

Volume 10, Issue 1 (1-2025)
CJHR 2025, 10(1): 37-46 |
Back to browse issues page



Ethics code: IR.GUMS.REC.1401.476
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mohammadi Khanqah M, Bakhshi F, Ashouri A, Afkar A. Social Support Theory for Predicting Stress, Anxiety, and Job Burnout of Healthcare Workers in the Post-pandemic COVID-19. CJHR 2025; 10 (1) :37-46
URL: http://cjhr.gums.ac.ir/article-1-396-en.html
URL: http://cjhr.gums.ac.ir/article-1-396-en.html


1- Department of Health Education and Health Promotion, Health and Environment Research Center, Faculty of Health, Guilan University of Medical Sciences, Rasht, Iran.
2- Department of Health Education and Promotion, School of Health, Guilan University of Medical Sciences, Rasht, Iran. ,fa.bakhshi88@gmail.com
3- Department of Cardiology, Faculty of Medicine, Cardiovascular Diseases Research Center, Heshmat Hospital, Guilan University of Medical Sciences, Rasht, Iran.
4- Department of Health Education and Promotion, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
2- Department of Health Education and Promotion, School of Health, Guilan University of Medical Sciences, Rasht, Iran. ,
3- Department of Cardiology, Faculty of Medicine, Cardiovascular Diseases Research Center, Heshmat Hospital, Guilan University of Medical Sciences, Rasht, Iran.
4- Department of Health Education and Promotion, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
Full-Text [PDF 558 kb]
(475 Downloads)
| Abstract (HTML) (966 Views)
Full-Text: (511 Views)
Introduction
The COVID-19 pandemic disrupted multiple aspects of daily life, significantly impacting mental health, as people contend with stress, anxiety, job insecurity, and various social restrictions [1]. In China, for example, Wang et al. (2020) reported that 53.8% of respondents perceived the psychological impact of COVID-19 as moderate to severe, while 16.5% experiencing depression and 28.8% feeling anxious [2]. Such psychological effects have been particularly acute among healthcare workers, who face not only general societal stresses but also heightened workplace demands and health risks [3].
Healthcare workers play an essential role in sustaining healthcare systems, particularly during health crises. The unprecedented demands of the COVID-19 pandemic have placed them under considerable psychological strain, manifesting as increased stress, anxiety, and burnout, with a consequential impact on their mental health and job satisfaction [4]. Research indicates clear associations between epidemic outbreaks and heightened psychological issues such as health anxiety, stress, and post-traumatic stress disorder (PTSD), with healthcare workers being especially vulnerable [5]. In a study conducted in China, Liu et al. found that most healthcare professionals experienced symptoms of depression, anxiety, insomnia, and agitation during infectious disease outbreaks, highlighting the severe mental toll of such crises [6].
Given the mental health challenges associated with pandemic-related stresses, theories of behavior change, such as the social support theory, can help identify factors that influence resilience and psychological well-being. Social support is often defined as the exchange of emotional, informational, and instrumental resources within a social network, providing individuals with a sense of belonging and security. According to Sarafino (2011), social support encompasses the affection, respect, and care a person receives from family, friends, and others, and is linked to reduced psychological distress [7]. Social support functions through two main mechanisms: The “buffering effect”, which mitigates the psychological impact of stress, and the “direct effect model”, which enhances health and well-being independently of stress levels [8]. Social support can potentially buffer against genetic and environmental susceptibilities, enhancing resilience to stress. This effect might be mediated through its influence on the hypothalamic-pituitary-adrenal (HPA) axis, the noradrenergic system, and central oxytocin pathways [9].
Social support is conceptualized along structural and functional dimensions. Structural support involves objective aspects, such as membership in communities or networks, while functional support focuses on the qualitative aspects of social interactions [10]. Evidence suggests that adequate social support can mitigate the adverse psychological effects of stressors, including those induced by the pandemic, thus improving mental health outcomes for those exposed to extreme stressors, such as healthcare workers [11].
Despite extensive research on the psychological impact of the COVID-19 pandemic, there is a critical need to explore how specific factors, such as social support, can mitigate stress and burnout among healthcare workers, particularly in the context of understudied regions like Ardabil, Iran.
This study aims to identify predictors of workplace stress, anxiety, and burnout among healthcare workers at comprehensive health service centers in Ardabil, Iran, during the post-pandemic COVID-19 era. Using the framework of social support theory, this research examines how social support influence mental health and burnout among healthcare professionals in 2023.
Materials and Methods
Study design and participants
This cross-sectional study focused on healthcare workers employed in comprehensive health service centers in Ardabil County, Iran, who were actively engaged in health units during the COVID-19 pandemic. Assuming minimum correlation of 0.25 between social support and anxiety [12], 95% confidence level, power of 0.80, and a 10% non-response rate, the minimum required sample size was estimated at 136 participants. To ensure statistical power in regression analyses, the sample size was increased to 216, allowing for approximately 10 observations per independent variable. Stratified random sampling was used to select participants, based on job positions such as family health experts, midwives, nurses, supervisory nursing experts, liaison experts, laboratory experts, and nutritionists within the health centers in Ardabil County. Random numbers were generated using Excel, and healthcare workers were selected according to their job categories. Inclusion criteria were having at least six months of employment at a health center. Exclusion criteria included absence during the study period, incomplete survey responses, and self-reported mental illnesses.
Data collection
Data were collected using validated self-report questionnaire during December and March 2022.
Depression, anxiety, and stress scale (DASS-21)
The DASS-21 includes 21 items measuring depression, anxiety, and stress on a four-point Likert scale (0=“not at all” to 3=“extremely”). Each subscale’s scores are multiplied by two for comparison with the DASS-42, with higher scores indicating greater levels of psychological distress. Reliability coefficients in general populations for DASS-21 are 0.87 for depression, 0.85 for anxiety, and 0.89 for stress, while clinical sample coefficients are similar [13, 14]. The DASS-21 has demonstrated concurrent validity with the Beck depression inventory (r=0.70), Zung anxiety scale (r=0.67), and a perceived stress scale (r=0.49) [15]. It should be noted that in the present study, assessment of stress and anxiety was of interest, and only these subscales of the instrument were used.
Job burnout questionnaire
The job burnout questionnaire by Maslach and Jackson (1981) includes 22 items on a 7-point Likert scale, assessing emotional exhaustion, depersonalization, and lack of personal accomplishment. Subscale ranges are 0-54 for emotional exhaustion, 0-30 for depersonalization, and 0-48 for personal accomplishment, with higher scores indicating greater burnout. Reliability coefficients are 0.90 for emotional exhaustion, 0.79 for depersonalization, and 0.79 for personal accomplishment, supporting its validity [16].
