg/dl and/or total TG greater than 150 mg/dl and/or HDL-Cholesterol less than 40 mgldl in males or less than 50 mg/dl in females is considered as dyslipidemia. HbA1c was determined using the ion-exchange high-performance liquid chromatography method.
QRISK3 score was calculated using the appropriate online calculator [19]. The 10-year cardiovascular risk is considered low, intermediate, and high when the QRISK3 score is <10%, 10-20%, and > 20%, respectively [20].
The data collected was scrutinized for errors as soon as collected. They were coded and entered into Microsoft Excel datasheet before they were transferred to the program for data analysis. Data analysis was carried out using the Statistical Package for Social Sciences software (SPSS) version 22. Quantitative variables were presented as Mean±Standard Deviation or median (where deemed appropriate). Categorical variables were presented as frequencies or proportions. A comparison of the mean values was done using the Student’s t-test. A P-value less than 0.05 was considered to be statistically significant.
Definition of terms
Clinical health workers: Health workers that interact directly with patients and patients’ care, such as doctors, nurses, physiotherapists, dentists, and pharmacists.
Non-clinical workers: Health workers who do not interact directly with patients and patients’ care, such as administrative staff members and security operatives.
Glucose intolerance: Glycated haemoglobin ≥5.7% - 6.4% [21].
Dyslipidaemia: Fasting total cholesterol >200mgldl and/or fasting TG >150 mg/dl and/or LDL-C >130 mg/dl and or HDL-C <40 mg/dl (in males) or 50mgldl (in females) [22].
Hypertension: Systolic blood pressure ≥140 ng/dl and/or diastolic blood pressure ≥90 mg/dl or being on anti-hypertensives [23].
Obesity: Body mass index ≥30 kg/m2 [24].
Overweight: Body mass index of 25-29.9 kg/m2 [24].
Central obesity: Waist circumference ≥94 cm in males or 80 cm in females [25].
3. Results
Fifty-two apparently health workers were recruited into the study who met the eligibility criteria. The age range was 30-58 years while the Mean±SD age was 44.9±8.1 years. Table 1 indicates the gender and occupational distribution of the participants and Figure 1 shows the frequency of cardiovascular risk factors among this cohort.
Dyslipidaemia was the most common risk factor among apparently healthy healthcare workers, while glucose intolerance was the least common. Figure 2 shows the number of risk factors present in the participants. Almost half of the participants had at least one cardiovascular risk factor and 15.4% of the participants had 3 or more cardiovascular risk factors.
In terms of 10-year cardiovascular risk using QRISK3 score, none of the participants had high risk, 3.8% had moderate risk, while the rest had low risk. There was no statistically significant difference in the 10-year cardiovascular risk score between the clinical and non-clinical health workers (P=0.313; t=0.819). However, male participants had a significantly higher 10-year cardiovascular risk score compared with the females (3.50 vs. 1.56; P<0.001; t=3.741) (Figure 3).
4. Discussion
This study documented a high prevalence of cardiovascular risk factors among apparently healthy healthcare workers in a tertiary hospital in Nigeria. In a similar study done among healthcare workers in a municipal hospital in Ghana, cardiometabolic risk factors were documented to be prevalent among apparently healthy participants [26]. Previous studies have shown that the prevalence of cardiovascular risk factors among healthcare workers is often comparable with those of their community despite the fact that healthcare workers are believed to be better equipped with knowledge of cardiovascular risk factors and their modification strategies [26-28]. Ike and Onyema have affirmed that the prevalence of cardiovascular risk factors among the Nigerian population is on the rise [29].
This study found the frequency of glucose intolerance among the participants as 7.9%. This is similar to the 10.5% that Lawal et al. documented in their cohort of employees in a tertiary hospital in Northern Nigeria [30]. Similarly, Bakari et al. reported a prevalence of 7.4% among the apparently healthy population of Nigerians [31]. The frequency of ex-smokers and present smokers was 11.5% in the present study. In a meta-analysis, Adeloye et al. reported the prevalence of current and ex-smokers amongst the general population in Nigeria as 17.7% [32]. Campaign against unhealthy living, including smoking cessation in health facilities, may account for the slightly lower prevalence in the present study compared with the general population.
Furthermore, among the outcomes of the study was a prevalence of central obesity of 23%. In a large population of apparently healthy Eastern Nigerian population, central obesity prevalence was reported as 21.7%, which is in accordance with the findings of the present study [33]. Interestingly, the frequency of overweight and obesity in this study (15.4%) would imply that some individuals with normal BMI had central obesity and their cardiovascular risk may be underestimated using BMI alone. Ijezie et al. reported the same observation in their cohort of apparently healthy Nigerians [33].