Multidimensional scale of perceived social support (MSPSS)
The MSPSS is a short instrument designed to measure an individual’s perception of support from 3 sources: Family, friends and a significant other [17]. This 12-item scale ranges from 12 to 60, with scores categorized as low (12-20), moderate (21-40), and high (>40) social support. The MSPSS has a Cronbach’s α of 0.89 for the total scale, with subscale reliabilities of 0.85, 0.91, and 0.89 for family, friends, and significant others, respectively, indicating strong internal consistency [18].
Data analysis
Data were analyzed using SPSS software, version 22. Descriptive statistics were calculated, and data distribution was assessed using skewness, kurtosis, Q-Q plots, and normality tests. For normally distributed variables, independent samples t-tests, ANOVA, and Pearson correlation were applied; for non-normal variables, non-parametric tests such as Mann-Whitney U, Kruskal-Wallis, and Spearman’s rank correlation were used. Relationships between social support, stress, anxiety, and burnout were explored through Spearman’s correlation and regression models.
Three multiple linear regression models were used to examine predictors of stress, anxiety, and burnout. The regression models were adjusted for demographic variables as well as for factors such as COVID-19 infection history, hospitalization, and loss of family member due to COVID-19. The entry of demographic variables into each regression model was conducted using the stepwise method, and only significant variables were included in the final models. Assumptions of multicollinearity, homogeneity of variances, absence of residual autocorrelation, and normality of residuals were verified. A significance level of 0.05 was set for all statistical tests.
Results
Demographic characteristics
The demographic characteristics of the study participants are presented in Table 1.
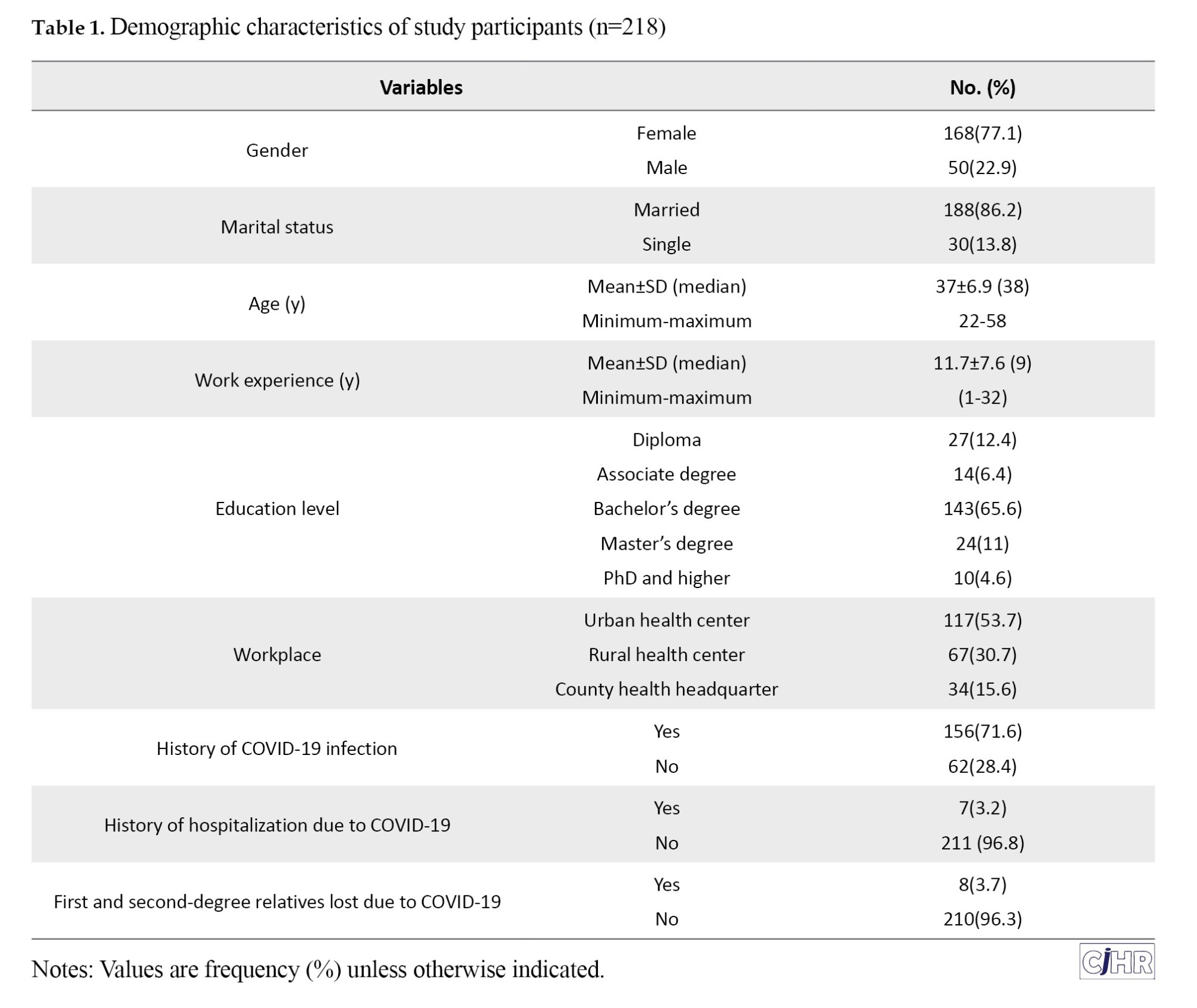
Of the total participants, 77% were women and 23% were men. The majority were married (86.2%), with a mean age of 37±6.9 years (range: 22–58 years). Participants had a mean of 9 years of work experience (range: 1–32 years), and most held a bachelor’s degree (65%). In terms of work location, 54% were employed in urban centers, 31% in rural centers, and 16% in county headquarters. A notable 72% of participants reported a history of COVID-19, 3.2% had been hospitalized due to the virus, and 7.3% reported the loss of a family member to COVID-19.
Psychological and social support scores
As shown in Table 2, the mean stress score was 9.11±5.64, the mean anxiety score was 6.44±5.23, and the mean job burnout score was 39.3±19.02.
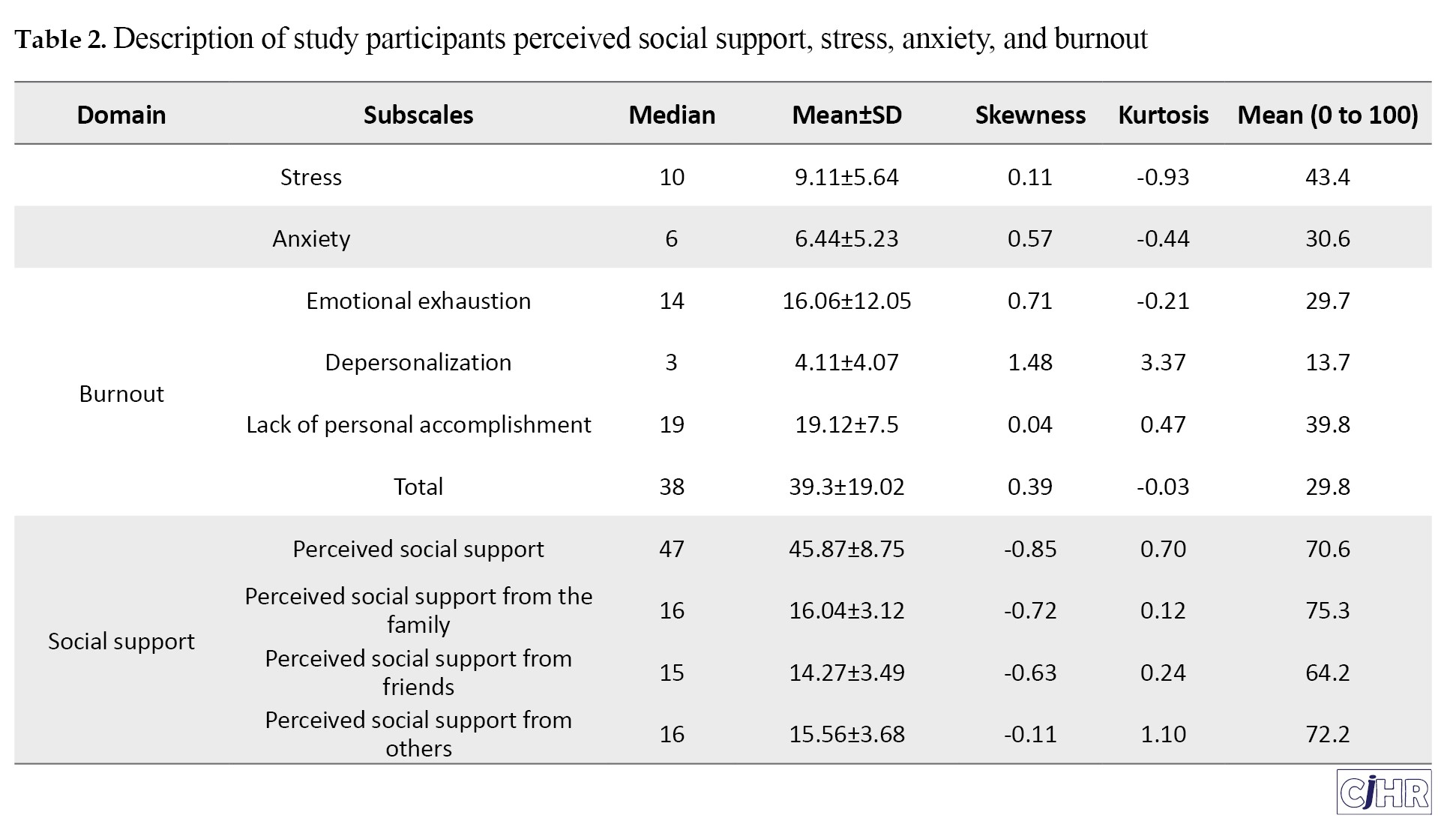
The mean perceived social support score was 47, with scores ranging from 20 to 60. On average, stress, anxiety, and job burnout scores were slightly below the midpoints of their respective scales, while perceived social support scores were slightly above average.
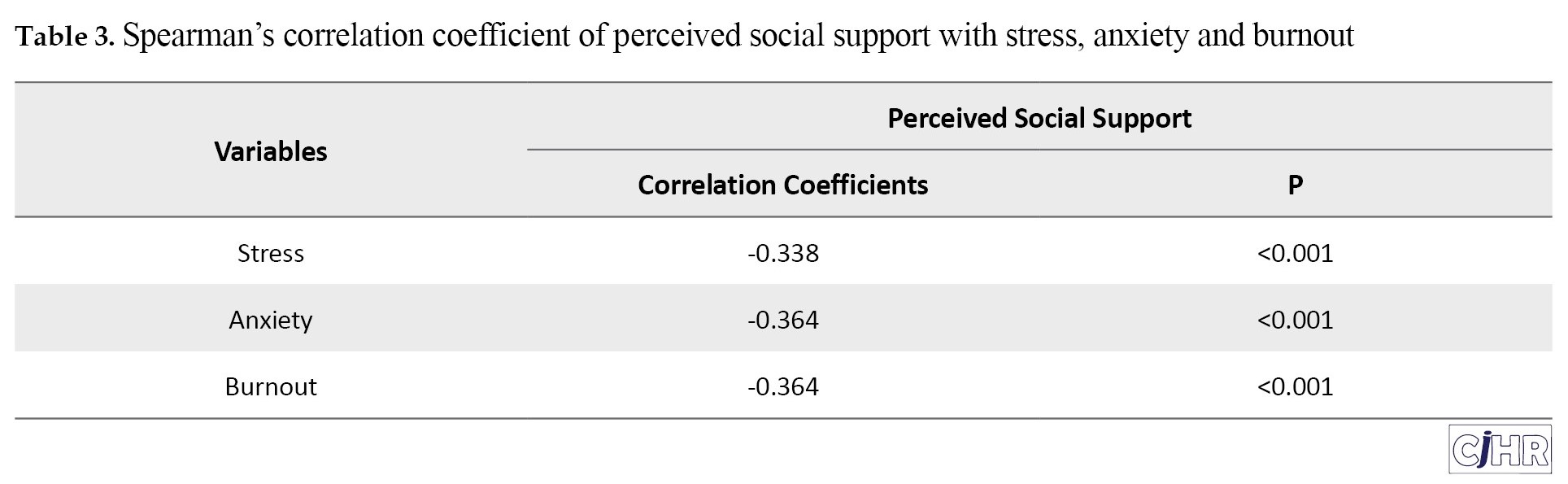
Correlations between social support, stress, anxiety, and burnout
Table 3 summarizes the correlation results, revealing a statistically significant moderate negative correlation between perceived social support and each psychological factor: Stress (r=-0.338, P<0.05), anxiety (r=-0.364, P<0.05), and job burnout (r=-0.364, P<0.05).