Additionally, among the participants in this study, 21.3% had hypertension. This is in keeping with the findings of Konin et al who reported the prevalence of hypertension among apparently healthy nursing staff of a hospital in Abidjan, Cote d’Ivoire as 17.5%; however, their subjects were largely female [34]. As regards dyslipidemia, its frequency in this study was 42.3%, similar to the study done among apparently healthy members of staff of a university in Southern Nigeria, which found a prevalence of 49.5% [35]. In the cardiovascular profiling of the participants in this study, clustering of cardiovascular risk factors was a prevalent finding. Other authors have reported clustering of cardiovascular risk factors among apparently healthy healthcare workers [28, 30, 34].
This study suffered from a limited sample size as this was a pilot study, which might make it difficult to draw conclusions. Therefore, it is recommended that further studies with a larger sample size be conducted to further characterize the frequency and pattern of cardiovascular risk factors among healthcare workers.
This study found the frequency of glucose intolerance among the participants as 7.9%. This is similar to the 10.5% that Lawal et al. documented in their cohort of employees in a tertiary hospital in Northern Nigeria [30]. Similarly, Bakari et al. reported a prevalence of 7.4% among the apparently healthy population of Nigerians [31]. The frequency of ex-smokers and present smokers was 11.5% in the present study. In a meta-analysis, Adeloye et al. reported the prevalence of current and ex-smokers amongst the general population in Nigeria as 17.7% [32]. Campaign against unhealthy living, including smoking cessation in health facilities, may account for the slightly lower prevalence in the present study compared with the general population.
Furthermore, among the outcomes of the study was a prevalence of central obesity of 23%. In a large population of apparently healthy Eastern Nigerian population, central obesity prevalence was reported as 21.7%, which is in accordance with the findings of the present study [33]. Interestingly, the frequency of overweight and obesity in this study (15.4%) would imply that some individuals with normal BMI had central obesity and their cardiovascular risk may be underestimated using BMI alone. Ijezie et al. reported the same observation in their cohort of apparently healthy Nigerians [33].
Additionally, among the participants in this study, 21.3% had hypertension. This is in keeping with the findings of Konin et al who reported the prevalence of hypertension among apparently healthy nursing staff of a hospital in Abidjan, Cote d’Ivoire as 17.5%; however, their subjects were largely female [34]. As regards dyslipidemia, its frequency in this study was 42.3%, similar to the study done among apparently healthy members of staff of a university in Southern Nigeria, which found a prevalence of 49.5% [35]. In the cardiovascular profiling of the participants in this study, clustering of cardiovascular risk factors was a prevalent finding. Other authors have reported clustering of cardiovascular risk factors among apparently healthy healthcare workers [28, 30, 34].
This study suffered from a limited sample size as this was a pilot study, which might make it difficult to draw conclusions. Therefore, it is recommended that further studies with a larger sample size be conducted to further characterize the frequency and pattern of cardiovascular risk factors among healthcare workers.
5. Conclusion
Cardiovascular risk factors are prevalent among healthcare workers just like the general population. There is a need to intensify efforts at prevention, early detection, and treatment of these cardiovascular risk factors among healthcare workers to mitigate the untoward effects of morbidity and mortality among them.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Ibadan (Code: NHREC/05/01/2008a). All ethical principles are considered in this article. The participants were informed about the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Both authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