Additional analyses indicated that stress levels among healthcare workers were significantly associated with gender (P<0.001), age (P=0.029), years of service (P=0.011), service location (urban or rural, P<0.001), history of COVID-19 infection (P=0.029), and family loss due to COVID-19 (P=0.042).
Multiple regression analysis
Table 4 presents the findings of multiple linear regression analyses.
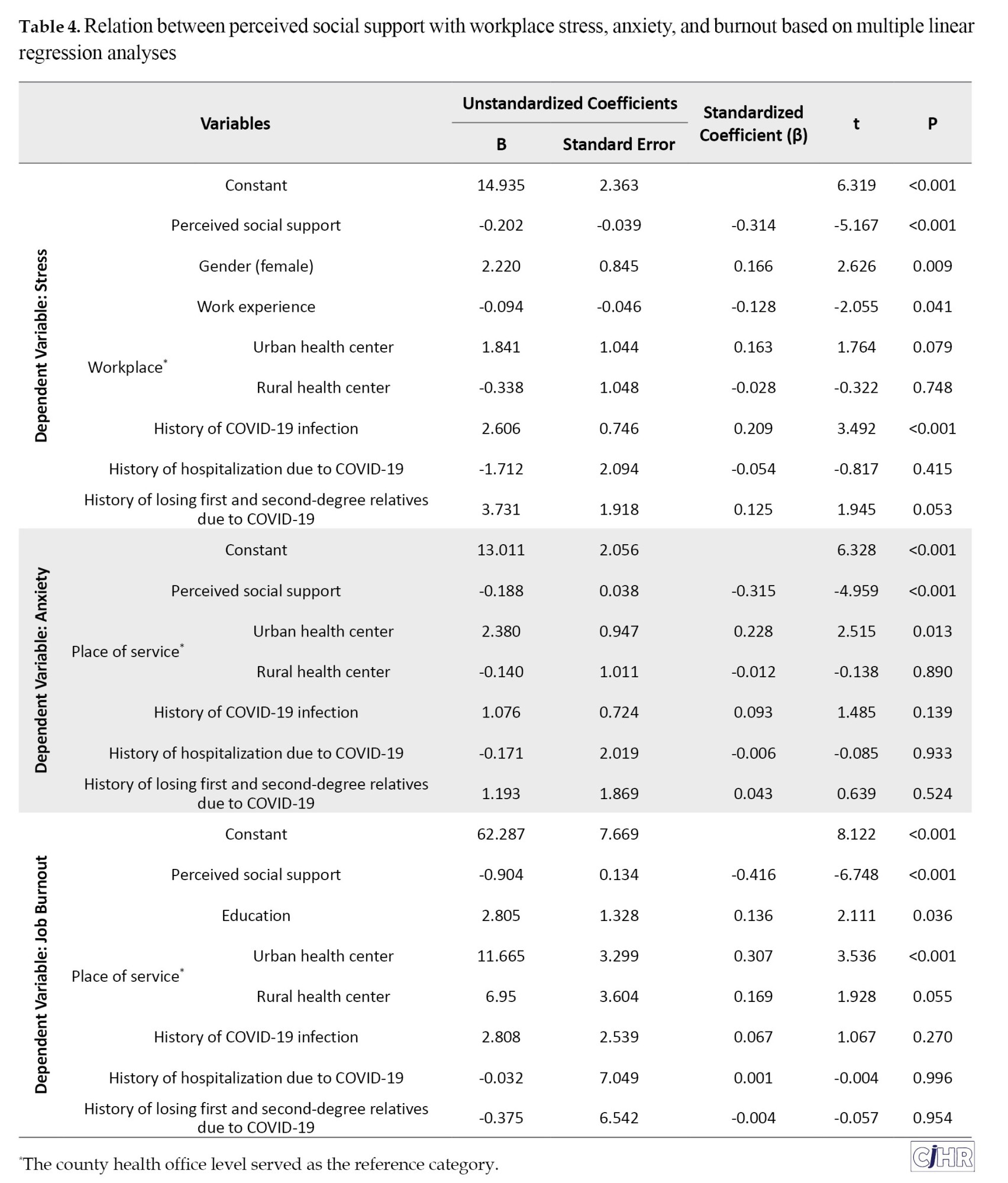
After adjusting for confounding factors, perceived social support remained significantly and negatively associated with stress (β=-0.202; 95% CI, -0.279%, -0.125%), anxiety (β=-0.188; 95% CI, -0.262%, -0.114%), and job burnout (β=-0.904; 95% CI, -1.167%, -0.642%), all with P<0.001.
In terms of demographic variables, the results of the multiple regression analyses indicated that female employees (P=0.009), those with less work experience (P=0.041), individuals who served in urban health centers compared to those in rural health centers (P=0.021) or county health headquarters (P=0.079), individuals with a history of COVID-19 infection (P<0.001), and those who lost family members due to COVID-19 (P=0.053) experienced higher scores of stress. Additionally, regarding anxiety, employees in urban health centers reported higher anxiety scores than those working in county health headquarters (P=0.013) or rural health centers (P<0.001). In terms of occupational burnout, employees with higher educational levels (P=0.036), as well as those serving in urban compared to those in county health headquarters (P<0.001) or rural health centers (P=0.086), reported higher scores of burnouts.
The coefficient of determination (R²) of the multiple regression models, which include significant demographic and confounding variables along with perceived social support accounted for 25% of the variance in stress, 16% in anxiety, and 23% in job burnout.
Discussion
The COVID-19 pandemic has exerted profound stress on healthcare workers, manifesting as increased fatigue, burnout, and diminished mental well-being due to heavy workloads, prolonged hours, heightened infection risks, and sometimes inadequate protective resources. As essential figures in public health, it is vital to assess the psychological impacts of these challenges and devise targeted interventions to support their mental health, as these psychological factors are key determinants of job performance [19, 20].
Our study found that healthcare workers reported below-average stress, anxiety, and job burnout in the post-pandemic period, in contrast to elevated levels reported in earlier pandemic-related studies [5, 11, 21, 22]. This reduction in stress and burnout may reflect the pandemic’s waning impact on workload intensity and psychological strain as healthcare systems began to stabilize.
The presence of higher stress in female employees and employees with less work experience is consistent with other studies [23, 24].
The higher stress among female employees and employees with less work experience is consistent with other studies. The results of Demir’s study also showed that women in the 20-30 age group with less work exerience experience more stress in their workplace and, although social support can be a solution to reduce their stress levels, they also seek less social support [25].
Another finding of this study was that stress, anxiety, and burnout were higher in people who worked in urban healthcare centers. Working in urban centers is inherently stressful due to the limited number of staff responsible for providing healthcare. The increased demand for care during COVID-19 is a reason for this increased workload and the resulting stress [26, 27]. There seems to be high healthcare demands in the post-COVID era.
A significant finding of this study is the moderate inverse correlation between perceived social support and levels of stress, anxiety, and job burnout, with correlation coefficients of -0.338, -0.364, and -0.364, respectively. Notably, perceived social support accounted for 25% of the variance in stress levels, underscoring its protective effect. This finding aligns with studies like those of Sun et al. (2023), who found perceived social support to be a crucial buffer against stress among nursing educators [28], and Bapolisi et al. (2022), which reported similar effects among Congolese healthcare workers during the pandemic [29].
Additional studies also corroborate the role of social support in reducing work-related stress and enhancing resilience [30, 31]. For example, Moosavian (2019) documented a negative association between social support and secondary traumatic stress in nurses [32], while Rostaminia and Hejazizadeh (2022) highlighted the link between quality of life, social support, and reduced job stress [33]. These findings, along with ours, reinforce the importance of emotional support systems within healthcare settings as protective factors against psychological distress.
In the context of COVID-19, social support has also been shown to moderate anxiety levels, as reported by Abdolahnezhad et al. (2021) [34]. Our results echo these findings, demonstrating that perceived social support explains 23% of the variance in job burnout. This emphasizes the essential role of social networks in buffering the adverse psychological effects of challenging work environments. Indeed, individuals with robust social connections reported lower stress, highlighting the potential of fostering workplace environments rich in social and emotional support.
Implications for practice
The findings underscore the value of perceived social support in mitigating stress and burnout among healthcare workers. Social support appears to bolster resilience and promote problem-solving coping strategies, reducing psychological distress [35]. The experience of the COVID-19 pandemic illustrates the need for healthcare organizations to re-evaluate and strengthen their support systems and management policies, ensuring healthcare workers’ mental health needs are met, enabling them to maintain optimal care quality.
Conclusion
The findings of this study highlight the enduring psychological challenges faced by healthcare workers in the aftermath of the COVID-19 pandemic and underscore the critical role of social support in mitigating stress, anxiety, and burnout. Despite the decline in reported stress levels compared to earlier pandemic phases, the moderate inverse correlations between perceived social support and psychological distress emphasize the protective value of strong social networks. These results align with existing literature, affirming that social support is a pivotal factor in promoting resilience and mental well-being among healthcare professionals.
Strengths and limitations
While much of the literature has focused on nurses, this study addressed a broader spectrum of healthcare workers, providing valuable insights into their mental health needs. However, the study has several limitations, including the use of convenient sampling methods, geographical constraints, and the self-reported nature of data, which may introduce biases and limit generalizability. Future research should aim to increase external validity by incorporating diverse populations across multiple regions and adopting randomized sampling approaches. Additionally, controlling for socio-economic factors could further enhance the findings.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Scientific and Ethical Committees of Guilan University of Medical Sciences, Rasht, Iran (Code: IR.GUMS.REC.1401.476).
Funding
The present article was extracted from the master’s thesis of Masoumeh Mohammadi Khanqah, approved by the Department of Health Education and Promotion, Faculty of Health, Guilan University of Medical Scienses, Rasht, Iran.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors extend their gratitude to all individuals and institutions contributing to the study.
References
The COVID-19 pandemic disrupted multiple aspects of daily life, significantly impacting mental health, as people contend with stress, anxiety, job insecurity, and various social restrictions [1]. In China, for example, Wang et al. (2020) reported that 53.8% of respondents perceived the psychological impact of COVID-19 as moderate to severe, while 16.5% experiencing depression and 28.8% feeling anxious [2]. Such psychological effects have been particularly acute among healthcare workers, who face not only general societal stresses but also heightened workplace demands and health risks [3].
Healthcare workers play an essential role in sustaining healthcare systems, particularly during health crises. The unprecedented demands of the COVID-19 pandemic have placed them under considerable psychological strain, manifesting as increased stress, anxiety, and burnout, with a consequential impact on their mental health and job satisfaction [4]. Research indicates clear associations between epidemic outbreaks and heightened psychological issues such as health anxiety, stress, and post-traumatic stress disorder (PTSD), with healthcare workers being especially vulnerable [5]. In a study conducted in China, Liu et al. found that most healthcare professionals experienced symptoms of depression, anxiety, insomnia, and agitation during infectious disease outbreaks, highlighting the severe mental toll of such crises [6].
Given the mental health challenges associated with pandemic-related stresses, theories of behavior change, such as the social support theory, can help identify factors that influence resilience and psychological well-being. Social support is often defined as the exchange of emotional, informational, and instrumental resources within a social network, providing individuals with a sense of belonging and security. According to Sarafino (2011), social support encompasses the affection, respect, and care a person receives from family, friends, and others, and is linked to reduced psychological distress [7]. Social support functions through two main mechanisms: The “buffering effect”, which mitigates the psychological impact of stress, and the “direct effect model”, which enhances health and well-being independently of stress levels [8]. Social support can potentially buffer against genetic and environmental susceptibilities, enhancing resilience to stress. This effect might be mediated through its influence on the hypothalamic-pituitary-adrenal (HPA) axis, the noradrenergic system, and central oxytocin pathways [9].
Social support is conceptualized along structural and functional dimensions. Structural support involves objective aspects, such as membership in communities or networks, while functional support focuses on the qualitative aspects of social interactions [10]. Evidence suggests that adequate social support can mitigate the adverse psychological effects of stressors, including those induced by the pandemic, thus improving mental health outcomes for those exposed to extreme stressors, such as healthcare workers [11].
Despite extensive research on the psychological impact of the COVID-19 pandemic, there is a critical need to explore how specific factors, such as social support, can mitigate stress and burnout among healthcare workers, particularly in the context of understudied regions like Ardabil, Iran.
This study aims to identify predictors of workplace stress, anxiety, and burnout among healthcare workers at comprehensive health service centers in Ardabil, Iran, during the post-pandemic COVID-19 era. Using the framework of social support theory, this research examines how social support influence mental health and burnout among healthcare professionals in 2023.