- Payne RA. Cardiovascular risk. Br J Clin Pharmacol. 2012; 74(3):396-410. [DOI:10.1111/j.1365-2125.2012.04219.x] [PMID] [PMCID]
- Jackson R, Kerr A, Wells S. Is estimating lifetime cardiovascular risk useful? BMJ. 2010; 341:7379. [DOI:10.1136/bmj.c7379] [PMID]
- O’Donnell CO, Elosua R. Cardiovascular risk factors. Insights from framingham heart study. Rev Esp Cardiol. 2008; 61(3):299-310. [DOI:10.1016/S1885-5857(08)60118-8]
- US Preventive Services Task Force, Curry SJ, Krist AH, Owens DK, Barry MJ, Caughey AB, et al. Risk assessment for cardiovascular disease with nontraditional risk factors: US preventive services task force recommendation statement. JAMA. 2018; 320(3):272-80. [DOI:10.1001/jama.2018.8359] [PMID]
- Santos P. The role of cardiovascular risk assessment in preventive medicine: A perspective from Portugal primary health-care cardiovascular risk assessment. J Environ Public Health. 2020; 2020:1639634. [DOI:10.1155/2020/1639634] [PMID] [PMCID]
- Grammer TB, Dressel A, Gergei I, Kleber ME, Laufs U, Scharnagl H, et al. Cardiovascular risk algorithms in primary care: Results from the DETECT study. Sci Rep. 2019; 9(1):1101. [DOI:10.1038/s41598-018-37092-7] [PMID] [PMCID]
- Hippisley-Cox J, Coupland C, Vinogradova Y, Robson J, Minhas R, Sheikh A, et al. Predicting cardiovascular risk in England and Wales: Prospective derivation and validation of QRISK2. BMJ. 2008; 336(7659):1475-82. [DOI:10.1136/bmj.39609.449676.25] [PMID] [PMCID]
- Hippisley-Cox J, Coupland C, Brindle P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: Prospective cohort study. BMJ. 2017; 357:j2099. [DOI:10.1136/bmj.j2099] [PMID] [PMCID]
- Johns I, Moschonas KE, Medina J, Ossei-Gerning N, Kassianos G, Halcox JP. Risk classification in primary prevention of CVD according to QRISK2 and JBS3 'heart age', and prevalence of elevated high-sensitivity C reactive protein in the UK cohort of the EURIKA study. Open Heart. 2018; 5(2):e000849. [DOI:10.1136/openhrt-2018-000849] [PMID] [PMCID]
- Adegoke O, Awolola NA, Ajuluchukwu JN. Prevalence and pattern of cardiovascular-related causes of out-of- hospital deaths in Lagos, Nigeria. Afr Health Sci. 2018; 18(4):942-9. [DOI:10.4314/ahs.v18i4.13] [PMID] [PMCID]
- Global Health Workforce Alliance. GHWA completes its ten year mandate [Internet]. 2016 [Updated 2016 May 15]. Available from: https://www.who.int/workforcealliance/en/
- Moreno-Lostao A, Guerras JM, Lostao L, de la Fuente L, Martínez D, Rodríguez-Artalejo F, et al. Cardiovascular mortality and risk behaviours by degree of urbanization before, during and after the economic crisis in Spain. BMC Public Health. 2019; 19(1):1109. [DOI:10.1186/s12889-019-7427-4] [PMID] [PMCID]
- Garrow JS, Webster J. Quetelet's index (W/H2) as a measure of fatness. Int J Obes. 1985; 9(2):147-53. [PMID]
- Flegal KM, Kit BK, Graubard BI. Body mass index categories in observational studies of weight and risk of death. Am J Epidemiol. 2014; 180(3):288-96. [DOI:10.1093/aje/kwu111] [PMID] [PMCID]
- Nuttall FQ. Body mass index: obesity, BMI, and health: a critical review. Nutr Today. 2015; 50(3):117. [DOI:10.1097/NT.0000000000000092] [PMID] [PMCID]
- O'Brien E, Asmar R, Beilin L, Imai Y, Mallion JM, Mancia G, et al. European Society of Hypertension recommendations for conventional, ambulatory and home blood pressure measurement. J Hypertens. 2003; 21(5):821-48. [DOI:10.1097/00004872-200305000-00001] [PMID]
- Hernandez-Vila E. A review of the JNC 8 Blood Pressure Guideline. Tex Heart Inst J. 2015; 42(3):226-8. [DOI:10.14503/THIJ-15-5067] [PMID] [PMCID]
- Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low density lipoprotein cholesterol in plasma without the use of the preparative ultracentrifuge. Clin Chem. 1972; 18(6):499-502. [DOI:10.1093/clinchem/18.6.499]
- ClinRisk. QRISK®3-2018 risk calculator [Internet]. 2018 [Updated 2018]. Available from: https://qrisk.org/three/