Materials and Methods
Study design and participants
This cross-sectional study focused on healthcare workers employed in comprehensive health service centers in Ardabil County, Iran, who were actively engaged in health units during the COVID-19 pandemic. Assuming minimum correlation of 0.25 between social support and anxiety [12], 95% confidence level, power of 0.80, and a 10% non-response rate, the minimum required sample size was estimated at 136 participants. To ensure statistical power in regression analyses, the sample size was increased to 216, allowing for approximately 10 observations per independent variable. Stratified random sampling was used to select participants, based on job positions such as family health experts, midwives, nurses, supervisory nursing experts, liaison experts, laboratory experts, and nutritionists within the health centers in Ardabil County. Random numbers were generated using Excel, and healthcare workers were selected according to their job categories. Inclusion criteria were having at least six months of employment at a health center. Exclusion criteria included absence during the study period, incomplete survey responses, and self-reported mental illnesses.
Data collection
Data were collected using validated self-report questionnaire during December and March 2022.
Depression, anxiety, and stress scale (DASS-21)
The DASS-21 includes 21 items measuring depression, anxiety, and stress on a four-point Likert scale (0=“not at all” to 3=“extremely”). Each subscale’s scores are multiplied by two for comparison with the DASS-42, with higher scores indicating greater levels of psychological distress. Reliability coefficients in general populations for DASS-21 are 0.87 for depression, 0.85 for anxiety, and 0.89 for stress, while clinical sample coefficients are similar [13, 14]. The DASS-21 has demonstrated concurrent validity with the Beck depression inventory (r=0.70), Zung anxiety scale (r=0.67), and a perceived stress scale (r=0.49) [15]. It should be noted that in the present study, assessment of stress and anxiety was of interest, and only these subscales of the instrument were used.
Job burnout questionnaire
The job burnout questionnaire by Maslach and Jackson (1981) includes 22 items on a 7-point Likert scale, assessing emotional exhaustion, depersonalization, and lack of personal accomplishment. Subscale ranges are 0-54 for emotional exhaustion, 0-30 for depersonalization, and 0-48 for personal accomplishment, with higher scores indicating greater burnout. Reliability coefficients are 0.90 for emotional exhaustion, 0.79 for depersonalization, and 0.79 for personal accomplishment, supporting its validity [16].
Multidimensional scale of perceived social support (MSPSS)
The MSPSS is a short instrument designed to measure an individual’s perception of support from 3 sources: Family, friends and a significant other [17]. This 12-item scale ranges from 12 to 60, with scores categorized as low (12-20), moderate (21-40), and high (>40) social support. The MSPSS has a Cronbach’s α of 0.89 for the total scale, with subscale reliabilities of 0.85, 0.91, and 0.89 for family, friends, and significant others, respectively, indicating strong internal consistency [18].
Data analysis
Data were analyzed using SPSS software, version 22. Descriptive statistics were calculated, and data distribution was assessed using skewness, kurtosis, Q-Q plots, and normality tests. For normally distributed variables, independent samples t-tests, ANOVA, and Pearson correlation were applied; for non-normal variables, non-parametric tests such as Mann-Whitney U, Kruskal-Wallis, and Spearman’s rank correlation were used. Relationships between social support, stress, anxiety, and burnout were explored through Spearman’s correlation and regression models.
Three multiple linear regression models were used to examine predictors of stress, anxiety, and burnout. The regression models were adjusted for demographic variables as well as for factors such as COVID-19 infection history, hospitalization, and loss of family member due to COVID-19. The entry of demographic variables into each regression model was conducted using the stepwise method, and only significant variables were included in the final models. Assumptions of multicollinearity, homogeneity of variances, absence of residual autocorrelation, and normality of residuals were verified. A significance level of 0.05 was set for all statistical tests.
Results
Demographic characteristics
The demographic characteristics of the study participants are presented in Table 1.
Of the total participants, 77% were women and 23% were men. The majority were married (86.2%), with a mean age of 37±6.9 years (range: 22–58 years). Participants had a mean of 9 years of work experience (range: 1–32 years), and most held a bachelor’s degree (65%). In terms of work location, 54% were employed in urban centers, 31% in rural centers, and 16% in county headquarters. A notable 72% of participants reported a history of COVID-19, 3.2% had been hospitalized due to the virus, and 7.3% reported the loss of a family member to COVID-19.
Psychological and social support scores
As shown in Table 2, the mean stress score was 9.11±5.64, the mean anxiety score was 6.44±5.23, and the mean job burnout score was 39.3±19.02.
The mean perceived social support score was 47, with scores ranging from 20 to 60. On average, stress, anxiety, and job burnout scores were slightly below the midpoints of their respective scales, while perceived social support scores were slightly above average.
Correlations between social support, stress, anxiety, and burnout
Table 3 summarizes the correlation results, revealing a statistically significant moderate negative correlation between perceived social support and each psychological factor: Stress (r=-0.338, P<0.05), anxiety (r=-0.364, P<0.05), and job burnout (r=-0.364, P<0.05).
Additional analyses indicated that stress levels among healthcare workers were significantly associated with gender (P<0.001), age (P=0.029), years of service (P=0.011), service location (urban or rural, P<0.001), history of COVID-19 infection (P=0.029), and family loss due to COVID-19 (P=0.042).
Multiple regression analysis
Table 4 presents the findings of multiple linear regression analyses.
After adjusting for confounding factors, perceived social support remained significantly and negatively associated with stress (β=-0.202; 95% CI, -0.279%, -0.125%), anxiety (β=-0.188; 95% CI, -0.262%, -0.114%), and job burnout (β=-0.904; 95% CI, -1.167%, -0.642%), all with P<0.001.
In terms of demographic variables, the results of the multiple regression analyses indicated that female employees (P=0.009), those with less work experience (P=0.041), individuals who served in urban health centers compared to those in rural health centers (P=0.021) or county health headquarters (P=0.079), individuals with a history of COVID-19 infection (P<0.001), and those who lost family members due to COVID-19 (P=0.053) experienced higher scores of stress. Additionally, regarding anxiety, employees in urban health centers reported higher anxiety scores than those working in county health headquarters (P=0.013) or rural health centers (P<0.001). In terms of occupational burnout, employees with higher educational levels (P=0.036), as well as those serving in urban compared to those in county health headquarters (P<0.001) or rural health centers (P=0.086), reported higher scores of burnouts.
The coefficient of determination (R²) of the multiple regression models, which include significant demographic and confounding variables along with perceived social support accounted for 25% of the variance in stress, 16% in anxiety, and 23% in job burnout.
Discussion
The COVID-19 pandemic has exerted profound stress on healthcare workers, manifesting as increased fatigue, burnout, and diminished mental well-being due to heavy workloads, prolonged hours, heightened infection risks, and sometimes inadequate protective resources. As essential figures in public health, it is vital to assess the psychological impacts of these challenges and devise targeted interventions to support their mental health, as these psychological factors are key determinants of job performance [19, 20].
Our study found that healthcare workers reported below-average stress, anxiety, and job burnout in the post-pandemic period, in contrast to elevated levels reported in earlier pandemic-related studies [5, 11, 21, 22]. This reduction in stress and burnout may reflect the pandemic’s waning impact on workload intensity and psychological strain as healthcare systems began to stabilize.
The presence of higher stress in female employees and employees with less work experience is consistent with other studies [23, 24].
The higher stress among female employees and employees with less work experience is consistent with other studies. The results of Demir’s study also showed that women in the 20-30 age group with less work exerience experience more stress in their workplace and, although social support can be a solution to reduce their stress levels, they also seek less social support [25].
Another finding of this study was that stress, anxiety, and burnout were higher in people who worked in urban healthcare centers. Working in urban centers is inherently stressful due to the limited number of staff responsible for providing healthcare. The increased demand for care during COVID-19 is a reason for this increased workload and the resulting stress [26, 27]. There seems to be high healthcare demands in the post-COVID era.
A significant finding of this study is the moderate inverse correlation between perceived social support and levels of stress, anxiety, and job burnout, with correlation coefficients of -0.338, -0.364, and -0.364, respectively. Notably, perceived social support accounted for 25% of the variance in stress levels, underscoring its protective effect. This finding aligns with studies like those of Sun et al. (2023), who found perceived social support to be a crucial buffer against stress among nursing educators [28], and Bapolisi et al. (2022), which reported similar effects among Congolese healthcare workers during the pandemic [29].
Additional studies also corroborate the role of social support in reducing work-related stress and enhancing resilience [30, 31]. For example, Moosavian (2019) documented a negative association between social support and secondary traumatic stress in nurses [32], while Rostaminia and Hejazizadeh (2022) highlighted the link between quality of life, social support, and reduced job stress [33]. These findings, along with ours, reinforce the importance of emotional support systems within healthcare settings as protective factors against psychological distress.
In the context of COVID-19, social support has also been shown to moderate anxiety levels, as reported by Abdolahnezhad et al. (2021) [34]. Our results echo these findings, demonstrating that perceived social support explains 23% of the variance in job burnout. This emphasizes the essential role of social networks in buffering the adverse psychological effects of challenging work environments. Indeed, individuals with robust social connections reported lower stress, highlighting the potential of fostering workplace environments rich in social and emotional support.
Implications for practice
The findings underscore the value of perceived social support in mitigating stress and burnout among healthcare workers. Social support appears to bolster resilience and promote problem-solving coping strategies, reducing psychological distress [35]. The experience of the COVID-19 pandemic illustrates the need for healthcare organizations to re-evaluate and strengthen their support systems and management policies, ensuring healthcare workers’ mental health needs are met, enabling them to maintain optimal care quality.
Conclusion
The findings of this study highlight the enduring psychological challenges faced by healthcare workers in the aftermath of the COVID-19 pandemic and underscore the critical role of social support in mitigating stress, anxiety, and burnout. Despite the decline in reported stress levels compared to earlier pandemic phases, the moderate inverse correlations between perceived social support and psychological distress emphasize the protective value of strong social networks. These results align with existing literature, affirming that social support is a pivotal factor in promoting resilience and mental well-being among healthcare professionals.
Strengths and limitations
While much of the literature has focused on nurses, this study addressed a broader spectrum of healthcare workers, providing valuable insights into their mental health needs. However, the study has several limitations, including the use of convenient sampling methods, geographical constraints, and the self-reported nature of data, which may introduce biases and limit generalizability. Future research should aim to increase external validity by incorporating diverse populations across multiple regions and adopting randomized sampling approaches. Additionally, controlling for socio-economic factors could further enhance the findings.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Scientific and Ethical Committees of Guilan University of Medical Sciences, Rasht, Iran (Code: IR.GUMS.REC.1401.476).
Funding
The present article was extracted from the master’s thesis of Masoumeh Mohammadi Khanqah, approved by the Department of Health Education and Promotion, Faculty of Health, Guilan University of Medical Scienses, Rasht, Iran.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors extend their gratitude to all individuals and institutions contributing to the study.
References
- Sadeghi Yarandi M, Gholami A, Ghasemi M, Sadeghi Yarandi M, Ghasemi Koozekonan A, Soltanzadeh A. [Investigating the psychological consequences of the COVID-19 outbreak in the occupational society (Persian)]. J Mil Med. 2020; 22(6):562-9. [DOI:10.30491/JMM.22.6.562]
- Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020; 17(5):1729. [DOI:10.3390/ijerph17051729] [PMID]
- Wheaton MG, Abramowitz JS, Berman NC, Fabricant LE, Olatunji BO. Psychological predictors of anxiety in response to the H1N1 (swine flu) pandemic. Cogn Ther Res. 2012; 36:210-8. [DOI:10.1007/s10608-011-9353-3]
- Roohafzaei S, AbediKooshki S, Gholami Moghadam A. [The role of job stress on the productivity of nurses working in the corona ward of Imam Khomeini Esfarayen hospital (Persian)]. Q J Nurs Manage. 2021; 10(2):1-10. [Link]
- Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet. 2020; 395(10227):912-20. [DOI:10.1016/S0140-6736(20)30460-8] [PMID]
- Liu N, Zhang F, Wei C, Jia Y, Shang Z, Sun L, et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Res. 2020; 287:112921. [DOI: 10.1016/j.psychres.2020.112921] [PMID]
- Sarafino EP. Applied behavior analysis: Principles and procedures in behavior modification. Hoboken: John Wiley & Sons; 2011. [Link]