- Edwards N, Langford-Smith AW, Parker BJ, Bruce IN, Reynolds JA, Alexander MY, et al. QRISK3 improves detection of cardiovascular disease risk in patients with systemic lupus erythematosus. Lupus Sci Med. 2018; 5(1):e000272. https://lupus.bmj.com/content/5/1/e000272.abstract
- American Diabetes Association. 2. Classification and diagnosis of Diabetes: Standards of medical care in Diabetes-2018. Diabetes Care. 2018; 41(Suppl 1):S13-27. [DOI:10.2337/dc18-S002] [PMID]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA. 2001; 285(19):2486-97. [DOI:10.1001/jama.285.19.2486] [PMID]
- Ayoade OG, Umoh I, Amadi C. Dyslipidaemia and associated risk factors among Nigerians with hypertension. Dubai Med J. 2020; 3(4):155-61. [DOI:10.1159/000509570]
- Amole IO, OlaOlorun AD, Owolabi AO. Prevalence of obesity and hypertension among adults in Ogbomoso, Nigeria. Internet J Med Update. 2011; 6(2):9-14. [DOI:10.4314/ijmu.v6i2.68186]
- Gierach M, Gierach J, Ewertowska M, Arndt A, Junik R. Correlation between Body Mass Index and Waist Circumference in Patients with Metabolic Syndrome. ISRN Endocrinol. 2014; 2014:514589. [DOI:10.1155/2014/514589] [PMID] [PMCID]
- Osei-Yeboah J, Kye-Amoah KK, Owiredu WKBA, Lokpo SY, Esson J, Bella Johnson B, et al. Cardiometabolic risk factors among healthcare workers: A cross-sectional study at the Sefwi-Wiawso Municipal Hospital, Ghana. Biomed Res Int. 2018; 2018:8904548. [DOI:10.1155/2018/8904548] [PMID] [PMCID]
- Cavagioni L, Pierin AM. [Cardiovascular risk among health professionals working in pre-hospital care services (Portuguese)]. Rev Esc Enferm USP. 2012; 46(2):395-403. [DOI:10.1590/S0080-62342012000200018] [PMID]
- Orozco-González CN, Cortés-Sanabria L, Viera-Franco JJ, Ramírez-Márquez JJ, Cueto-Manzano AM. [Prevalence of cardiovascular risk factors in a population of health-care workers (Spanish)]. Rev Med Inst Mex Seguro Soc. 2016; 54(5):594-601. [PMID]
- Ike SO, Onyema CT. Cardiovascular diseases in Nigeria: What has happened in the past 20 years? Nig J Cardiol. 2020; 17(1):21-6. [DOI:10.4103/njc.njc_33_19]
- Lawal Y, Muhammad S, Dahuwa UF, Bichi I, Ahmed H. Screening for obesity and undiscovered glucose intolerance among employees of a tertiary health centre in north-east Nigeria. J Health Res Rev. 2019; 6(3): 107-13. [DOI:10.4103/jhrr.jhrr_44_19]
- Bakari AG, Onyemelukwe GC. Glucose intolerance among apparently healthy Hausa-Fulani Northern Nigerians. Ann Afr Med. 2004; 3(1): 32-4. https://www.ajol.info/index.php/aam/article/view/8298
- Adeloye D, Auta A, Fawibe A, Gadanya M, Ezeigwe N, Mpazanje RG, et al. Current prevalence pattern of tobacco smoking in Nigeria: A systematic review and meta-analysis. BMC Public Health. 2019; 19(1):1719. [DOI:10.1186/s12889-019-8010-8] [PMID] [PMCID]
- Chukwuonye II, Chuku A, Onyeonoro UU, Okpechi IG, Madukwe OO, Umeizudike TI, et al. Prevalence of abdominal obesity in Abia State, Nigeria: Results of a population-based house-to-house survey. Diabetes Metab Syndr Obes. 2013; 6:285-91. [DOI:10.2147/DMSO.S43545] [PMID] [PMCID]
- Konin C, Kramoh E, Anzouan-Kacou JB, Essam N'Loo A, Yayé A, N'Djessan JJ, et al. [Diagnostic approach and treatment of hypertension in healthcare workers in Abidjan's district (Ivory Coast) (French)]. Rev Epidemiol Sante Publique. 2012; 60(1):41-6. [DOI:10.1016/j.respe.2011.07.006] [PMID]
- Akintunde AA, Salawu AA, Opadijo OG. Prevalence of traditional cardiovascular risk factors among staff of Ladoke Akintola University of Technology, Ogbomoso, Nigeria. Niger J Clin Pract. 2014; 17(6):750-5. [DOI:10.4103/1119-3077.144390] [PMID]
Article Type: Original Contributions |
Subject:
Public Health
Received: 2021/01/27 | Accepted: 2021/03/15 | Published: 2021/03/30
Received: 2021/01/27 | Accepted: 2021/03/15 | Published: 2021/03/30
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Contact Information
cjhr Office, Guilan University of Medical Sciences
P.O.Box 93345-41938, Rasht, Iran
Journal Tel: +9813 33335820
Publisher Tel: +9821 453 55 000
Email: cjhr.gums@gmail.com