- Locher JL, Ritchie CS, Roth DL, Baker PS, Bodner EV, Allman RM. Social isolation, support, and capital and nutritional risk in an older sample: Ethnic and gender differences. Soc Sci Med. 2005; 60(4):747-61. [DOI:10.1016/j.socscimed.2004.06.023] [PMID]
- Ozbay F, Johnson DC, Dimoulas E, Morgan CA, Charney D, Southwick S. Social support and resilience to stress: From neurobiology to clinical practice. Psychiatry (Edgmont). 2007; 4(5):35-40. [PMID]
- Riahi M E, Aliverdinia A, Pourhossein Z. [Relationship between social support and mental health (Persian)]. Soc Welf Q. 2011; 10(39):85-121. [Link]
- Ashcroft R, Donnelly C, Lam S, Kourgiantakis T, Adamson K, Verilli D, et al. Qualitative examination of collaboration in team-based primary care during the COVID-19 pandemic. BMJ Open. 2023; 13(2):e067208. [DOI:10.1136/bmjopen-2022-067208] [PMID]
- Eyni S, Ebadi M, Hashemi Z. [Corona anxiety in nurses: The predictive role of perceived social support and sense of coherence (Persian)]. Iran J Psychiatry Clin Psychol. 2020; 26(3):320-31. [DOI:10.32598/ijpcp.26.3436.1]
- Lovibond PF, Lovibond SH. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995; 33(3):335-43. [DOI:10.1016/0005-7967(94)00075-U] [PMID]
- Najafi Kalyani M, Pourjam E, Jamshidi N, Karimi S, Najafi Kalyani V. [Survey of stress, anxiety, depression and self-concept of students of Fasa University of medical sciences, 2010 (Persian)]. J Fasa Univ Med Sci. 2013; 3(3):235-40. [Link]
- Sahebi A, Asghari M, Salari S. Validation of the Stress Anxiety Depression Scale (DASS-21) for the Iranian population. Transformational Psychology: Iranian Psychologists. 2005; 1(4):36-54. [Link]
- Grossi S, Khodaparast Z. [The relationship between functional social support and quality of life amongst married women after childbirth in Kerman city (Case: Women referred to health centers) (Persian)]. Iran J Soc Stud. 2014; 8(2):104-27. [Link]
- Zimet GD, Powell SS, Farley GK, Werkman S, Berkoff KA. Psychometric characteristics of the multidimensional scale of perceived social support. J Pers Assess. 1990; 55(3-4):610-7. [DOI: 10.1080/00223891.1990.9674095] [PMID]
- Wongpakaran T, Wongpakaran N, Ruktrakul R. Reliability and validity of the multidimensional scale of perceived social support (MSPSS): Thai version. Clin Pract Epidemiol Ment Health. 2011; 7:161-6. [DOI:10.2174/1745017901107010161] [PMID]
- Ashoori J. [Prediction of nurse’s job burnout based on social capital, perceived social support, and organizational citizenship behavior (Persian)]. Pajouhan Sci J. 2017; 15(2):13-9. [Link]
- Khademian F, Delavari S, Koohjani Z, Khademian Z. An investigation of depression, anxiety, and stress and its relating factors during COVID-19 pandemic in Iran. BMC Public Health. 2021; 21(1):275. [DOI:10.1186/s12889-021-10329-3] [PMID]
- Corlade-Andrei M, Măirean C, Nedelea P, Grigorasi G, Cimpoesu D. Burnout syndrome among staff at an emergency department during the COVID-19 pandemic. Healthcare (Basel). 2022; 10(2):258. [DOI:10.3390/healthcare10020258] [PMID]
- Fazaeli S, Yousefi M, Jamali J, Ebrahimi Z, Hemati M. Evaluation of the relationship between occupational stress and hospital support among nurses caring for covid-19 patients: Comparison between nurses with experience of patient care in infectious and non-infectious wards. Iran Red Crescent Med J. 2021; 23(5):e366. [Link]
- Monnat SM. Rural-urban variation in COVID-19 experiences and impacts among US working-age adults. Ann Am Acad Polit Soc Sci. 2021; 698(1):111-36. [DOI:10.1177/00027162211069717]
- Çelmeçe N, Menekay M. The effect of stress, anxiety and burnout levels of healthcare professionals caring for COVID-19 patients on their quality of life. Front Psychol. 2020; 11:597624. [Link]
- Demir M. Stress experienced by female employees at workplace; symptoms, sources of stress, ways to deal with these sources of stress. Turk Online J Educ Technol. 2024; 23(3):73-82. [Link]
- Kelly D, Schroeder S, Leighton K. Anxiety, depression, stress, burnout, and professional quality of life among the hospital workforce during a global health pandemic. J Rural Health. 2022; 38(4):795-804. [DOI:10.1111/jrh.12659] [PMID]
- Ding Y, Qu J, Yu X, Wang S. The mediating effects of burnout on the relationship between anxiety symptoms and occupational stress among community healthcare workers in China: A cross-sectional study. Plos One. 2014; 9(9):e107130. [DOI:10.1371/journal.pone.0107130] [PMID]
- Sun X, Yin H, Liu C, Zhao F. Psychological capital and perceived supervisor social support as mediating roles between role stress and work engagement among Chinese clinical nursing teachers: A cross-sectional study. BMJ Open. 2023; 13(8):e073303. [DOI:10.1136/bmjopen-2023-073303] [PMID]
- Bapolisi A, Maurage P, Rubambura RB, Tumaini HM, Baguma M, Cikomola C, et al. Psychopathological states among Congolese health workers during the first wave of COVID-19 pandemic: Links with emotion regulation and social support. Eur J Psychotraumatol. 2022; 13(2):2101346. [DOI:10.1080/20008198.2022.2101346] [PMID]
- Shi LS, Xu RH, Xia Y, Chen DX, Wang D. The impact of COVID-19-related work stress on the mental health of primary healthcare workers: the mediating effects of social support and resilience. Front Psychol. 2022; 12:800183. [DOI:10.3389/fpsyg.2021.800183] [PMID]
- Karadaş A, Duran S. The effect of social support on work stress in health workers during the pandemic: The mediation role of resilience. J Community Psychol. 2022; 50(3):1640-9. [DOI:10.1002/jcop.22742] [PMID]
- Moosavian Khorasani SH, Vagharseyyein SA, Zarei B, Shafiee F. [Association of perceived social support with secondary traumatic stress and perceived stress in nurses (Persian)]. Sci J Nurs Midwifery Paramed Fac. 2019; 5(2):68-80. [Link]
- Rostaminia M, Hejazizadeh G. Comparison of quality of life, job stress, and social support among employees of the ministry of health and medical education. islamic life style. 2022; 6(0): 208-20. [Link]
- Abdolahnezhad F, Andam R, Rajabi M. [The impact of COVID 19 concerns on the mental health of athlete students with the modifying role of social support in a multi-group analysis by gender (Persian)]. Qom Univ Med Sci J. 2021; 15(3):198-209. [DOI:10.52547/qums.15.3.198]
- Marler EK, Bruce MJ, Abaoud A, Henrichsen C, Suksatan W, Homvisetvongsa S, et al. The impact of COVID-19 on university students’ academic motivation, social connection, and psychological well-being. Scholarsh Teach Learn Psychol. 2024; 10(3):320-30. [DOI:10.1037/stl0000294]
Article Type: Original Contributions |
Subject:
Health Education and Promotion
Received: 2024/11/15 | Accepted: 2024/12/13 | Published: 2025/01/29
Received: 2024/11/15 | Accepted: 2024/12/13 | Published: 2025/01/29
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
